 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
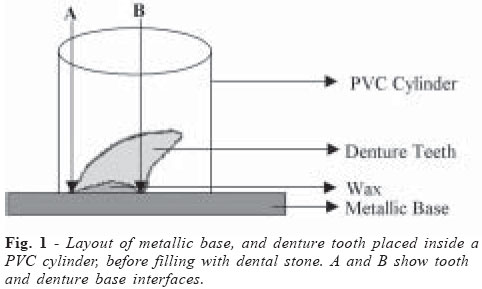
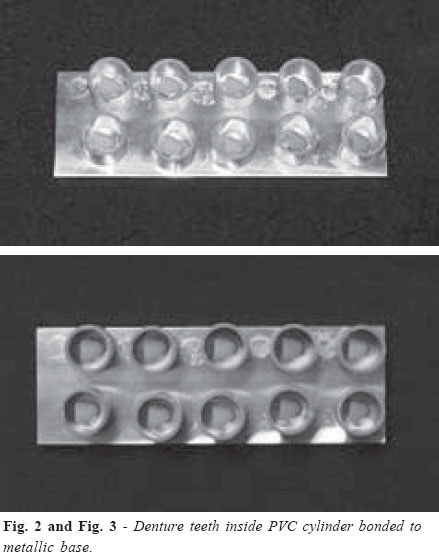
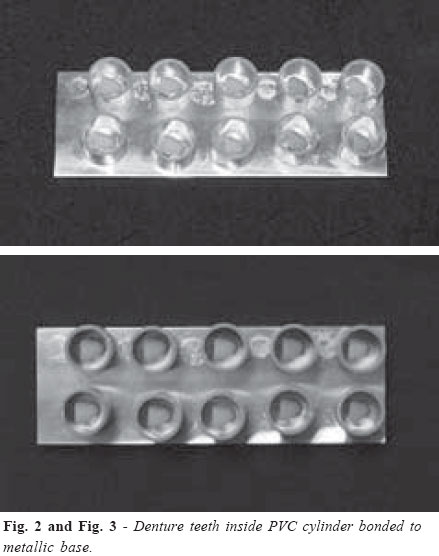
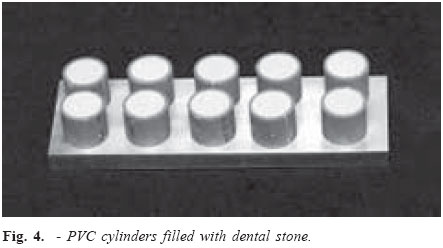
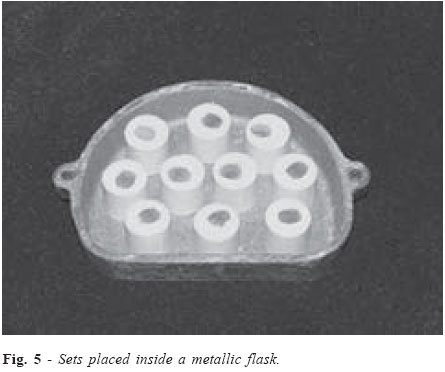
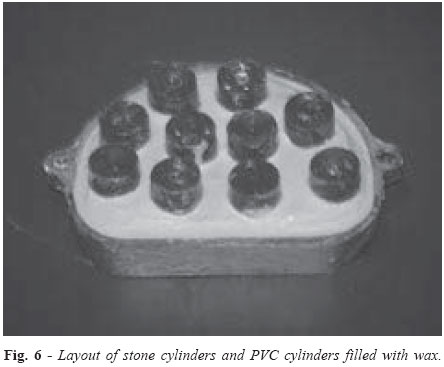
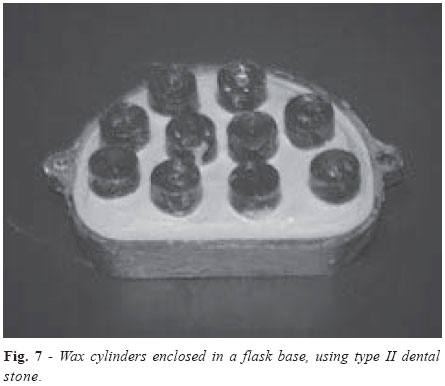
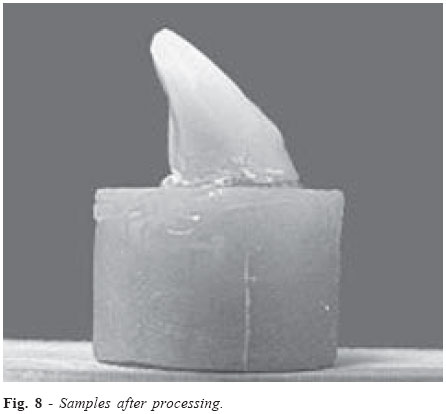
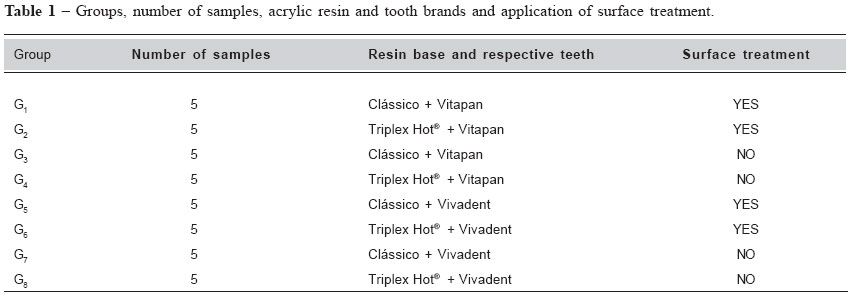
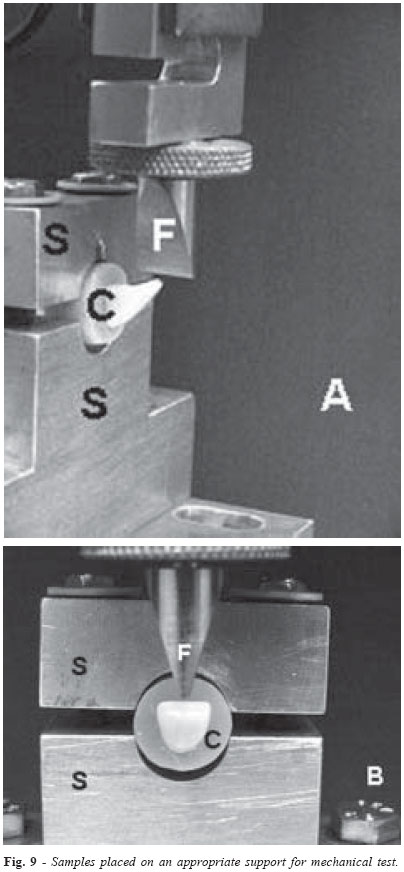
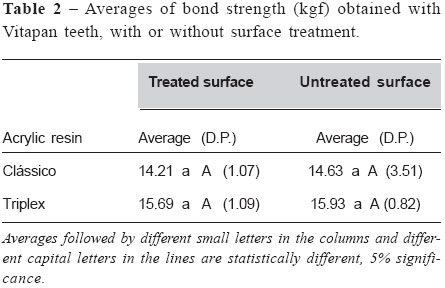
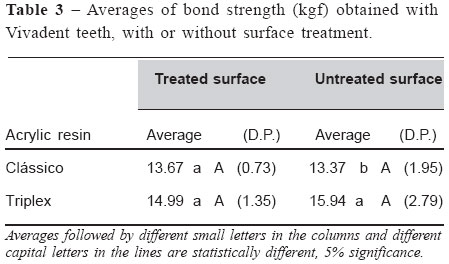
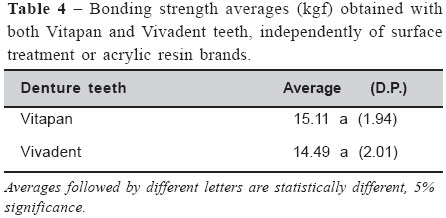
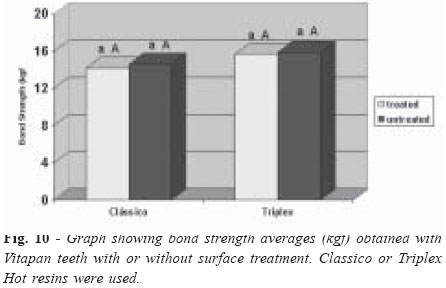
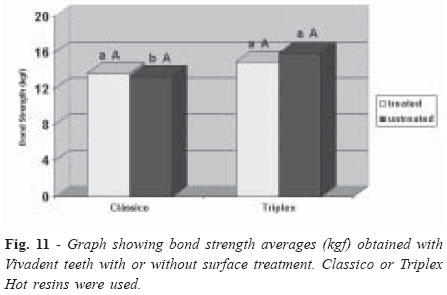
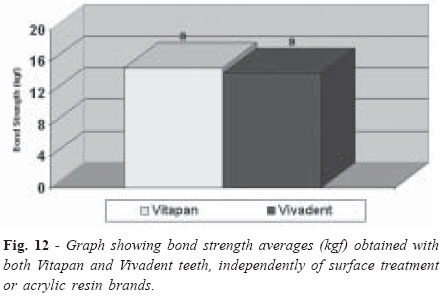
Brazilian Journal of Oral Sciences, Vol. 3, No. 9, April/June 2004, pp. 458-464 Evaluation of bond strength of denture teeth bonded to heat polymerized acrylic resin denture bases Guilherme Saavedra 1 Maximiliano Piero Neisser 2 Mário Alexandre Coelho Sinhoreti 3 Cristiane Machado 4 1 Graduate student, Paulista Dental School,Julio de Mesquita Filho State University (UNESP), São José dos Campos, São Paulo, Brazil. 2 Assistant Professor Department of Dental Materials and Prosthodontics, Paulista Dental School, Julio de Mesquita Filho State University (UNESP), São José dos Campos, São Paulo, Brazil. 3 Associated Professor, Department of Dental Materials, Piracicaba Dental School, University of Campinas (UNICAMP), Piracicaba, São Paulo, Brazil.4 Post graduated student, Department of Prosthesis and Periodontology, Piracicaba Dental School, University of Campinas (UNICAMP), Piracicaba, São Paulo, Brazil. Correspondence to: Guilherme Saavedra Julio de Mesquita Filho State University (UNESP), Paulista Dental School Av. Francisco José Longo, 777 São Jose dos Campos, SP - Brazil CEP: 12245-000 E-mail: saavedra@fosjc.unesp.br Phone: (11) 38158897 / (11)98140413 Received for publication: February 2, 2004 Code Number: os04015 Abstract The purpose of this study was to investigate bond strength between two commercially available plastic teeth, Vitapan (Vp) and Vivadent (Vv), and two commercially available denture base resins, Classico (C) and Triplex Hot (T), as affected by tooth surface treatment. Eight experimental groups, each consisting of 5 samples, were investigated according to the variables: tooth brand (Vv or Vp), resin brand (C or T) and treated or untreated tooth surface (S or N, respectively). For surface treatment, tooth surface was grooved with aluminum oxide particles (110µm). Bond strength was evaluated with a tensile force test device on an EMIC-DL-2000 machine, speed of 0.5 mm/min, until failure. Results were evaluated statistically with ANOVA and Tukey’s test (5% significance). Obtained values were (kgf): G1: Vp/C/ S=14.21 (1.07); G2: Vp/T/S=15.68 (1.09); G3: Vp/C/N=14.63 (3.51); G4: Vp/T/N=15.93 (0.82); G5: Vv/C/S=13.67 (0.73); G6: Vv/T/ S=14.99 (1.35); G7: Vv/C/N=13.37 (1.95) and G8: Vv/T/N=15.94 (2.79). Statistically significant differences were found only between groups G7 and G8 (pd”.05). The following can be concluded: (1) there were statistically significant differences among Vitapan teeth and the other groups; (2) Vivadent teeth that received surface treatment showed higher bond strength values when Triplex Hot resin was used; (3) surface treatment did not modify bond strength values. Key Words: complete denture, acrylic resin, denture teeth, bond strength, surface treatment Introduction Complete dentures should restore aesthetic, phonetics and mastication. Complete denture bases are made of some type of acrylic resin. Acrylic resins were developed in 1936, to substitute vulcanized rubber (Vulcanite) patented by Goodyear in 1851. Vulcanite had been widely used for 80 years, despite color, opacity and porosity restrictions as well as relining and burnishing difficulties. Some of acrylic resin properties are not desirable, such as low thermal conductivity, surface micro-porosity, low resistance and susceptibility to abrasion. However, there are many advantages in using acrylic resins for complete denture construction, such as chromatic compatibility with soft tissues, easy relining procedures, low specific weight, low solubility in oral fluids, low cost, and simplicity of the device used for resin processing. Water bath polymerization is the commonest and most widely used method for denture processing1. Acrylic resin teeth are more widely used than porcelain teeth in the fabrication of dentures. Regarding patients' satisfaction, Lamoureux et al.2 studied patient's satisfaction and found there was no statistically significant difference between complete dentures fabricated with porcelain teeth and acrylic resin teeth. Sellen et al.3 affirmed that acrylic resin teeth should be used for fabrication of dentures in most cases. One of the commonest causes of prosthesis failure is the alteration of adhesion between plastic tooth and acrylic resin denture base. This adhesion may be influenced by: the type of resin base material and its physical and chemical properties; contamination of the bond interfaces during laboratorial procedures and the presence of impurities on tooth surface in close contact with the denture base. Cunningham and Benington4 and Thean et al.5 affirmed that the bond failure between denture base material and resin teeth remained a significant problem for treatment success and that wax or sodium alginate-contaminated surfaces produced highly significant weaker bonds. Wax removing is an important step in obtaining a consistently high bond strength value. According to Kawara et al.6 and Darbar et al.7-8, failures are probably caused by gap and crack propagation in areas of load concentration. Many studies were carried out in order to minimize this problem. Buyukyilmaz and Ruyter9 studied the influence of the temperature reached during denture processing and concluded that the higher temperature, the better bond strength of autopolymerizing acrylic resins. Buyukyilmaz and Ruyter9 also found that bond characteristics changed from adhesive failure to cohesive failure due to temperature increasing, especially for over 50ºC temperatures. Vallittu5 related that with temperature increasing, denture base monomer spread in acrylic resin denture teeth more effectively. Vergani et al.10 recommended different kinds of tooth surface treatment before bonding teeth to denture bases. Chung et al.11 determined a protocol in order to minimize bond failures between tooth and denture base. Tooth surface treatment should be carried before bonding by grooving tooth surface (mechanical retentions) and applying liquid methyl methacrylate monomer. Vallittu5 observed that mechanical retentions on acrylic resin tooth surface promoted better adhesion. Cunningham12 described that the application of a bonding agent on teeth/ denture base interfaces significantly increased bond strength values. Thus, this author recommended the application of dichloromethane on tooth surface before denture processing. Takahashi et al.13 described that the application of dichloromethane resulted in a significant increase of bond strength values compared to the application of diatoric. Cunningham and Benington14 investigated variables that might affect the bond between plastic teeth and denture base resin such as resin stage, tooth surface treatment, processing and monomer cementing. A significantly stronger bond was obtained when the resin was packed late in the dough stage and, in all the cases, when a high-impact resin was used. Tooth surface modification by grooving showed no significant differences when compared with unmodified surfaces. Wax-contaminated surfaces produced significant weaker bonds. Time of introduction and duration of water-bath processing showed no significant effect on bond strength. Monomer cementing of tooth surface, especially with high-impact monomer significantly improved bond strength. The application of resin cements produced the most significant increase in denture tooth bond strength. The authors recommended an adequate removal of wax from tooth surface followed by the application of resin cement before denture processing. Regarding mechanical tests, most authors recommended the use of non-axial tensile force to analyze tooth/denture base bond strength. The purpose of this study was to evaluate bond strength between two commercially available plastic teeth and two commercially available denture base resins as affected by tooth surface treatment. Material and Methods Samples preparation Forty denture teeth (right maxillary central incisor) were selected (20 Vivadent (Ivoclar) and 20 Vitapan (Vita)). Each tooth was bonded to a metallic base and surrounded by an 18-mm height, 17-mm diameter polyvinyl chloride (PVC) cylinder (Figure 1). In order to keep similar angulations for all teeth, regarding PVC cylinder long axis, tooth was bonded to the metallic base with wax, and after, tooth was pressed until contacting the metallic base (middle part of tooth buccal surface and middle part of tooth palatal surface) (Figure 1, arrows A and B). PVC cylinders were bonded to the metallic base with vinyl acetate (Cascolar) (Figures 2 and 3). Type II dental stone was proportioned according to manufacturer's instructions and placed into the PVC cylinders under vibration (Figure 4). After stone setting, each PVC cylinder was separated of the metallic base and checked to verify absence of porosity and adequate removal of wax. PVC cylinders were longitudinally cut using aluminum oxide disks and removed. Mechanical retentions were made on stone cylinder lateral surface and stone cylinders were placed inside the base of a metallic flask, in order to verify available space (Figure 5). After that, liquid wax was applied into the PVC cylinders to create a virtual space that will be filled with acrylic resin, simulating a denture base (Figure 6). The base of the flask was filled with type II stone (Figure 7). After stone setting, sodium alginate (Cel-Lac) was applied on stone surface. The superior part of the flask was placed and filled with type II stone. The flask was closed and put under pressure (1250 kgf) for 45 minutes. After stone setting, the flask was immersed in boiling water for 10 minutes, removed and opened. Wax was removed with abundant boiling water and detergent (Limpol). After that, the basal surfaces of twenty plastic teeth (ten Vivadent and ten Vitapan) were grooved with aluminum oxide particles (110µm) using an abrasive spurting device (Micron Etcher- Danville), approximately 3-cm distance, for 10 seconds. After this, acrylic resin was manipulated and packed in dough stage. The flasks were put under 1250 kgf for 8 hours and after, acrylic resin was processed for 9 hours, 74 °C, for 9 hours. Polymerization device was turned off and flasks remained in the polymerization device until reaching room temperature. Flasks were opened and samples were removed. After finishing and burnishing procedures, samples were stored in distilled water, at room temperature (Figure 8). Samples were separated in 8 groups, according to table 1. Mechanical test Literature showed some types of mechanical tests to evaluate bond strength (1626 (1974), ISO 3336 (1977), BS 3990 (1980), DIN 13907 (1983), ANSI/ADA 15 (1985). In the present study, JIS T 6506 (1989) was used because it is a recent test and represents clinical occurrences5. Mechanical test was carried by non-axial tensile force test, using an EMIC machine (model DL-2000, 50 kgf Trd 21 load, speed of 0.5 mm/min and 1.10 version of Mtest software) until failure. In order to facilitate and standardize the test, a metallic device (S) was used, so that tooth long axis formed a ±45º angle with the base of the EMIC machine (Figure 9). Results (kgf) were evaluated statistically with ANOVA (factorial) and Tukey's test (5% significance). Results Tables 2, 3 and 4 and figures 10, 11 and 12 show the average values of bond stregth. When Vitapan teeth were used, there was no statisticaly significant difference between surface treated and untreated teeth (p>.05). Also, there was no statiscaly significant difference between Classico and Triplex Hot resins (p>.05) (table 2 and figure 10). When surface treatment was carried in Vivadent teeth, there was no statisticaly significant difference between Classico and Triplex Hot resins (p>.05). However, there were statisticaly significant differences between Classico and Triplex Hot resins (p<.05) for Vivadent teeth that did not receive surface treatment. In this case, Triplex Hot resin showed a higher bond strength. When analysing just surface treatment, there was no statisticaly significant difference between treated and untreated teeth, for both resins (p>.05) (table 3 and figure 11). Comparing Vitapan and Vivadent teeth, independetly of resin brands and surface treatment, there was no statistically significant difference between tooth brands (p>.05) (table 4 and figure 12). Discussion Many studies were carried to determine the quality of tooth/denture base bond. However, critical analysis of these studies becomes a difficult task because tests and samples used were not standardized. Bond failures between tooth and denture base represent a problem for rehabilitation success. In order to minimize these failures, many authors described main factors that can influence in bond strength: tooth types and brands7,9,12,15; resin types and brands8,13; stress distribution4-5; temperature of processing14; resin stage1 and processing variables6, 16. Cunningham and Benington4 and Thean et al.17 affirmed that bond failures between denture base material and plastic teeth remained a significant problem for treatment success and that wax or sodium algitate-contaminated surfaces produced highly significant weaker bonds. Already Kawara et al.6 and Darbar et al.7-8 affirmed that bond failures were probably caused by gap and crack propagation in areas of load concentration. Obtained results demonstrated that tooth surface treatment by grooving (with 110-µm aluminum oxide particles) showed no statistically significant differences (p>.05). Other authors defended that surface treatment by grooving improved bond strength9,11. Many authors related the effect of chemical surface treatment. Application of VEMA and a color agent did not influence bond strength. However, MMA reduced tooth/denture base bond16,18. On the other hand, Leles et al.19 told that the application of the MMA increased adhesive force. Cunningham12 and Takahashi et al.13 recommended the application of dichloromethane in tooth surface before processing. Studies that used the same tooth and acrylic resin commercial brands used in the present study were not found. There was no statistically significant difference (p>.05) between Classico and Triplex Hot resins when Vitapan teeth were used. When Vivadent teeth were grooved (surface treatment) there was no difference between Classico and Triplex Hot resins (p>.05). However, when Vivadent teeth were not grooved, there were statistically significant differences (p<.05) between Classico and Triplex Hot resins. When Vivadent teeth (without surface treatment) and Triplex Hot resin were used, higher bond strength values were obtained, probably because of a better chemical interaction between the two materials, since they are from the same manufacturer (Ivoclar). The following can be concluded: (1) there were statistically significant differences among Vitapan teeth and the other groups; (2) Vivadent teeth that did not receive surface treatment showed higher bond strength values when Triplex Hot resin was used; (3) surface treatment did not modify bond strength values. AcknowledgementsWe wish to thank FAPESP for the grant to support this study (Process 02/00624-0) References
Copyright 2004 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}