 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 3, No. 9, April/June 2004, pp. 475-478 Addison's disease associated to paracocidioidomycosis Claudio Maranhão Pereira3 Silmara Regina Silva1 Priscila Spaziane Camargo1 Andrea Mantesso2 Rodrigo Calado Nunes Souza 1 1Dentistry Section, Municipal Healthy Service, Campinas-SP, Brazil 2Oral Pathology, São Leopoldo Mandic Dental Research Institute, Campinas-SP, Brazil 3Oral Pathology, School of Dentistry of Piracicaba, UNICAMP, São Paulo, Brazil Correspondence to:Claudio Maranhão Pereira, Faculdade de Odontologia de Piracicaba-UNICAMP, Semiologia e Patologia Oral -Diagnóstico Oral, Av. Limeira, 901 -Areião - Caixa Postal 52, CEP: 13414-900 - Piracicaba/SP - Brazil + 55 19 3412 5213; Fax: + 55 19 3412 5218,E-mail: claudiomaranhao@hotmail.com Code Number: os04018 Abstract Paracoccidioidomycosis is a deep mycosis caused by the Paracoccidioides brasiliensis and it has been considered the most
frequent
systemic mycosis in Latin America. Mulberry-like ulcers on the
oral mucous membranes are one of the earliest manifestations of the
disease. Infection may remain subclinical, localized or disseminate occasionally.
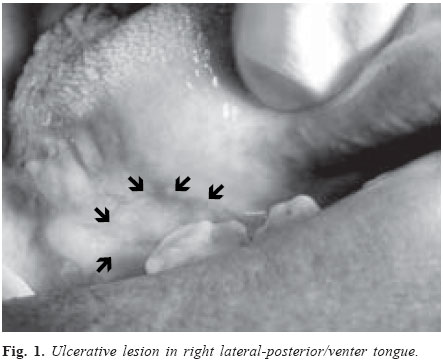
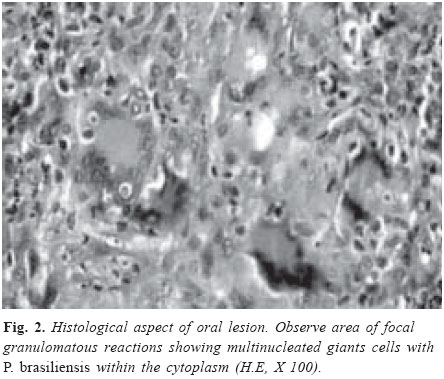
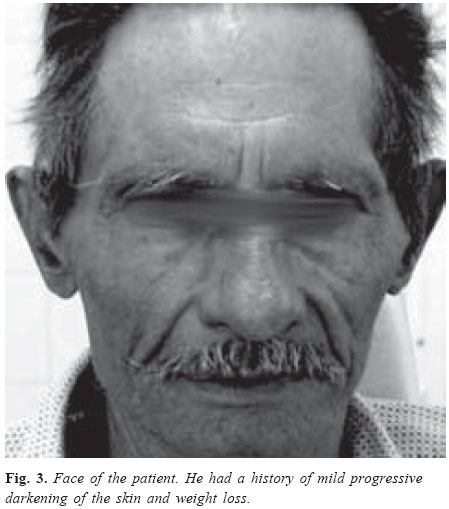
Key Words: Addison’s disease, paracoccidioidomycosis, adrenal glands. Introduction Paracoccidioidomycosis (South America blastomycosis) is a chronic mycosis disease caused by the dimorphic fungus Paracoccidioides brasiliensis1-2. Geographic fungal distribution is restricted to Latin America where it is considered the most prevalent systemic mycosis3-5. It is still relatively unknown in the United States and Europe4,6. P. brasiliensis may grow in the soil, in water, on plants in rural areas, and reaches the human host by the inhalation of airbone propagules5. Ninety per cent of cases have occurred in males patients with rural activities7, and peak incidence in the 30 to 50 year age group1-2,6. The disease has many clinical forms, particularly lymph node and pulmonary involvements as well as mixed forms1, 2, 8, 9. One of the early and more frequent manifestations is the presence of mulberry-like ulcers on the oral mucous membranes2,7,10-11. Infection may remain subclinical, localized or may occasionally disseminate6,12. Hematogenous dissemination of paracoccidioidomycosis to abdominal lymph nodes, spleen, liver, adrenal glands, skin, or brain can result in life-threatening complications1,4,9. Adrenal glands involvement has been documented and postmortem studies report adrenal abnormalities in 44 to 80% of cases13-15. Paracoccidioidomycosis is regularly associated with adrenal insufficiency in 10-15% of symptomatic cases14-16. Although the involvement of the adrenal glands for P. brasiliensis is not uncommon, there is not many cases reported Addison’s disease associated to oral paracoccidioidomycosis. A case of oral paracoccidioidomycosis with involvement of adrenal glands is reported herein. Clinical caseA 61-year-old male was referred to the Municipal Dentistry Service of Campinas-SP, Brazil, in November 2001, complaining about a painful ulcerative lesion on the right posterior-lateral/venter tongue lasting 2 months. The patient had a 3-week history of mild progressive darkening of the skin, dysphagia and weight loss. He smoked for more than 30 years. On clinical examination, the patient had a 2.0 X 2.0 cm ulcer on the right lateral/venter tongue. The ulcer had a granular surface with little inflammatory halo (Figure 1). With clinical diagnosis was squamous carcinoma, the patient was submitted to an incisional biopsy. The microscopic examination showed non-necrotizing granulomas with abundant multinucleated giant cells in the conjunctive tissue, and zones of pseudoepitheliomatous hyperplasia (Figure 2). Yeast-like organisms with thick capsules in multiple budding forms were observed by special stain SPA (Schiff's periodic acid). The clinicopathological features allowed the diagnosis of paracocidioidomycosis. After diagnosis, chest radiographs were made and confirmed pulmonary involvement. The patient was referred to the Municipal Center of Infect Disease for further management of his systemic disease. At the moment, it was suspected involvement of the adrenal glands due to the history of progressive skin darkening, dysphagia and weight loss (Figure 3). After hormonal level exams of adrenal glands, that showed low basal steroid levels and lack of response to ACTH (adrenocorticotropic hormone) therapy, the diagnosis of Addison's disease caused by P. brasiliensis was made. The patient was treated with steroids, sulfa and, after 5 months, the oral lesion resolved, but the clinical features of adrenal complications yet persist. The patient was not returned to the Medical Service for follow-up. DiscussionIt is generally accepted that in typical Addison’s disease, the destructive lesion of the adrenal glands must be of a chronic progressive nature such as might be associated with amyloidosis, tumor formation, tuberculosis, and other infectious diseases16-18. Adrenal involvement by granulomatous diseases is the main cause of the gland insufficiency in Brazil1,14, but infectious forms of the Addison's disease are relatively rare in the United States18. Among these, paracoccidioidomycosis is considered the most prevalent systemic mycosis in Latin America1,3,14.Paracoccidioides brasiliensis exhibits a high tropism for the adrenal glands which results in a low hormone reserve and, in more severe cases, in symptoms of primary adrenal insufficiency19. Adrenal involvement has been demonstrated in 21% to 80% of autopsy cases20. Azevedo21, in 1934, was the first to report one case with extensive necrotic changes in adrenal gland caused by P. brasiliensis. Del Negro14, 1961, reported involvement of the adrenal glands in 3 paracocidioidomycosis patients autopsied in study with 27 individuals. Several reports have described adrenal dysfunction in paracocidioidomycosis. These studies usually focused on cortisol responses to synthetic ACTH (adrenocorticotropic hormone) administration and established graded impairment of adrenal dysfunction13-14,22. Because differing methodologies were used to interpret the data, comparisons are difficult. Adrenocortical hypofuction associated with disseminated P. brasiliensis could be detected in 22% to 48% of patients, with a 9% to 14% prevalence of symptomatic Addison's 14,19,22. Colombo et al4, 1994, reported hypofunction of adrenal glands in only 14% of patients with disseminated paracoccidioidomycosis. The higher prevalence of adrenocortical hypofunction is associated with the disseminated forms of paracoccidioidomycosis; however, the possibility of exclusive adrenal involvement as the sole manifestation of the disease has been demonstrated14,16-17. The relationship between the pathogenetic factors of paracocidioidomycosis and adrenocortical hormones has not been explored. In recent years, many studies have documented that numerous cytokine family members influence the secretory activity of the hypothalamic-pituitary-adrenal (HPA) axis, which generally inhibit or modulate inflammation through the immunossuppressive effects of the glucocorticoids23. More recently, the adrenal androgen dehydroepiandrosterone sulfate (DHEA-S) was implicated as an immunomodulator hormone24. Leal et al.25 (2003) examined the functional status of adrenocortical hormones and their relationship with inflammatory cytokine patterns in patients with active paracocidioidomycosis. Their findings demonstrate a significant inverse correlation between DHEA-S and interleucine-6 plasma levels in paracocidioidomycosis, which may be of pathogenetic significance in this and others inflammatory diseases25. Although the typical oral paracoccidioidomycosis lesions consist of multiples mulberry-like ulcers in palate, gums, buccal mucosa, lips, and tongue, the patient reported herein showed only one ulcerative lesion with granulomatous surface and inflammatory halo. These clinical features, associated with chronic smoking and drinking habits, lead to a wrong clinical diagnosis of squamous carcinoma. On the other hand, with definitive diagnosis of paracoccidioidomycosis, it was possible to suspect of adrenal glands involvement due to the patient had history of mild progressive darkening of the skin, dysphagia and weight loss. Paracoccidioidomycosis is most relevant to dentistry because lesions may involve especially the head and neck, typically the oral and nasal mucosa, and facial skin2. In spite of not being rare the involvement of the adrenal glands for the P. brasiliensis, it was not possible to find in the literature a similar case that the oral paracoccidoidomycosis lesion provided the diagnosis of mycosis disease disseminated with secondary Addison’s disease caused by P. brasiliensis. The patient reported herein received diagnosis of paracoccidioidomycosis and Addison’s disease due to one oral lesion. It was confirmed the value of dentistry on systemic diseases diagnosis. References
Copyright 2004 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}