 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
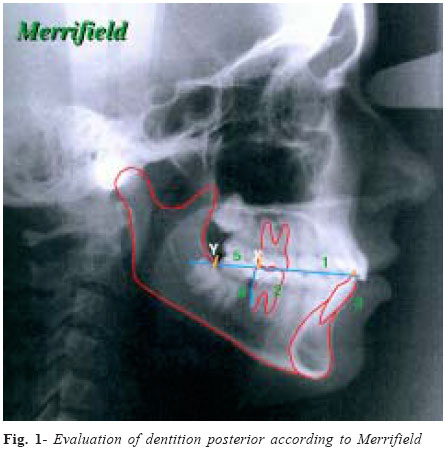
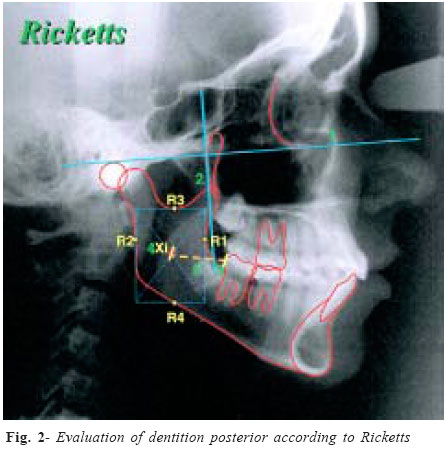
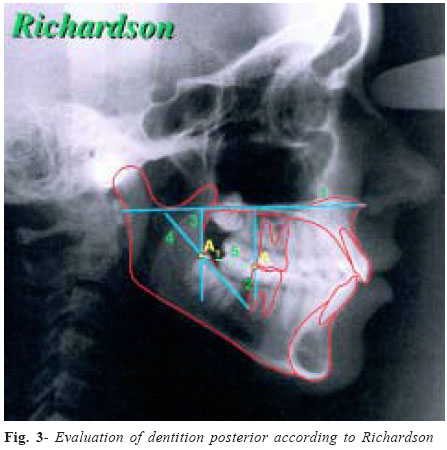
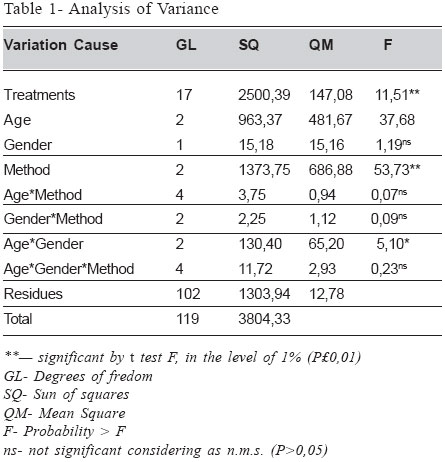
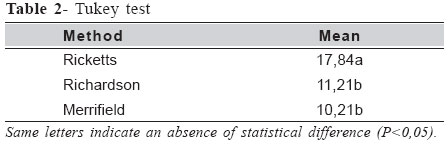
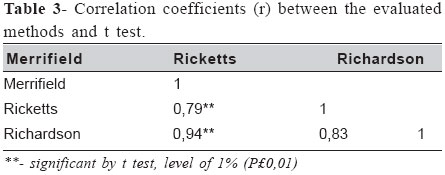
Brazilian Journal of Oral Sciences, Vol. 3, No. 9, April/June 2004, pp. 454-457 Methods of evaluation of mandible posterior segment Haroldo Amorin de Almeida1, Maria Helena Castro de Almeida1, João Sarmento Pereira-Neto1, Maria Beatriz Borges de Araújo1, Stenyo Wanderley Tavares1, Fábio Lourenço Romano1 1Department of Orthodontics, University of Campinas - Piracicaba Dental School - Brazil Correspondence to: João Sarmento Pereira Neto, Av. Limeira, 901 Caixa Postal 52, CEP: 13414-903 Piracicaba -SP e-mail: sarmento@fop.unicamp.br Received for publication: January 30, 2004 Code Number: os04014 Abstract The aim of this research was to compare three methods to evaluate the availability of existent space in the mandible posterior segment; the methods are the Merrifield’s (1986), Ricketts’ (1976) and Richardson’s (1992). Sixty 60 teleradiographs in lateral pattern, from head, belonging to 60 Brazilian leucoderm subjects were evaluated. The age range from 9 to 19 years, all having a mal-occlusion of Class II, division 1, equally separated as for the gender (being 30 of male gender and 30 of female gender). It was concluded: Evidence of growing in the mandible arch posterior segment in the age range studied, with mean values of 10,21 mm for the Merrifield, 11,21 mm for the Richardson and 17,84 mm for the Ricketts methods. We have concluded that irrespective of the evaluated method, it was verified that the female gender has a more precocious growing (12,17 mm) as compared to the male gender (8,81 mm), in the ages 9 to 12. In the correlation between the employed methods, there was no a statistical difference among themselves by the t test, in the level of 1% (p £ 0,01). Key Words: orthodontics, cephalometric, diagnostic IntroductionThe changes in feeding habits resulted in a decrease in the masticatory force, causing, among other effects, a gradual reduction in the sizes of maxilla and mandible. Despite this event to be associated to the decrease in tooth number, the lack of space is a reality that challenges the orthodontist, especially referring to the dentition posterior space1. Aware of these occurrences, some researchers have worried about the problems of development and eruption of the third molars, especially as associated to the pos-treatment recurrences. However, there is a frequent interest in relation to the necessary space to accommodate the second and third molars, frequently there is a deficiency of space in this region, being necessary, during a orthodontic intervention, the indication of exodontias2-3. The precocious extraction of the third molars has been indicated as a measure to compensate the lack of growing in the dental arch posterior segment. Nevertheless, the studies on the space availability prevision for this region can, in many situations, clearly to solve the fate of the third molars for the different types of occlusion4-5. It seems that there is not a precise age that determines the inferior arch posterior segment growth. Ledyard Jr6 (1953) has considered the limit at 14 years; Hoek7 (1964), at 15-16 years; Richardson8 (1973), at 15 years to the female gender and at 17 years to the male gender; and Merrifield9 (1986), at 14 years to the female gender and a more late growing to the male gender, verifying this way a sexual dimorphism. In this context, our intuit is to evaluate the space availability in the inferior arch posterior segment in Brazilian leucoderm subjects, in the age range from 9 to 19 years, having a malocclusion of Class II, ision 1, correlating it using the Merrifield (1986)9, Ricketts10 (1976) and Richardson11 (1992) methods, and verifying which one will be the ideal for a more reliable prevision. Material and MethodsTeleradiographs in lateral pattern, belonging to 60 Brazilian leucoderm subjects, from region of Piracicaba (SP), equally separated as for the gender, in the age range from 9 to 19, all presenting a mal-occlusion of Class II, division 1. The evaluation according to Merrifield12 (1978) needs the determination of the occlusion plane (line that passes by the medial cuspids of the first molars and, in the anterior portion, by the incisive edge of inferior's), from the X point (line perpendicular to the occlusive plane tangent to the distal face of the inferior permanent first molar) to the Y point (intersection of the occlusive plane and the anterior edge of the mandible ascending branch). The distance from X to Y was measured with a millimeter rule, corresponding to the existent space in the inferior dental arch posterior segment (Figure 1). For the evaluation of posterior dentition of according to Ricketts10 (1976), the center of the mandible branch was determined (Xi) and of the distal face of the inferior permanent second molar (DF2MI). The location of Xi point was geometrically obtained through planes perpendicular to the Frankfurt plane and to the Vertical Pterigoid Plane, tangent to the points R1 (deepest point of the anterior edge concavity of the ascending branch), R2 (point over the posterior edge of the ascending branch, projection of point R1 parallel to the Frankfurt), R3 (deepest point of the sigmoid chamfer) and R4 (point in the inferior edge of the ascending branch, projection of point R3 parallel to the VPP). The Xi point is localized exactly in the center of the rectangle formed by the above-mentioned planes, in the intersection of the diagonals. After the determination of the points, a direct read of Xi to DF2MI distance was executed using a millimeter rule, corresponding to the existent space in the inferior dental arch posterior segment (Figure 2). The evaluation of posterior dentition of according to Richardson11 (1992) requires the determination of points A (intersection of a perpendicular line to the palatine plane and tangent to the distal face contour of the inferior permanent first molar) and A1 (intersection of two lines, one tangent to the occlusive edge of the inferior permanent third molar and other tangent to the anterior edge of the mandible branch perpendicular to the palatine plane). The distance from A to A1 corresponds to the existent space in the inferior dental arch posterior segment (Figure 3). To minimize and determine an error margin associated to the used method, all the teleradiographs were retraced twice, with a minimal interval of 10 days, and always by the same operator13. Results The analysis of Variance to the variable distance is presented on Table I. There was a significant statistical differences between the methods and the age classes. The smaller means of distance had been observed using the Richardson and Merrifield methods, without a significant statistical difference. The mean distance obtained by the Ricketts method was statistically superior to the others methods (Table 2). Studying the linear correlation between the used methods in this article, it was observed by t test a significant statistical difference, and it was positive for all the methods; that is, despite of the methods proposed by Merrifield and Richardson are equal among themselves and distinct from the Ricketts', they all have varied in the same way (Table 3). Discussion The availability of existent space in the mandible posterior segment has been the object of several studies due to the high frequency of impaction of the inferior third molars10-12, 14-17. To foster the amount of posterior space, or to evaluate its evolution, it is necessary to have an appropriate radiograph. In this work, it was chosen a cephalometric radiograph in lateral pattern since it is used by the three prevision methods employed in the methodology, and it is an integrant part of the orthodontic diagnostic. In this research, were evaluated three methods of measuring space in the dentition posterior segment. It was found significant statistical differences among them. There were also differences among the age classes, which to prove that the measuring methods are independent of the age factor. The mean value for the measures of the existent space in the dentition posterior segments were 17,84 mm by the Ricketts, 11,21 mm by the Richardson and 10,21 mm by the Merrifield techniques. This values'differences were statistically significant. The mean value found in this study by the Ricketts'prevision method suggests that probably there won't be space for the eruption of third molars, for according the author are necessary 30 mm or more in the age of 8 to 9 years to it happens. The values obtained by the Richardson and Merrifield methods cannot to be analyzed within a group, but rather inidually for each patient for they depend upon the teeth size in this region. The mean distances'of each method in relation to the gender was 18,49 mm for females and 17,77 mm males by the Ricketts method; 11,90 mm for the female and 11,08 mm for the male gender by the Richardson method; and 10,62 mm for the female and 10,49 mm for the male gender by the Merrifield method. Between the Merrifield and Richardson methods, there was no significant statistical difference. The Ricketts method was statistically superior to the others, and it can be explained by the variations in the existent space measure in the posterior region. However, the methods have presented the same behavior as ordered in a straight line as proved by linear correlation and t tests, showing that all they vary in the same way. It was observed that irrespective of the method, when we consider the existent differences between age and gender, the mean distances that have been obtained from 9 to 12 years for the female and male genders were statistically different; from 13 to 15 and 16 to 19 years, significant alterations have not occurred. The smaller mean was found in the method proposed by Merrifield at an age from 9 to 12 years age, and it is explained by the growing burst that occurs on this age range, for the mandible increases under the same influences of the craniofacial growing6, 12, 15, 18, 19. The higher means were found in the range of 16 to 19 years, principally by the Ricketts method (22,04 mm), evidencing an increase of the inferior dental arch due to a higher growing answer6,12,15,18-19. Among the analyzed methods, the Merrifield's12 (1978) was those showing a easier application References
Copyright 2004 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}