 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
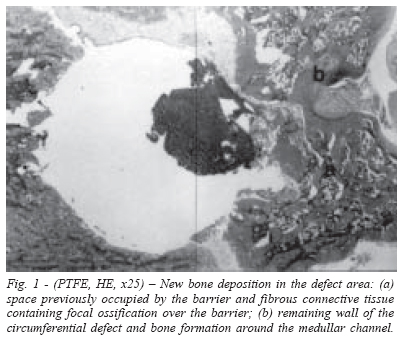
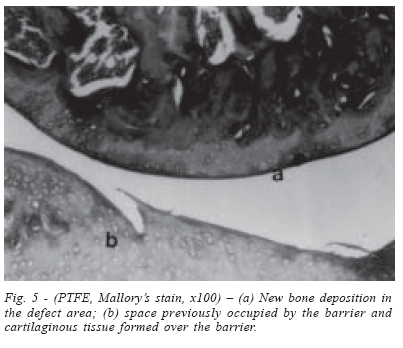
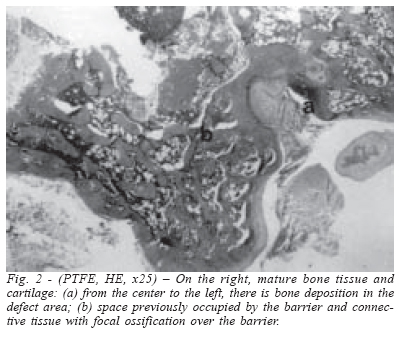
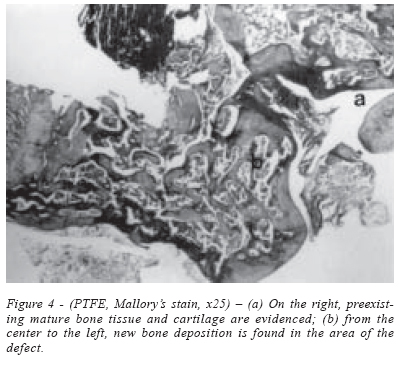
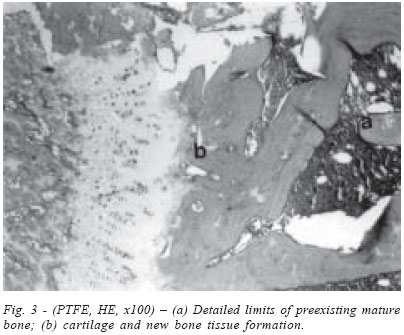
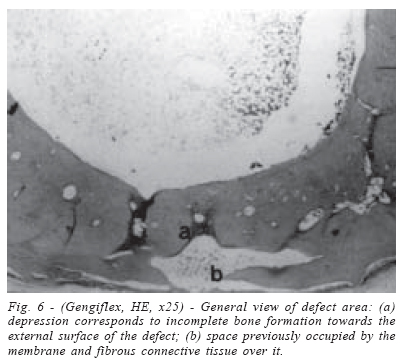
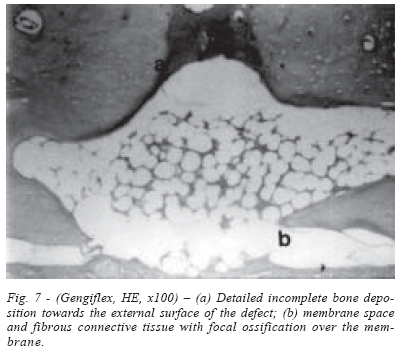
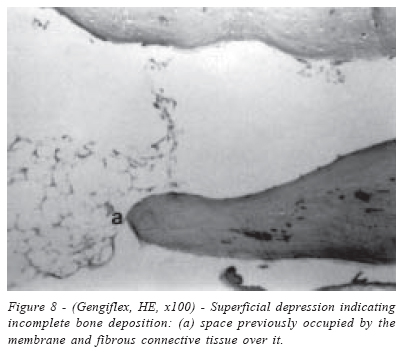
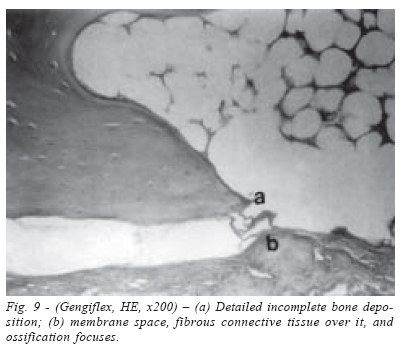
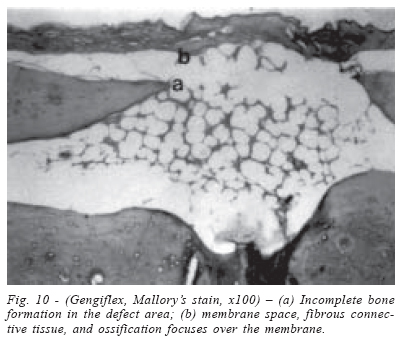
Brazilian Journal of Oral Sciences, Vol. 3, No. 8, Jan/Mar. 2004, pp. 395-400 Evaluation of two membranes in guided bone tissue regeneration: histological study in rabbits Nelson Luiz de Macedo 1a Fábio da Silva Matuda 2a Luís Guilherme Scavone de Macedo1a Adriana Socorro Ferreira Monteiro3a Marcia Carneiro Valera2a Yasmin Rodarte Carvalho3a 1 Department of Surgery, Periodontics and Radiology 2 Department of Restorative Dentistry 3 Department of Biosciences and Oral Diagnostic a São José dos Campos School of Dentistry– UNESP – São Paulo - Brazil Correspondence to:Fábio da Silva Matuda- Postgraduate student of Restorative Dentistry Av. Paul Harris, 381- Jardim das Colinas São José dos Campos- São Paulo- Brazil ZIP: 12.242-170 Phone: + 55 12 39479047 E-mail: fabiomatuda@terra.com.br Received for publication: July 28, 2003 Code Number: os04003 Abstract The purpose of this study was to evaluate bone regeneration in rabbits, comparing two types of physical barriers used to treat bone defects in guided tissue regeneration (GTR). Two osseous defects (8 mm in diameter) were performed in each hind-foot of four adult rabbits, using surgical burs with constant sterile saline solution irrigation. Defects obtained on the right hind-foots were protected with polytetrafluoroethylene (PTFE) barriers while Gengiflex membranes were used over wounds created in the left hind-foots. Rabbits were sacrificed after three months for histological evaluation of treatments performed. Defects covered with PTFE barriers were completely repaired with bone tissue. Incomplete lamellar bone formation was detected in defects treated with Gengiflex membrane, resulting in voids and lack of continuity of bone deposition. Results withdrawn from this study demonstrated that the non-porous PTFE barrier fulfilled all requirements to induce natural bone tissue regeneration, thus becoming a more effective alternative to treat osseous defects than Gengiflex membrane. Key Words: Guided bone regeneration, membranes, polytetrafluoroethylene, cellulose Introduction Experimental studies on the behavior of different cell types during tissue regeneration of surgical wounds have given support to the development of the biological principles for guided tissue regeneration (GTR). This technique aims mostly to optimize the reconstruction of periodontal tissues lost during periodontal inflammatory process1-3. Selective repopulation of the root surface by cells originated from the periodontal ligament and alveolar bone allows the organization of new attachment areas4-5. Such phenomenon becomes a viable procedure when a physical barrier is inserted between the mucoperiosteal flap and the root surface, thus excluding undesired cells from the repair process. Bone regeneration can be inhibited by fast fibroblast proliferation inside the defects. Connective tissue penetrates intra-osseous lesions and prevents natural formation of bone tissue in such defects. Limited osteogenesis occurs since the installation of fibroblasts prevents the colonization of surgical wounds by osteoblasts6-7. Therefore, physical barriers are important to avoid fibroblasts invasion in bony defects and to create adequate space so osseous cells can participate in the natural process of bone regeneration. Experimental studies, clinical trials, and case reports have encouraged GTR procedures for diverse periodontal situations8-9. Establishment of the biological principles for GTR has oriented the research of several materials for the build up of physical barriers that will induce the formation of the tissues desired. Acetate-cellulose, polytetrafluoroethylene, polylatic acid, polygalactin 910, certain types of collagen or rubber-based materials have been tested for GTR purposes. The most technologically sophisticated membranes used for GTR are constituted of polytetrafluoroethylene (Gore-Tex) or polylatic acid (Guidor and Resolut). Since polylatic acid barriers were recently developed, further studies are required to confirm its clinical effectiveness3,10-11. Non-porous PTFE barriers are biocompatible materials that have been tested for. Macedo9 (1992) first reported the application of PTFE membranes in Dentistry to repair second-degree bone lesions, demonstrating excellent results in clinical trial. Introduction of Gengiflex membrane has motivated investigations on the behavior of a cellulose-based barrier for GTR9,12-13 . Gengiflex membrane has derived from a product used as artificial skin in burns or skin tissue loss. Its inner layer is composed of a net of crystalline cellulose microfibers produced by bacteria, which offers rigidity to the membrane. The outer alkali-cellulose layer is chemically modified. According to Novaes Jr et al.14 (1992), Gengiflex is biocompatible, inert, and hypoallergenic. Its adequate structure, thickness, and resistance, additional to appropriate shapes, make this material suitable for GTR procedures. Therefore, the purpose of this study was to evaluate bone regeneration comparing two types of physical barriers, polytetrafluoroethylene or cellulose membranes, in guided bone regeneration of osseous defects induced in rabbit tibias. Material and Methods The Committee of Ethics in Research of São José School of Denstritry - UNESP, in accordance with the criteria of the animal protocol, approved this investigation. Four adult rabbits, weighing approximately 4 kg, were selected for this study. Two bone defects were created in each hind-foot of the rabbits, so different membranes were tested in the same animal. Two experimental groups were determined to investigate bone repair testing two types of physical barriers: Gengiflex membrane (Biofill, Produtos Biotecnológicos, Curitiba, PR, Brazil) or polytetrafluoroethylene PTFE barrier (Tecnoflon, Ind. & Com. Plásticos, São Paulo, SP, Brazil). Surgical proceduresRabbits were anesthetized with intramuscularly application of 0.3ml/kg of body weight of Zoletil 50 (Virbac of Brasil Ind. and Com. Ltda., São Paulo, SP, Brazil). Local complementary infiltration with 1 ml of 3% Scandicaine (Septodont, France) was performed at the surgical sites. Hind-foots were scraped and washed with 0.5% chlorhexidine gluconate solution. Medial surfaces of both tibias (left and right) were exposed after skin incision and subperiosteal dissection. Unicortical circular defects of 8 mm in diameter were performed in both hind-foots using surgical drills and abundant sterile saline solution irrigation. PTFE barriers were placed covering defects created in the right tibia while Gengiflex membranes were inserted over wounds in the left tibia. Periosteum and deep soft tissue were sutured with 4-0 absorbable vicryl (Ethicon, Johnson & Johnson) and skin was sutured with 4-0 silk thread (Ethicon - Johnson & Johnson) to induce first intention repair. Animals were fed with commercially available solid diet and water ad libitum. Visual inspectionVisual inspection of surgical sites were performed also to evaluate the position of the physical barriers and to observe whether repair followed normality patterns. Histological evaluationAnimals were sacrificed, with an overdose of anesthetic, three months after the surgical procedures were performed. Their tibias were dissected and bone fragments were immersed in 10% formalin solution for tissue fixation. Next, bone was decalcified using 20% formic acid and specimens were prepared for histological evaluation. Transverse sections were performed along the bone diaphysis in order to observe the whole circumference of the bone, including the surgical site. Tissue was stained with hematoxylin-eosin or Mallory's stain (thrichrome stain) for the descriptive histological analysis. ResultsVisual inspection results Clinical repair of the surgical wounds occurred within normality patterns. All physical barriers remained unexposed on the operated sites and did not cause clinical signs of inflammation. Bone defects covered with PTFE barriers demonstrated slight elevation of their profile, evidencing tissue regeneration. Bone profile remained unaltered in sites protected with Gengiflex cellulose membrane. Histological evaluation results Microscopic analysis of bone defects covered with the PTFE barrier demonstrated complete bone repair. External contour of the traverse sections was altered, evidencing the formation of bone callus. Exuberant neoformation of bone and cartilaginous tissues could be observed in wide superficial projections. Since the barrier was removed prior to the inclusion of the bone fragments in paraffin, a space correspondent to the barrier could be noticed on the surface of the bone callus (Figure 1). Woven fibers and cartilage formation could also be detected in the most external surface. Narrow external cortical of compact bone tissue was observed in the defect area (Figure 5). Underneath, spongy bone tissue constituted of lamellar bone trabeculae. These trabeculae were fused to each other and with the external cortical, determining wide spaces. Such spaces were filled with woven medullar hematopoietic containing several adipocytes (Figures 1, 2, and 4). Hyaline cartilage was present in some areas, especially within the boundaries of preexisting and the repaired bone tissue. Hyaline cartilage was also found along the external surface of the cortical bone formed over the defect (Figures 1, 2, 3 and 5). The cartilaginous tissue fused with the adjacent bone tissue. Sometimes bone trabeculae were visualized within the thin cartilaginous septum located among hypertrophic chondrocytes (Figure 3). Intense bone regeneration was observed also throughout the contours of the medullar channels, in the endosteal area (Figure 1). PTFE allowed complete bone repair of the defects. New bone formation was distinct from mature cortical bone, presenting countless bone trabeculae and wide medullar spaces. Cartilage areas evidenced endochondral ossification and bone deposition was thicker in sites covered by the barrier. Group protected with Gengiflex membraneTissue repair occurred with lamellar bone deposition. However, the defect was not entirely filled. In small areas the lack of bone formation was evident (Figure 6), sometimes reaching the external surface of the bone. Near that area, a bone callus was noticed altering the external contour. Compact bone tissue was deposited in the defect area. However, wide medullar spaces filled with fatty bone marrow were observed in the center, similarly to what could be seen in the medullar channels (Figures 7, 8, 9, and 10). Space previously occupied by the membrane could also be detected on the surface of the repairing bone. Externally to the blank area, fibrous connective tissue was detected, containing focal spots of bone deposition and cartilaginous tissue (Figure 9). Defects protected with Gengiflex membrane were partially repaired with bone. Although the space created by this membrane was smaller, incomplete bone regeneration was detected. A small depression and lack of continuity of bone margins were evidence of this phenomenon (Figures 6, 7, and 10). Discussion In this study, a descriptive evaluation of bone repair was carried out in rabbits to compare two physical barriers for GTR: non-porous PTFE film and cellulose-based Gengiflex membrane. The absence of connective tissue underneath the physical barriers indicated that the membranes remained stable and did not interfere with the results. Repair of soft tissues located above the physical barriers was normal, protecting membranes throughout the postoperative period. Exposure of membranes has always been associated to little or no bone formation due to bacterial contamination and subsequent inflammation of adjacent soft tissues15. Low resistance to the pressure offered by soft tissues, small ability to create appropriate space for tissue growth, and potential to induce an inflammatory reaction might have been the main factors that influenced bone regeneration in sites protected with Gengiflex barrier. Boyne16 (1964) stated that membrane porosity is important to allow the flow of fluids and nutritive substances, thus creating an optimal environment for osteogenesis. However, the results obtained from this study, in agreement with Schmid et al.17 (1994) and Lundgren et al.18 (1998), demonstrated that membrane permeability is not a requirement for GTR. PTFE-e domes (expanded polytetrafluoroethylene) placed in mice calvariae could not induce bone regeneration when the periosteum was not recovering the sites 19. The periosteum is an important structure since it offers appropriate nutrition and supplies essential growth factors during the beginning and throughout the progression of osteogenesis. Opposing to that idea, Schmid et al.17(1994) demonstrated that new bone formation does not depend on the periosteum. Likewise conducted in this study, Schmid et al.17 (1994) sutured the periosteum in the physical barrier, thus avoiding direct contact of the periosteum with the bone defect. Therefore, the results obtained from this study are in agreement with those reported by Schmid et al.17 (1994), since the periosteum was not essential for new bone formation in the situation studied. Previous studies have reported regeneration of bone and periodontal tissues in GTR techniques performing total flaps and suture of periosteum in the physical barrier6-7. Besides its biocompatibility13, the application of PTFE as physical barriers is supported due to the maintenance of adequate space for the blood clot. PTFE membranes resist tissue pressure, which can be an important requirement for bone regeneration in surgical wounds. In this study, PTFE non-porous barrier was more effective than the Gengiflex cellulose membrane. More intense bone deposition and less inflammation were observed in sites protected with PTFE barriers, in accordance to data reported in previous studies6,9,13. Unpublished data of a clinical trial using nonporous PTFE barriers to treat several types of bone defects has demonstrated that this material induced bone regeneration, even in situations of membrane exposure to the oral environment. Results withdrawn from this study demonstrated that PTFE non-porous barrier has fulfilled all requirements to induce natural bone regeneration in GTR. Although PTFE film was not porous, it was more effective in repairing osseous defects than Gengiflex cellulose membrane. AcknowledgementsSpecial acknowledgements to the staff members from the Research Support Laboratory at São José dos Campos School of Dentistry - UNESP, Mônica and Salete, for all the help and assistance they offered during the development of this research. References
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}