 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
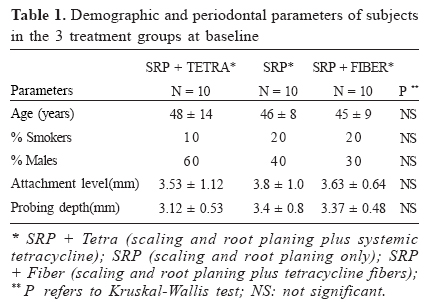
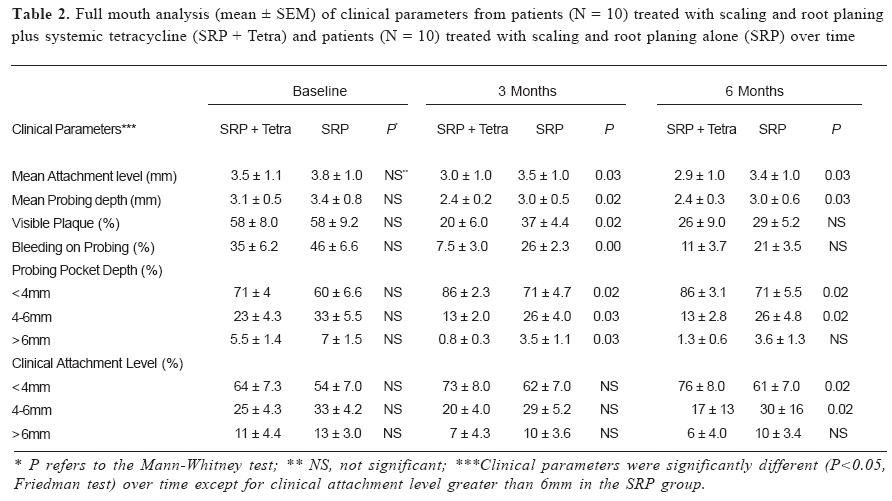
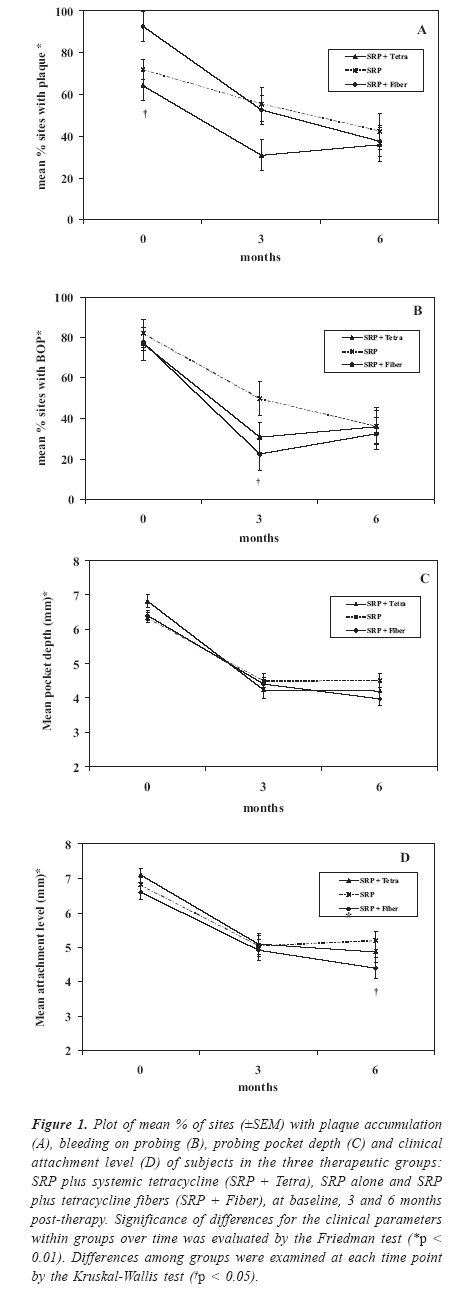
Brazilian Journal of Oral Sciences, Vol. 3, No. 8, Jan/Mar. 2004, pp. 384-389 Clinical effects of systemic and topical tetracycline therapy on chronic periodontal disease. Cristiane Gonçalves1, Rosa Maria J. Rodrigues2, Eduardo Jorge Feres-Filho3, Ana Paula Colombo4 1 MSD - Dept. of Dental Clinic - Periodontics - Gama Filho University - Rio de Janeiro -Brazil 2 MSD - Dept. of Dental Clinic - Periodontics - Federal University of Rio de Janeiro - Rio de Janeiro -Brazil 3 DSc - Dept. of Dental Clinic - Periodontics - Federal University of Rio de Janeiro - Rio de Janeiro -Brazil 4 DMSc - Dept. of Medical Microbiology Federal University of Rio de Janeiro - Rio de Janeiro -Brazil Correspondence to:Ana Paula V. Colombo Rua Gal. Dionísio, 60 apt. 804 -Humaitá CEP: 22271-050 - Rio de Janeiro, RJ, Brazil Email: apcolombo@micro.ufrj.br Received for publication: June 23, 2003 Code Number: os04001 Abstract In order to evaluate the additional effects of antimicrobials associated with conventional therapy, this study compared the clinical changes in subjects treated with scaling and root planing (SRP) alone or in combination with local or systemically administered tetracycline over time. Thirty patients with chronic periodontitis were randomly assigned to 3 groups: SRP + 500 mg of systemic tetracycline twice/day for 14 days (SRP + Tetra); SRP alone and SRP + tetracycline fibers at 4 selected sites for 10 days (SRP + Fiber). Clinical assessments were made at 6 sites/tooth at baseline, 3 and 6 months post-therapy. Two types of analyses were performed, one including all sites and other only the 4 test sites in each subject. Significant changes within and between groups were sought using Friedman, Mann-Whitney and Kruskal-Wallis tests. All therapies resulted in clinical improvement over time, which was more marked in the groups treated with tetracycline. The SRP + Tetra group had a significant lower % of sites with plaque, bleeding on probing (BOP) and deep probing pocket depth (PPD) at 3 months; higher % of sites with shallow PPD and lower % of sites with PPD = 4 - 6mm at 3 and 6 months compared to SRP alone (p < 0.05). Subjects in the SRP + Fiber group had a significant lower % of sites with BOP at 3 months and lower mean of attachment level at 6 months than the controls (p< 0.05). The adjunctive use of systemic or local tetracycline may improve the efficacy of the mechanical non-surgical therapy of chronic periodontitis. Key Words: periodontitis/ therapy; tetracycline/ therapeutic use; tetracycline/local delivery IntroductionConsiderable scientific evidence have demonstrated the importance of biofilm control and scaling and root planing for the successful treatment of periodontal diseases1,2. Nevertheless, proper and comprehensive mechanical debridement of sites with deep pockets are difficult to accomplish3. Data have demonstrated that SRP alone has limited effect on some pathogenic species, which may result in therapeutic failure4. The use of antimicrobial agents in association to conventional therapy has been proposed as a therapeutic alternative5,6. In general, success in antimicrobial therapy is dependent on the appropriate choice of the antibiotic for specific etiologic agents and the capacity of the drug to achieve an adequate level of activity at the site of infection for sufficient time7,8. Clinical trials have suggested that the adjunctive use of systemic antimicrobial agents results in additional periodontal improvement9-13. However, the inability to achieve and maintain therapeutic concentrations of the drug in the periodontal pocket, the risk of adverse drug reactions, development of bacterial resistance and dependence on patient compliance are some of the disadvantages reported5-8,14. As an alternative to systemic administration, several local delivery methods of antimicrobial agents have been tested7,15-17. In particular, a tetracycline fiber (Actsite®) has been reported to improve clinical and microbiological parameters in chronic periodontitis18-22. Despite an extensive literature on the clinical efficacy of SRP combined with systemic or local antibiotics, differences in experimental designs, types of drugs, nature of disease and delivery devices used have led to controversial results23. Therefore, the purpose of the present investigation was to compare the clinical effects of systemic and locally delivered tetracycline therapies used as adjuncts to SRP to those of SRP alone in the treatment of chronic periodontitis. Material and Methods Subject population Thirty patients with chronic periodontitis (mean age 46 ± 11years) from the Dental School at the Federal University of Rio de Janeiro (UFRJ) were selected. All subjects had at least 20 teeth and 4 sites with probing pocket depths (PPD) > 6 mm at baseline. Exclusion criteria included pregnancy, nursing, allergy to tetracycline, systemic conditions that could affect the progression or treatment of periodontal diseases, any type of periodontal intervention and use of antibiotics 6 months prior to enrolling in the study or need for prophylactic antibiotics before clinical monitoring and treatment. In order to participate, all patients were informed about the nature of the study and signed a consent form. The study protocol was previously approved by the Review Committee for Human Subjects of the University Hospital Clementino Fraga Filho (UFRJ). Experimental designSubjects were randomly assigned to 3 groups using a table of random numbers, including 10 individuals in each one. After initial clinical assessment, group 1 received full mouth scaling and root planning (SRP) plus systemically administered tetracycline (Tetraciclina, INFABRA, Rio de Janeiro, Brasil), 500 mg twice/day for 14 days, starting on the first day of mechanical therapy (SRP + Tetra). Group 2 received full mouth SRP only and group 3 received full mouth SRP followed by placement of tetracycline fibers (Actsite®, ALZA Corporation, Palo Alto, CA) at 4 randomly selected non-adjacent deep sites (PPD > 6mm) for 10 days (SRP + Fiber). These patients were instructed to rinse with 0.12% chlorhexidine solution (Periogard®, Colgate, São Paulo, Brasil) during that period of time. The sites selected for the 3 therapeutic groups did not include any teeth with furcation or endodontic/periodontic lesions. SRP was performed under local anesthesia in 4 - 6 weekly sessions of approximately 1 hour each. All patients received maintenance therapy every month, including supragingival prophylaxis and reinforcement in home care procedures during the post-therapy period. Clinical monitoringFull mouth clinical measurements were performed at 6 sites per tooth at all teeth, excluding third molars, at baseline, 3 and 6 months post-therapy. They included PPD and clinical attachment level (CAL) measured with a conventional North Carolina periodontal probe (Hu-Friedy, Chicago, IL), as well as presence or absence of visible plaque and BOP. The clinical monitoring and treatment were performed by 2 calibrated periodontists. In short, the between-examiners average agreement (± 1mm) reached 90% and the within-examiner was 90% for one and 94% for the other periodontist. Each periodontist treated 50% of the patients in each group, i.e. 5 patients per group (total of 15 subjects). The periodontist who performed the clinical measurements in a group of 15 patients was blind to the treatment delivered for this group by the other professional. Statistical analysisThe statistical program SPSS® (Statistical Package for the Social Sciences, version 8.0, Chicago, Il) was used for all the analyses. Statistical testing was performed on a "subject-based"assessment. Clinical measurements were averaged for all sites in each subject and then across subjects within each group. Two types of clinical analyses were performed: one including all sites (maximum of 168 sites) measured in each patient aimed to compare the SRP plus systemic tetracycline group to the SRP alone group. A second analysis, including only 4 randomly selected non-adjacent deep sites ( PPD > 6mm) in each subject was made in order to compare the efficacy of the local tetracycline to the other therapeutic modalities. Significance of differences in clinical parameters between two groups were sought using the Mann-Whitney test and among all groups with the Kruskal-Wallis test. In order to compare the efficacy of the three therapeutic modalities overtime, the Friedman test was employed. In all cases, statistical significance was reached at a 5% level. ResultsThe baseline clinical features of the 3 therapeutic groups are shown in Table 1. No significant differences among the 3 groups for any of the clinical parameters evaluated were observed, suggesting that the groups were homogenous. The long-term clinical changes in the SRP + Tetra and SRP groups using the full mouth measurements in the analysis are depicted in Table 2. No significant differences between groups were observed at baseline (Mann-Whitney test). In general, both therapies resulted in clinical improvement over time. A significant decrease in the percent of sites with plaque, BOP, moderate and deep PPD, as well as an increase in the prevalence of shallow sites were observed in both groups after 6 months of therapy (p < 0.01, Friedman test). Likewise, both groups showed a significant increase in % of sites with CAL < 4mm. A decrease in the prevalence of sites with high CAL (4 - 6 and > 6mm) was also detected in all subjects, although this change was not significant for CAL > 6mm in the SRP group (Friedman test). Although differences between groups over time were not significant, the SRP + Tetra group showed a more marked clinical improvement than the control group. The tetracycline group presented a significantly lower mean PPD and CAL than the SRP group at 3 and 6 months post-therapy. Comparisons between groups at 3 months demonstrated that the SRP + Tetra had a significantly lower % of sites with plaque, BOP and deep PPD than the SRP group (p < 0.05, Mann-Whitney test). However, these differences were not significant at 6 months. Conversely, a significantly higher percentage of sites with shallow PPD and lower % of sites with PPD of 4-6 mm was found at 3 and 6 months in the SRP + Tetra group compared to the SRP group (p < 0.05, Mann-Whitney test). No significant differences regarding sites with CAL > 6mm were noted between groups in each time point. A second clinical analysis included the periodontal parameters evaluated in the 4 previously selected sites in each subject of the 3 therapeutic groups at different time points (Figures 1 A-D). Similarly to the full mouth analysis, a significant improvement in all clinical parameters could be observed in the 3 groups over time (p< 0.01, Friedman test), being more marked from baseline to 3 months post-therapy. Comparisons among groups for the 4 selected sites showed that both local and systemic tetracycline groups presented a greater reduction, although not significant, in mean PPD and CAL than the SRP group. The fiber group presented a significant greater mean % of sites with plaque accumulation at baseline (p < 0.05, Kruskal- Wallis test). However, a similar reduction in this parameter was observed in the 3 groups after therapy (Fig. 1A). Pairwise comparisons showed that subjects in the fiber group had significantly lower % of sites with BOP at 3 months (Fig. 1B), as well as lower mean CAL at 6 months post-therapy than the SRP group (Fig. 1D; p < 0,05, Mann-Whitney test). DiscussionIt has been recognized that the adjunctive use of antibiotics may aid in the suppression of subgingival pathogens by mechanical periodontal therapy5-6,8-16. The clinical response to this combined approach is reflected upon enhanced gain in attachment level and reduction in probing depths initially greater than 5mm10,12. The present study compared the clinical effects of systemic or topical tetracycline administration in association with SRP to the effects of SRP alone. Due to the study design, two different analyses were required. A full mouth analysis was performed in order to evaluate the clinical responses to the systemic tetracycline. The other, aimed at 4 selected sites in each patient, allowed for a direct comparison of the locally applied to the systemic tetracycline and the SRP groups. The full mouth analysis demonstrated that both SRP plus systemic tetracycline and SRP alone led to a significant periodontal improvement. As expected, the greatest clinical changes were observed from baseline to 3 months months post-therapy, followed by a relatively stable outcome over the 6 month study period. These beneficial effects were similar to those reported in previous investigations, which demonstrated greater short-term clinical improvements following mechanical therapy in association with systemic or local tetracycline administration11,13,17,21. Subjects who received systemic antibiotic showed an overall greater improvement in most clinical parameters than those in the SRP alone group over time. These results were more apparent in relation to sites with probing depths in the range of 4-6mm from baseline to 6 months post-therapy. Similar results were observed for clinical attachment levels. Conceivably, sites with deep probing depths are not reached by conventional instrumentation3. On the other hand, the additional effect of the systemic tetracycline could be related to its capacity to reach deep periodontal pockets and other oral sites which may harbor periodontal pathogenic microorganisms, diminishing the risk of re-infection5. Furthermore, the antiinflammatory properties of tetracycline, specially its anti-matrix metalloproteinase activity, could be accounted for a more pronounced decrease in sites with BOP in patients receiving the drug24. The analysis involving the 4 selected sites in each individual demonstrated also a significant clinical improvement in all groups over time. In particular, both tetracycline groups showed a trend to result in a greater decrease in mean pocket depth and clinical attachment level when compared to the control, even though differences in clinical changes among groups were not markedly significant for most of the parameters evaluated. These findings could result from the fact that the selected test sites presented deep pockets (PPD > 6 mm), which are not efficiently treated by mechanical therapy only, but can be reached by antimicrobial drugs. Actually, microbiological analysis of those sites presented in previous report have shown that the microbial "red complex"is suppressed and kept at low levels and frequency in the groups treated with tetracycline even up to six months after therapy (data not shown)26. These data agree with other clinical trials that showed additional effects of the combined locally-derived tetracycline therapy over SRP alone17-21. In fact, some authors have demonstrated great benefits of this therapy in the treatment of patients with refractory periodontitis21. Moreover, the fiber group showed a greater reduction in percent of sites with plaque from baseline to 6 months after treatment than the other two groups. Significant differences among therapies were found only for BOP at the 3 month and for CAL at 6 month post-therapy evaluation. Both parameters were significantly more reduced in the SRP plus tetracycline fiber group compared to the SRP alone group. In this regard, one should acknowledge the fact that patients in the tetracycline fiber group were requested to use chlorhexidine mouth rinses for the entire period of time fibers were kept in place. That could have contributed to lower the plaque accumulation and marginal inflammation, reducing the prevalence of sites that bled upon probing. On the other hand, studies have reported that chlorhexidine does not seem to be effective against subgingival plaque and established periodontitis, and its short period usage would possibly have a limited impact, if any, on the clinical parameters evaluated at 3 and 6 months after therapy27. Despite the difference in CAL at 6 months between the SRP and fiber groups was statistically significant, this difference seems to be very modest clinically (SRP - 5.2 to SRP+ fiber - 4.4= 0.8 mm), particularly when considering the errors of probing measurements. Nevertheless, one should notice that this difference (0.8 mm) is an average of 40 sites within each group. In addition, the intra and inter-examiner levels of agreement in the clinical exams were quite satisfactory. Although both tetracycline groups in the present study demonstrated a better clinical response than the subjects who were treated with SRP alone, the lack of significance among therapies was most likely due to the insufficient power of the study, given the limited number of subjects examined in each group. Another aspect to be acknowledge is the high clinical efficacy of scaling and root planing per se in the treatment of chronic periodontitis. Ultimately, the selection of a higher number of subjects and particularly with agressive or refractory forms of disease could provide a better clinical and statistically meaningful response in the groups receiving antimicrobials. In conclusion, we were able to demonstrate some additional clinical effects of local or systemic tetracycline used in association with SRP over SRP alone for the treatment of chronic periodontitis over a 6 month-period. AcknowledgmentsThe authors would like to thank Dr. Goodson for assistance with the experimental study design. This work was supported in part by PRONEX, CNPq, FAPERJ and CAPES, Brazil. References
Copyright 2004 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}