 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 3, No. 8, Jan/Mar. 2004, pp. 420-424 Determination of root dentin and cementum micro hardness Fabiano Ribeiro Cirano 1 Giuseppe Alexandre Romito 2 José Hildebrando Todescan 3 1 PhD Student in Periodontics, Department of Stomatology, Periodontics division University of São Paulo - Brazil 2 Professor, Department of Stomatology, Periodontics division University of São Paulo Brazil 3 Ex-Chairman, Department of Stomatology, Periodontics division University of São Paulo Brazil Correspondence to: Giuseppe Alexandre Romito Faculdade de Odontologia - Universidade de São Paulo. Disciplina de Periodontia Av. Lineu Prestes, 2227 Cidade Universitária São Paulo S.P. Brazil CEP 05508-900 Telefone: 55 (11) 5084-9949 ou 55 (11) 8174-3639 e-mail: garomito@usp.br Received for publication: January 12,2004 Code Number: os04008 Abstract Vickers micro hardness was assessed on root dentin and cementum in 30 canines obtained from the Periodontics Discipline tooth bank. Crown and cervical portion of the root were discarded by a transverse section situated 3mm, apically, from the cemento-enamel junction on the buccal surface, thus obtaining the root specimen. On root dentin, mean micro hardness values were obtained for 3 regions: (DR1) from 0.05 to 0.1 mm of the cemento dentin junction – 30.64 VHN; (DR2) from 0.3 to 0.5 mm of the cemento dentin junction – 56.92 VHN and (DR3) from 0.8 to 1.0 mm of the cemento dentin junction – 32.70 VHN. After statistical analysis (Variance Analysis test, p < 0,05), we conclude that micro hardness at the DR2 region was statistically greater than that at the DR3 region which was, in turn, greater than that at the DR1 region. The mean micro hardness of cementum was 19.70 VHN. Key Words: micro hardness, root dentin, cementum Introduction The need for mechanical intervention on dental surfaces during periodontal treatment as well as in health maintenance is commonplace1. The amount of tissue loss depends on various factors or parameters, one of these, are possibly the micro hardness of the tissue being manipulated. Root dentin micro hardness was studied by Craig et al.2, Rautiola and Craig3 and Saleh and Ettman4, who found that the central portion of this tissue presented a greater mean micro hardness when compared to the regions close to the pulp and to the cementum. Riffle5,6 showed that root dentin micro hardness figures presented an inversely proportional variation according to the patient's age. However, Dalitz7 found no relationship between age and rood dentin micro hardness. Riffle5,6 showed that root dentin micro hardness presented smaller values in patients suffering from periodontal disease or with cementum exposure. These values were inversely proportional to the depth of the periodontal pockets. Emslie and Stack8 also showed that the cervical root dentin presented a lower micro hardness value in teeth with periodontal pockets, this reduction being greater in the internal dentin than in the superficial dentin. However, Rautiola and Craig3 showed there was no difference in root dentin micro hardness in regions exposed to periodontal disease. Few studies on cementum have been carried out due to the technical difficulties involved9. Rautiola and Craig3 found no differences in cementum micro hardness in different locations. Riffle5,6 showed that cementum micro hardness is inversely proportional to the patient's age. On the other hand, Stepnick and Gettleman9 found no significant differences related to age, however they showed that cementum presents considerably smaller micro hardness values than dentin. Riffle5,6 also noted that cementum micro hardness values presented an inversely proportional variation to the depth of the periodontal pouch. Rautiola and Craig3 and Warren et al.10 verified that there were no significant differences between cementum exposed and non-exposed to periodontal disease. Thus, due to the great diversion reported in literature and the lack of uniformity presented by the authors as to a micro hardness standard in dental tissues, it has seemed to us that these physical properties need further studying in the search for answers that may establish directives for dental micro hardness. Moreover, this property may be directly related to the amount of tissue removed during the different kinds of procedure carried out on dental surfaces, during periodontal treatment and supportive periodontal treatment. The aim of this study was to analyze Vickers micro hardness values on different regions of root dentin and cementum. Material and MethodsThirty healthy canines were used, with the approval of the Dental College of University of São Paulo-Brazil Ethics Committee. The method utilized to get the specimens as done according Cirano et al.11, which we resumed describe as follows: With the use of a cutter (Labcut 1010 - Extec), mounted with a diamond disc (XL 12205 - Extec) a transversal section was made on each tooth. The apical portion of its root, held each tooth by the instrument's fixation device, for the execution of the section. The section was cut 3 mm apical from the cemento enamel junction on the buccal surface; the most incisal portion of the tooth was discarded. For the evaluation of micro hardness, each specimen was positioned in an adjustable universal clamp (Shimadzu). The clamp was locked into a position so that the exposed surface stayed parallel to the horizontal plane, immobilizing the specimen completely during the measurement. The ensemble was later taken to a micro durometer (HMV 2000 - Shimadzu), where Vickers micro hardness measurements were taken, at room temperature. Twelve penetrations were carried out, three of them on each of the four surfaces (buccal, lingual and two proximal) on the following regions: Root Dentin:
Cementum:
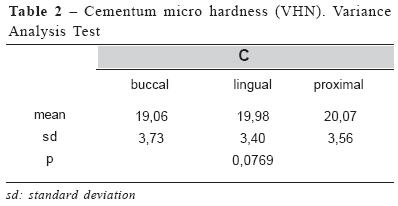
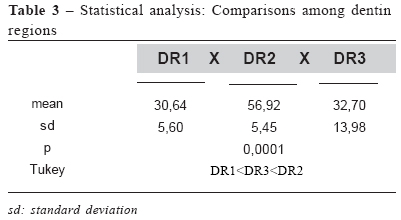
Using a light microscope coupled to the micro durometer, each of the markings made with the spherical drill was located. Next, maintaining the alignment with these markings, penetrations on each of the surfaces were carried out with the Vickers instrument. The penetrations were carried out at a minimal distance of 100mm apart. This care was taken in order to avoid the possible interference of one penetration being too close to the other. The penetration diagonals were measured with the aid of bars located on the instrument's viewfinder and through these values, the micro hardness of that spot was calculated. For this experiment, the micro durometer was calibrated at 50 grams applied for 45 seconds, a time considered as being enough for the plastic deformation of the structures evaluated. After all values having been obtained, the results were grouped and submitted to statistical analysis. ResultsInitially, it was analyzed whether there was a statistical differences between micro hardness values assessed on the buccal, lingual, and proximal surfaces in each of the regions evaluated, on root dentin and on cementum. According to tables 1 and 2, we noticed that none of the regions of the root dentin and of the cementum presented a statistically significant difference between the surfaces. Micro hardness of different regions of the root dentin was later compared. The micro hardness of the DR2 region was statistically greater than that of the DR3 region, which in turn, was greater than that of the DR1 region (Table 3). Because the cementum was not subdivided into regions due to its diminished thickness, we adopted the mean micro hardness value of 19.70 VHN. Discussion The main objective of periodontal treatment is achieving healthy periodontal tissues12. The removal of the plaque-calculus association, as being a local etiologic agent, should make up part of every therapeutic strategy against periodontal disease. Plaque-calculus removal and accumulation control techniques are, mostly, mechanical and relate with procedures denominated scaling and root planning. Clinical procedures are often carried out without adequate evaluation of its interferences or consequences. Likewise, one should take into account procedures relating to periodical control and maintenance, as well as the mechanical mechanisms of domestic oral hygiene. All of these procedures carried out on dental surfaces could lead to their wear and thus, more information on tooth structures should be obtained. In this way, we consider the study of tooth surface micro hardness of importance, for this property may present some relation to the wear suffered by teeth, during therapeutic and maintenance procedures, which are part of periodontal therapy. This study was aimed at assessing the occurrence of variation according to location of the region analyzed, as to distance in relation to the external surface and as to position on different surfaces. Furthermore, we compared our results to that of other authors who worked with Vickers or Knoop micro hardness. This was achieved based on the study by Ryge et al.13, who demonstrated that when using charges of between 50 and 100g, Knoop and Vickers micro hardness are equivalent. All regions of root dentin did not present a statistically significant difference on the different surfaces studied, displaying uniformity in micro hardness in each of the bands studied. Mjör14 demonstrated that human dentin presents a relatively uniform pattern of calcification, in layers. The highest micro hardness value of root dentin was that of the DR2 region (56.92 VHN), an intermediate micro hardness value was found on the DR3 region (32.70 VHN), and the smallest value was found on the DR1 region, next to the dentin-cementum junction (30.64 VHN). Our results suggest a pattern similar to that found by Craig et al.2; Rautiola and Craig3 and Saleh and Ettman4 where micro hardness of root dentin at the DR2 region was greater than that of regions DR1 and DR3. Fairbanks et al.15 was the only one that did not follow the aforementioned standard, and presented micro hardness values of 43.96 VHN for the root dentin close to the cemento dentin junction, and of 43.51 VHN for dentin close to the pulp, both of these figures being higher than the 41.6 VHN micro hardness value found for root dentin located in an intermediate position between these two structures. Our study presented a disparity as to micro hardness of different regions in relation to other studies. Even so, we obtained some results that corroborated those found in other studies. A value of 30.64 VHN for the DR1 region was obtained, which is close to the 38 KHN value found next to the cementodentin junction found by Rautiola and Craig3. A result of 56.92 VHN for the DR2 region was obtained, which was very close to the 51.7 to 54.4 KHN for root dentin 1mm away from the pulp, described by Saleh and Ettman4. Furthermore, we obtained a micro hardness value of 32.70 VHN for the DR3 region, which is very close to the 34 KHN obtained by Craig et al.2 for dentin adjacent to the root canal. We must highlight that different units of micro hardness are being compared, however, this can be considered valid as supported by Ryge et al.13 who showed that figures obtained by the Knoop and Vickers penetrators are similar, especially with charges over 50 g. The variation obtained for each of the regions of root dentin can be justified by the anatomical and histological characteristics of these structures. Smaller micro hardness values of dentin adjacent to the cemento-dentin junction can be explained by the presence of a high concentration of interglobular dentin (with a higher organic content), by the occurrence of branching of the dental tubules and by smaller calcification, as reported by Craig et al.2 and again by Mjör14, as to the hypo mineralization. Marshall16 reported that dentin is considered being a heterogeneous material that contains tubules of micrometers in diameter, circled by highly mineralized peritubular dentin, with approximately 95% of mineral content, and intertubular dentin, contained in a collagen matrix, with approximately 30% of mineral content. Before the study by Pashley et al.17, changes in dentin micro hardness were correlated with the variation of the dental tubules and it was believed that a decrease in micro hardness observed with relation to the proximity of the pulp was due to the increase in tubule density and possible changes in mineral density. However, when studying peritubular and intertubular dentin micro hardness, Kinney et al.18 proposed that the decrease in dentin micro hardness observed with the proximity of the pulp could be attributed to changes in intertubular dentin micro hardness and not by the increase in the number of dentinary tubules as had been previously suggested by Pashley et al.17. In our study, root dentin micro hardness close to the cemento dentin junction (DR1) presented lower values probably due to the presence of a hypo mineralized zone in this region. The DR2 region presented the highest values, probably due to its proximity to the cemento dentin junction, where intertubular dentin presents higher micro hardness. The DR3 region presented perhaps lower values, maybe due to its proximity to the root canal. Cementum presented the lowest micro hardness values (19.70 VHN) in our study, a fact also observed by numerous authors, due to the mineral composition of this structure3,9,10. The mean micro hardness value of cementum obtained in our study was very similar to that observed by Warren et al.10 who obtained a value for cementum micro hardness in teeth with periodontal involvement of 17.0 KHN and for those without periodontal involvement 20.0 KHN. However, the discrepancy was great when compared to the study carried out by Rautiola and Craig3, where the mean micro hardness value for non-exposed cementum was 39.6 KHN and for exposed cementum, 39.3 KHN. Even though we were not able to determine whether or not the teeth used in this study presented periodontal involvement, this factor seems not to attribute great relevance, as reported by Rautiola and Craig3 and by Warren et al.10 who showed that there was no statistically significant difference between micro hardness of cementum in teeth with and without periodontal involvement. Recent studies19-22 showed the importance of micro hardness on the evaluation of products (bleaching agents, for instance) or procedures used on root structures. Periodontics carries out numerous procedures with the aim of treating the unhealthy root in order to re-establish periodontal health. Procedures range from prophylaxis using rubber cup and pummy stone, through sodium bicarbonate jetting, to root treatment with manual instruments and ultra-sound equipment. Each procedure will act differently on a dental surface and its choice will depend on the region being treated. Thus, when new research is carried out and micro hardness will serve for the analysis of results obtained after mechanical and/or chemical treatment on root surface, the micro hardness values found tin this study may be used as a parameter for comparing therapeutic conducts elected. ConclusionsWithin the scope of this study, we can conclude that:
Copyright 2004 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}