 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
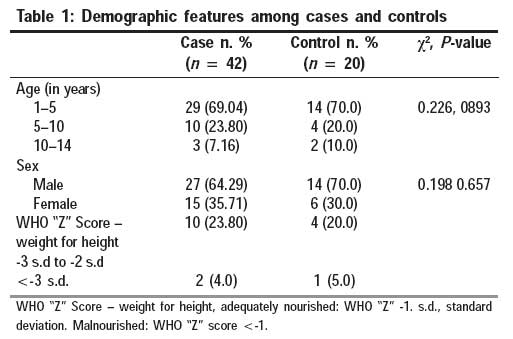
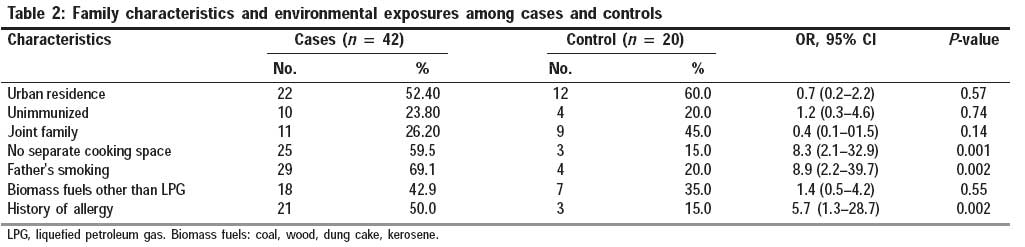
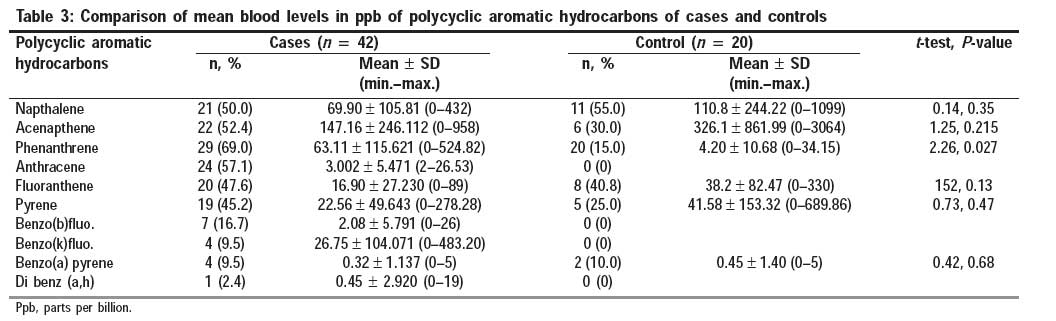
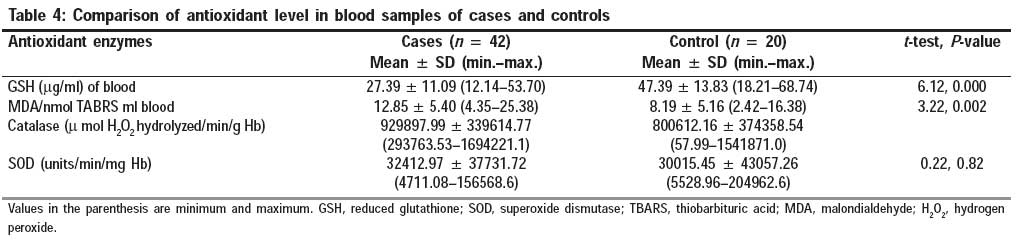
Indian Journal of Occupational and Environmental Medicine, Vol. 13, No. 1, January-April, 2009, pp. 33-37 Original Article Assessment of association of exposure to polycyclic aromatic hydrocarbons with bronchial asthma and oxidative stress in children: A case control study Suresh Ram, Awasthi Shally, Mahdi AA, Patel DK, Singh VK, Rita Misra Department of Pediatrics, Chhatrapati Shahuji Maharaj Medical University, Lucknow - 226 003, UP Code Number: oe09008 Abstract Background: Polycyclic aromatic hydrocarbons (PAH) originate from the incomplete combustion of organic matter and ambient air pollution by these is increasing. There is also an increase in the global prevalence of asthma, for which environmental pollution has been recognized as one of the important factors. Exposure to pollutants and other allergens induces chronic airway inflammation by generation of reactive oxygen species, causing oxidative stress. Therefore, the objective of the present study was to assess association, if any, between exposure to PAH and asthma as well as oxidative stress in children.Method: In this hospital-based case control study, cases of bronchial asthma aged 1-14 years and healthy matched controls were included. Oxidative stress was measured by assessing the levels of enzymes catalase, superoxide dismutase, malondialdehyde (MDA), and reduced glutathione (GSH). Results : Forty-two cases and 20 controls were enrolled. Mean blood level of phenanthrene, a PAH, was 63.11 ppb ± 115.62 and 4.20 ppb ± 10.68 ppb in cases and controls, respectively ( P = 0.02). Mean blood levels of GSH was significantly lower in cases and controls (27.39 mg/ml ± 11.09 versus 47.39 g/ml ± 13.83; P -value = 0.001). Likewise, mean blood level of MDA in nanomole/ml was significantly higher in asthma as compared with controls (12.85 ± 5.40 versus 8.19 ± 5.16; P -value = 0.002), suggestive of increased oxidative stress. Conclusions: Because elevated blood level of phenanthrene is associated with bronchial asthma as well as with oxidative stress, measures to reduce exposure to PAH may possibly lead to reduced incidence and severity of bronchial asthma. Keywords: Asthma, children, India, phenanthrene, polycyclic aromatic hydrocarbons, oxidative stress Introduction Asthma is the most common inflammatory lung disease in children and is a major public health problem, showing steady increases in prevalence both in developing and in developed countries. [1] Globally, 150 million people are suffering from asthma. [2] In India, there is wide variation (4-19%) in the prevalence of asthma in school going children from different geographic areas. [3] About half to one-third of the cases of asthma have been associated with ambient air pollution. [4] Exposure to polycyclic aromatic hydrocarbons (PAH) as a result of ambient air pollution has also been associated with asthma. PAH are a group of small organic compounds of three to five benzene rings that are formed during the incomplete combustion of coal, oil, gas wood garbage, or other substances, such as tobacco. [5] Our hypothesis was that exposure to PAH results in an oxidative stress in the respiratory tract, which may stimulate the redox cycle and generate reactive oxygen species, resulting in exacerbation of airway inflammation and manifesting as asthma. [6] The objective of the current study was to assess the association, if any, between exposure to PAH and bronchial asthma along with evidence of oxidative stress, as assessed by levels of antioxidant enzymes catalase (CAT), superoxide dismutase (SOD), glutathione (GSH), and malondialdehyde (MDA). [7] Materials and Methods Study design This was a hospital-based case control study carried out after obtaining institutional ethical clearance in a tertiary care hospital in Lucknow, northern India, from August 2005 to July 2006. Subjects Inclusion criteria for cases were clinical diagnosis of bronchial asthma, defined as a history of more than three episodes of documented wheeze in a year. [8] Inclusion criteria for controls was no history of asthma or any concomitant respiratory problem and were age, sex, weight for height (World Health Organization Z score), and residential area matched healthy children. Excluded were cases and controls with congenital heart disease, chronic lung disease like suspected cystic fibrosis, bronchiectasis, lung abscess, or whose parents or guardian did not consent to participation. Sample size calculation To assess exposure of 50% and 10% of cases and controls, respectively, to any PAH with an alpha level of 0.05 and power of 0.8 with a 2:1 ratio of cases to controls, 18 controls and 37 cases were to be recruited. Variables for data collection and definition Data were collected on age, sex, anthropometry, weight, height, family characteristics, residential area, immunization status, history of allergy, family history of asthma, and surrogate markers of exposure to environmental pollutants, like number of rooms in house, separate cooking space, use of biomass fuels for cooking, smoking status of parents, distance of residence from heavy traffic, and industrial factory in near by area. Exposure to PAH and measurement of oxidative stress were assessed by biochemical analyses of venous blood. Biochemical analysis Approximately 5.0 ml of venous blood was withdrawn from all subjects and was stored in pre-heparinized glass vials. Samples were coded and transported under ice-cold conditions to the Analytical Toxicology Lab, Industrial Toxicology Research Centre, Lucknow, for analysis of PAH and antioxidant enzymes. The analytical toxicologist was totally blind to the medical history and final diagnosis of the subjects. Two milliliters of blood was used for the preparation of the lysate. Blood was centrifuged at 2500 g for 15 min at 4°C and the supernatant was aspirated. The erythrocyte-rich precipitate was washed three times with ice-cold physiological saline (3:1 v/v) and lysed by double distilled water. The particulate material was centrifuged at 15,000 g for 90 min at 4 0 C and the supernatant (erythrocyte lysine) was collected for determination of CAT and SOD activity. Three milliliters of blood was utilized for the estimation of MDA, GSH, and PAHs levels. Analyses of PAH Extraction of PAH from blood was carried out according to Van Scooten et al. [9] Peak confirmation of PAHs in blood samples was performed by gas chromatography (mass spectrometer using model auto system XL [Perkin-Elmer Waltham, Massachusetts, USA] coupled with a Turbo Mass detector). The sample was reduced to 0.5 ml under a gentle stream of nitrogen and analyzed on an HPLC-FD at a reverse phased (RP) C - 18 ODS analytical column (75 mm x 4.6 mm i.d., 3.5 mm particle size), with a pre-column of the same phase from Waters (Water Milford, MA, USA) for different PAHs other than acenaphthylene (due to no response by FD). The elution conditions and detection wavelength program was same as that reported by Barranco et al. [10] Recovery experiments were conducted to check the analytical quality control. Samples of blood were spiked with a mix standard of 16 PAHs and the recoveries ranged from 78 to 94% for all PAH compounds. Gas Chromatography conditions and temperature programming was same as described by Poon et al. [11] The mass detector was operated in an electron impact at 70 eV in full scan. The target compounds were identified in the scanning mode. The spectrum of individual PAH was confirmed by matching it with the authentic spectra of standard PAH in the list library available in the GC-MS instrument Perkin-Elmer Waltham, Massachusetts, USA. According to the Environmental Protection Agency priority list, the following PAH were studied: naphthalene, acenapthene, phenanthrene, anthracene, fluoranthene, pyrene, benzo (b) fluo, benzo (k) fluo, benzo (a) pyrene, di benzo (a,h) anthracene. Estimation of antioxidant enzymes The extent of lipid peroxidation was estimated by measuring the formation of MDA by the reaction of MDA with thiobarbituric acid and expressed as nmol MDA/ml blood, using a molar extinction coefficient of 1.56 x l0 5 M−1 cm−1 . [12] Reduced GSH was estimated in the whole blood using Ellman′s reagent and expressed as µmol/ml of blood. [13] CAT activity was determined using hydrogen peroxide (H 2 O 2 ) as substrate and expressed as µmol H 2 O 2 decomposed/min/g hemoglobin (Hb). [14] SOD activity determination was carried out by the method of Mishra et al. [15] Data management Data were entered in MS-Excel 2000. Statistical analysis was performed using the Statistical Package for Social Sciences for windows (SPSS-Version 11, Chicago, Illinois, USA ). Univariate analysis was performed to study the frequency distribution of the variables. χ2 and Students t-test were used to test the association between categorical and continuous variables, respectively. The Kruskal Wallis test, a non parametric test equivalent to one way ANOVA (F test), was used to check whether the mean level of PAH differs significantly among cases and controls. In order to asses the effects of PAH exposure by different sources and other potential risk factors for asthma, the crude odds ratio (OR) with 95% confidence interval (CI) was calculated. For those variables that had a univariate association with asthma, multivariate logistic regression analysis was performed to calculate the adjusted OR with 95% CI. Statistical inferences were based on the conventional level of statistical significance (P < 0.05). Results Sixty-two children, 42 cases of bronchial asthma and 20 controls, were included. Demographic features are given in [Table - 1]. The male to female ratio was 1.9:1. Family characteristics and environmental exposures among cases and control are given in [Table - 2]. Non-availability of separate cooking space, father smoking status, and history of allergy were positively associated with asthma. Family type, use of biomass fuels, and residential area distribution was not significantly associated with case control status. Proportion of cases and controls positive for PAH in blood samples as well as their mean levels are given in [Table - 3]. Mean blood level of phenanthrene was statistically significantly higher in cases (63.11 ppb ± 115.62) as compared with controls (4.20 ppb ± 10.68; P = 0.02). Comparison of mean blood levels of antioxidant enzymes, CAT, and SOD, as well as GSH and MDA between asthma and controls is given in [Table - 4]. Mean levels of GSH in blood were significantly lower in cases as compared with controls. Mean level of MDA in nanomole/ml was significantly higher in asthma as compared with controls. Mean blood levels of CAT and SOD were similar among cases and controls. Multivariate conditional logistic regression analysis was performed to assess the association of blood PAH and oxidative stress with case control status, controlling for other variables that either had a univariate association with it or were clinically meaningful or could be potentially modified. Variables associated with bronchial asthma were father smoking status (adjusted OR = 7.4, 95% Cl: 1.2-43.7; P = 0.03), mean blood levels of phenanthrene (adjusted OR = 13.3, 95% Cl: 1.9-88.5; P = 0.008), and GSH (adjusted OR = 0.8, 95% Cl: 0.8-0.9; P = 0.001). Discussion In the present study, we assessed the exposure to PAH by estimating their levels in blood and also evaluated their possible association with bronchial asthma as well as with oxidative stress. We found a higher blood level of phenanthrene as well as evidence of oxidative stress, in the form of reduced blood level of GSH and elevated blood MDA level, in cases of bronchial asthma when compared with matched controls. As reported earlier, we also found a significant association of asthma with non-availability of separate cooking space and smoking status of father, both of which cause indoor air pollution along with exposure to PAH. [16],[17],[18] Several studies have also documented increased prevalence of asthma by indoor air pollution using unprocessed biomass fuels. [3],[18],[19],[20] Use of unprocessed biomass fuels is a major determinant of indoor air pollution. However, we have not found an association between the uses of biomass fuels with asthma, possibly because of small sample size due to different types of biomass fuels used here. However, ambient air pollution through biomass fuel use is aggravated if there is inadequate ventilation, as found in households that do not have a separate cooking space, which has been found to be associated with asthma in our study. Likewise, we have not found an association of asthma with urban residence, as reported earlier by others. [21] Because there are no standard guidelines or available data that determine the minimal risk level for a particular PAH for any duration of exposure, any amount of PAH detected in the blood sample was considered as positive by us. In the present study, the mean blood levels of phenanthrene were found to be significantly higher in cases of asthma. Studies have shown that all the PAH detected in our study are found in diesel exhaust particles (DEP), environmental tobacco smoke, and unprocessed biomass fuels. [22] According to the Agency for Toxic Substances and Disease Registry (ATSDR) 1994, [22] the most common PAH in DEP are phenanthrene, fluorenes, fluoranthene, and pyrene, including benzo (a) pyrene, with a major contribution from phenanthrene. We found only a significant association of phenanthrene alone with bronchial asthma and oxidative stress. Recent studies of PAH concentrations in ambient aerosol in Indian cities show that total PAH concentration is 10-50 times higher than that reported internationally. [3],[19] Hence, urgent steps are needed to reduce this exposure here. We have also assessed the blood levels of antioxidant enzymes CAT and SOD in cases and controls. It is quite well known that that loss of CAT activity amplifies oxidative stress and contributes to chronic inflammation. [23],[24],[25] Because we recruited cases in the initial phase of acute attack of asthma, we have not observed any difference in the level of CAT between cases and controls. Likewise, SOD in the cytosol is crucial for protecting airways against oxidative stress. [26] SOD converts superoxide anion to hydrogen peroxide. [26] Thereafter, GSH peroxide removes hydrogen peroxide and organic hydroperoxides in a reaction that consumes tripeptide GSH, resulting in a reduction in its levels. We have observed a reduced level of GSH among cases, which can be taken as an evidence of oxidative stress. However, blood levels of SOD were similar in both the groups because during the initial phase of oxidative stress only cytosol levels of SOD are reduced [27] and, with increasing disease duration, this change may also be documented in the blood levels. This was a matched case control study where simultaneous estimation of PAH and evidence of oxidative stress was performed among cases of bronchial asthma and controls. Therefore, exposure to PAH can be associated with oxidative stress as well as with asthma. We could neither establish dose response of PAH to either the severity of bronchial asthma or oxidative stress. To retain power of 80%, we kept a case to control ratio of 2:1 as it was difficult to obtain consent for venepuncture from healthy controls. Because there are hardly any studies from northern India to show the proportion of population positive for different PAH in blood samples, we only aimed to detect those that were found in at least 50% cases of bronchial asthma and 15% of controls. Thus, our sample size was inadequate to detect an association between PAH and asthma as well as oxidative stress for those that are present in more than 15% of the controls. However, our results can be generalized to other populations. Because we have documented an elevated blood level of phenanthrene among cases of bronchial asthma along with evidence of oxidative stress, measures to reduce exposure to PAH may possibly lead to reduced incidence and severity of bronchial asthma. However, further studies are needed, with a large sample size, to confirm our findings. Acknowledgment This work was funded through the Intramural short-term research project, Research Cell, King George′s Medical University, Lucknow, India.References
Copyright 2009 - Indian Journal of Occupational and Environmental Medicine The following images related to this document are available:Photo images[oe09008t1.jpg] [oe09008t3.jpg] [oe09008t2.jpg] [oe09008t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}