 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences,Vol. 3, No. 10, July/September, pp. 480-483 Chronic pain - a psychological approach Maria da Graça Rodrigues Bérzin MS in Clinical Psychology, PUC/RS Graduate Student, Piracicaba Dental School, State University of Campinas São Paulo, Brazil Received for publication: June
30, 2004 Code Number: os04020 Abstract The article presents some relative considerations of bio-psycho-social nature to chronic pain, emphasizing to Temporomandibular Disorders (TMD). It describes some consequences triggered by chronic pain on the every life and points the main psychodynamic characteristics of the TMD carrier. It still stresses the necessity of a diagnostic and therapeutical interdisciplinary and personalized approach, and the importance of a adequate preparation of the health professionals in general, regarding the methods and appropriate cares, destined to patients bearing painful syndromes. The good relation between professional and patient is pointed as one of the most important tools of work that makes possible more efficient and human treatments. Key Words:chronic pain; temporomandibular disorder (TMD); psychodinamic characteristics; interdisciplinary approach; personal and professional requirements.
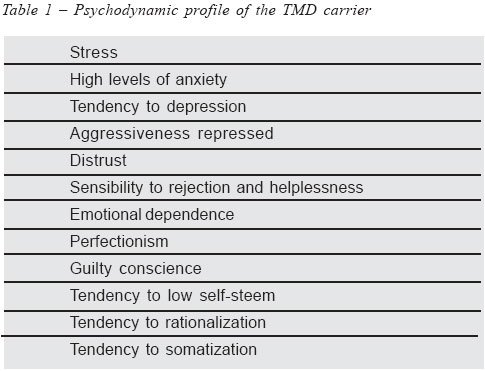
“Listen carefully, consider all the possibilities, cure if you can, refer if can´t, but always consoles” Pain is one of the greatest concerns of humanity and has been for years the subject of scientific studies. The literature on pain is vast and this subject is approached from various angles1-2. However, despite technological advances and a better understanding of pain, which has contributed greatly to its diagnosis and treatment, there is currently a progressive increase in the incidence of chronic pain in many clinical pictures, such as temporomandibular dysfunction (TMD)3. At the same time, it can be seen that professionals involved in this area are confronted with barriers and difficulties in relation to patients with this painful syndrome. The aim of this paper is to present some considerations on the bio-psychosocial nature of chronic pain in general and to point out some observed tendencies in the technical training and personal profile of health professionals that could explain some difficulties in the perception of chronic pain as a complex phenomenon. Such difficulties consequently can result in the adoption of inadequate diagnostic and therapeutic approaches to pain pictures. They are among the factors that explain the high indices of treatment failure, aggravation of clinical picture, and unnecessary physical and emotional suffering of patients, as frequently occur among those with TMD4. In general, many aspects can contribute in some form to the progressive increase in the incidence of chronic pain in our society. The development of technological resources of diagnosis and treatment have contributed for the increase in longevity and survival of numerous individuals with diseases until recently considered fatal. Living longer, however, does not necessarily mean living better. The characteristics of our physical environment, which are not always ergonomic and full of architectural barriers that hamper good posture, mobility and the safety of people are factors that promote physical pain to become chronic. Stressful factors of modern life, such as inadequate diet, sedentary habits, long hours at work, professional competitiveness, economic and family difficulties, lack of leisure, and loneliness, contribute greatly to the increase of chronic pain indices. Patients with TMD often refer to this scenario as the way of everyday life, beyond to present a typical psychodynamic profile5-6 (Table 1). Although all the above are important, it is still necessary to better understand the reasons for which chronic pain has been so poorly understood and managed in Brazil, despite that the significance of pain prevention as a fundamental condition for the satisfactory clinical recuperation of many patients has been widely acknowledged for more than 10 years7. The complex nature of pain itself should be considered as an attenuating factor, with its subjective expression, its large diversity of presentation, and it being the result of innumerable causal factors8- 9. However, it is worth recalling that besides nociceptive stimulus and the perception of pain in the nervous system, chronic pain appears to be a significant part of humanexperience known as suffering. Suffering is expressed through objective behavior signs that need to be considered and comprehended by health professionals10. Suffering caused by persistent pain, known as chronic pain, which causes damage to the psyche and life of the patient, can be understood based on three points of view. The existential is when pain represents a threat or impediment to the realization of a project in life. The circumstantial is when pain stimulates feelings of threat by external situations such as medical examinations, relations with the medical team and iatrogenic risk. Finally, suffering imposed by pain evokes pre-existing experiences, exacerbating emotional or prior family conflicts11. There are many consequences of chronic pain in the lives of people6. It can unleash, for example, feelings such distress, fear, anxiety, rage, irritability, sadness and lack of confidence. It also limits physical activity, makes family and social living difficult, alters body perception, damages emotional and cognitive resources, inhibits sexual appetite, compromises self-esteem, increases feelings of social and professional rejection, alters the system of beliefs and produces concerns about the future. Besides all this, it worsens the quality of sleep, aggravating general health conditions. This in turn compromises the view and management of pain, in addition to aggravating pre-existing diseases and weakening the immune system. Because of so many unfavorable conditions that affect in many ways the life of the patient with chronic pain, its diagnostic and therapeutic approach is never easy. This is particularly observed in the TMD clinic5,12 . Living a long time with pain stimulates cognitive and emotional conflicts that determine different patterns of behavior in the patient, that in turn can make treatment difficult and even undermines it13. Therefore, the first step in the direction toward the effective therapy for the individual with chronic pain is to consider the relation between the professional and the patient, and the first and perhaps foremost being the study tool. A good professional relationship should not be established primarily between symptom and technique. It should, above all, signify an encounter between two persons, that is, one who is ill and is suffering and one who feels and cares. For more than 50 years, pain has been studied based on an interdisciplinary concept. The etiology of pain has thereby come to be viewed from a bio-psychosocial focus14. Therefore, some modern authors when referring to the treatment of TMD recommend not only an interdisciplinary approach, but also specific care of each patient15-16. In this case the question of therapeutic relationship becomes even more important. The health team should actually be interdisciplinary and perform in harmony in relation to the clinical necessities of the patient, who in turn should feel like a part as well, participating actively in his/her treatment17. Keep in mind that patients,despite their suffering, can and should be stimulated and encouraged to utilize their cognitive affective and behavioral resources in confronting their problems18. The health team should thereby be informed with respect to the differences between acute and chronic pain and to the methods and appropriate care in handling the patient with pain. It should not have a fragmented view of pain, which is often seen due to the excessive focus in the specialization of health areas. This includes the insistence of the empirical utilization of medications (types, doses and inadequate intervals), and also the adoption of excessively technical approaches, leading to the detriment of dignity in treatment19-20. Finally, some personal and professional requisites appear to be necessary and can contribute to a more adequate and efficient performance by those practicing in the area of pain21,22. A good theoretical-technical academic training is important and helps the professional to avoid stereotypes. It should also help the professional to be tolerant and humble, so as not to be drawn toward poorly known and accepted, scientific and clinical understanding. However, from a personal point of view, it is expected that the professional be capable of handling frustrations and creating positive ties with the patient, despite resistance and sometimes lack of confidence on the part of the patient. Therefore, the health professional should have the capacity for empathy, to support and handle the various forms of suffering, without ever losing sight of the important and simple gesture of “opening up to the patient,” so that the patient in the midst of his/her misfortunes, can at least be spared from experiencing one of the worst pains, that is, of being misunderstood and not respected as a person. Acknowledgments The author wishes to thank Dra. Dagmar de Paula Queluz Administrative Editor and Dr. Sergio Roberto Peres Line, Scientific Editor of Brazilian Journal of Oral Sciences for the helpful correction of technical presentation and English revision of this manuscript. References
The following images related to this document are available:Photo images[os04020t1.jpg] |
| |||||||||

{kind=link}