 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
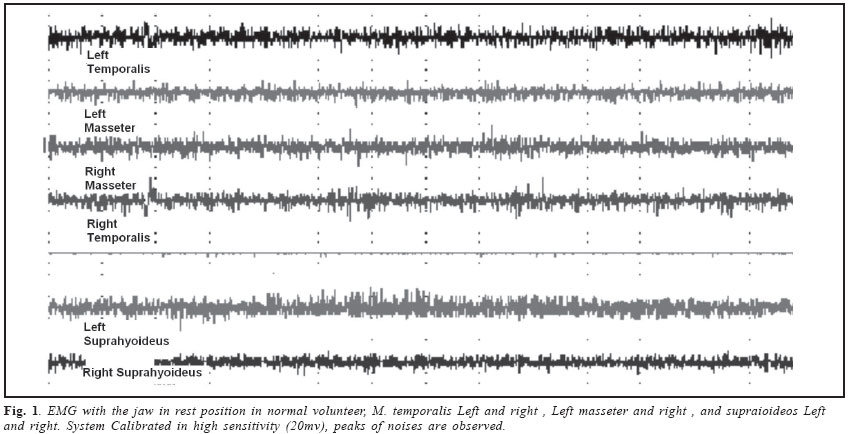
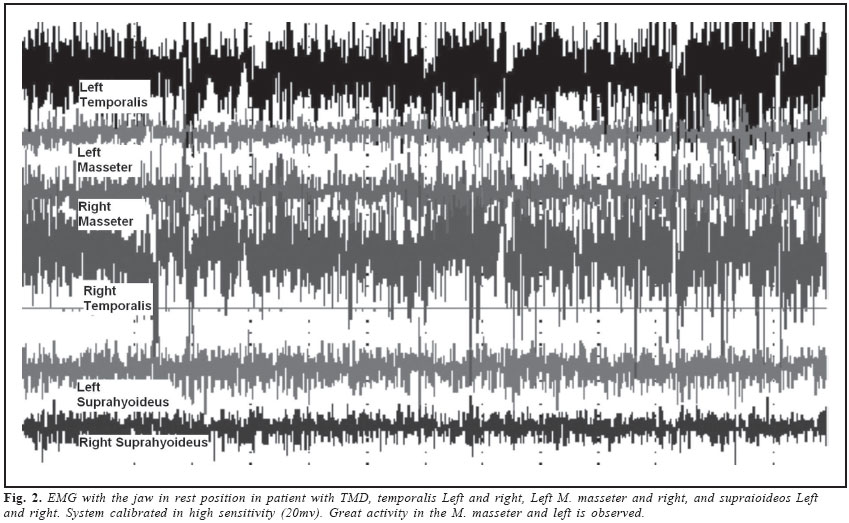
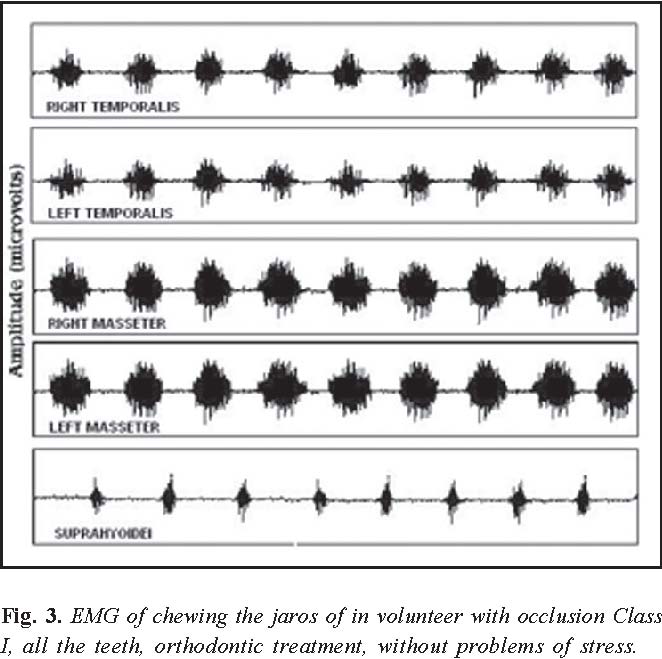
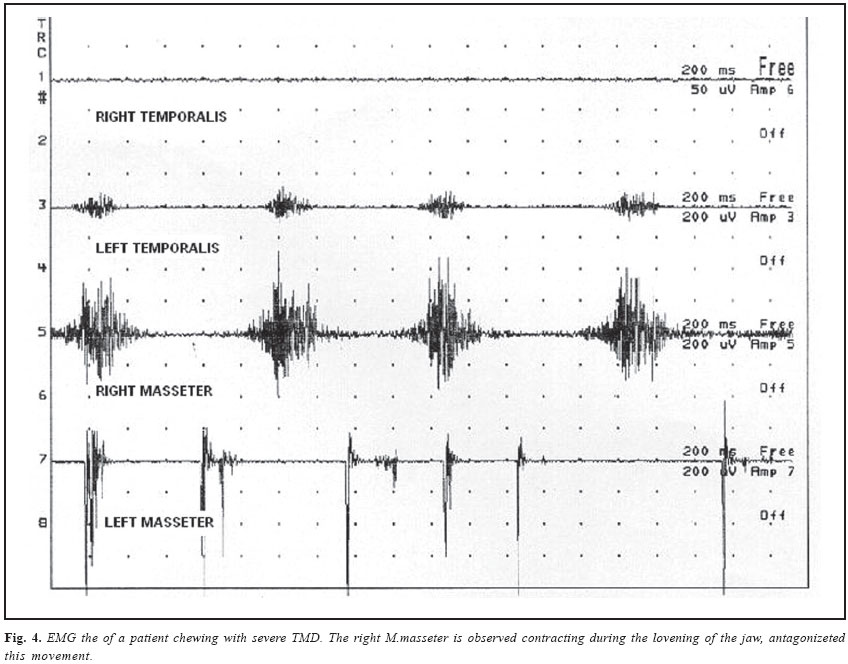
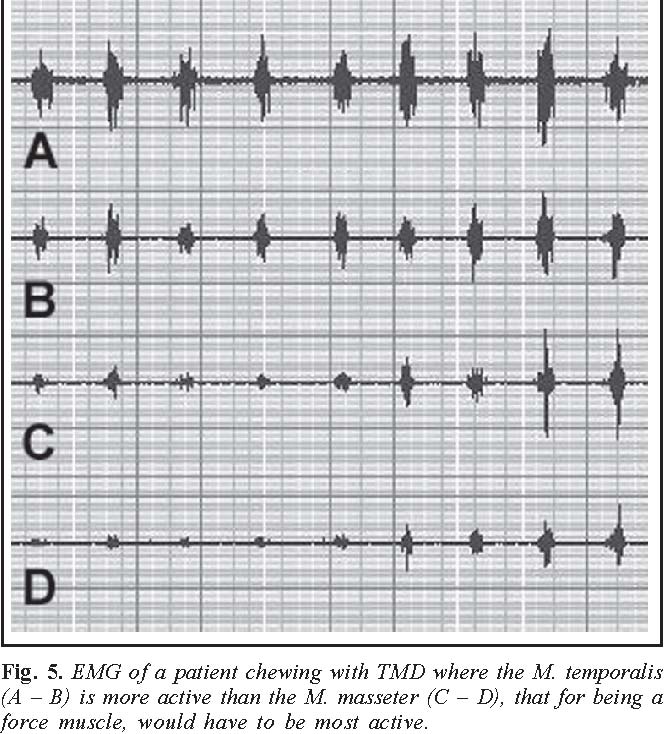
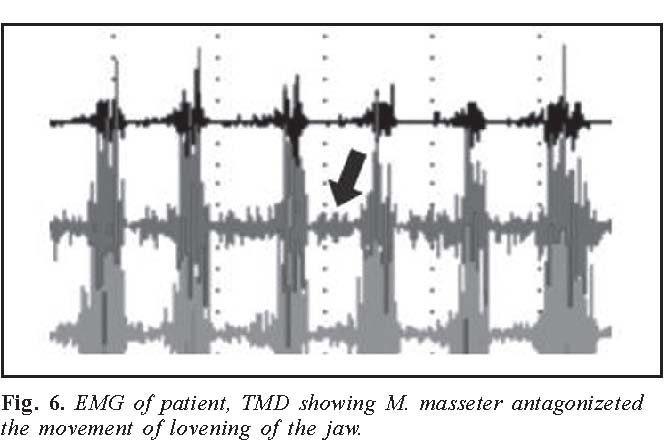
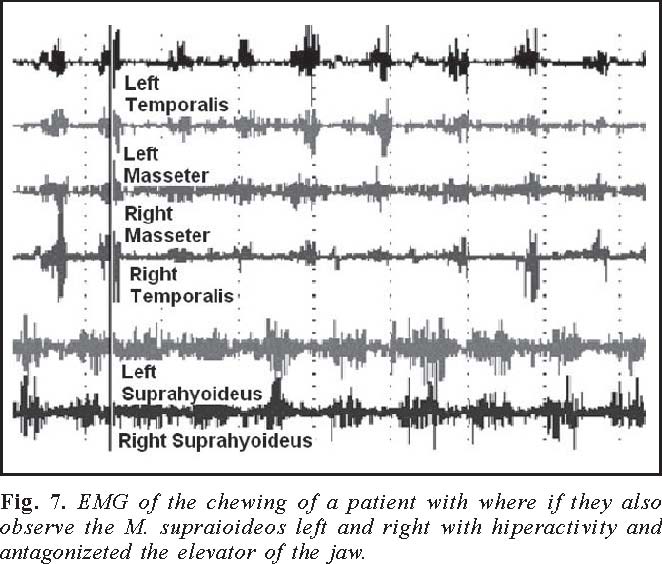
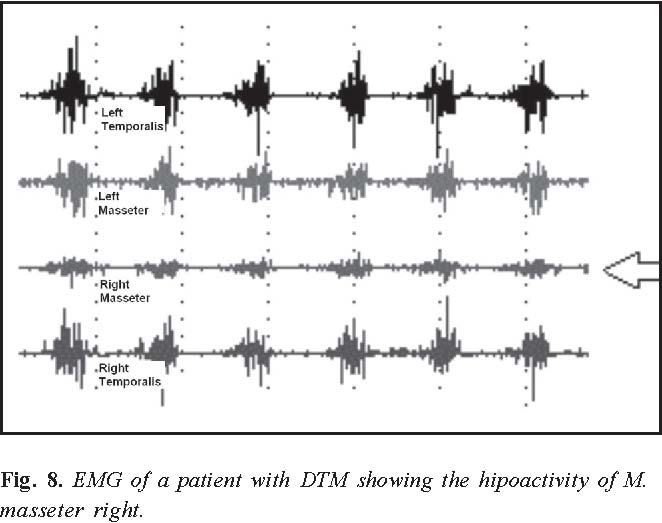
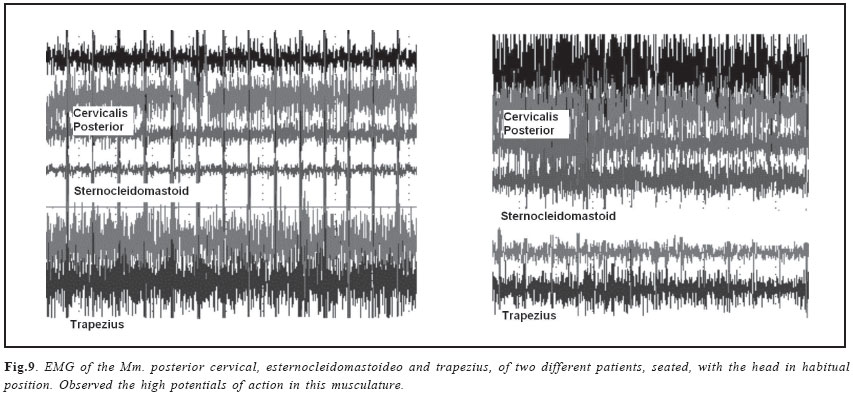
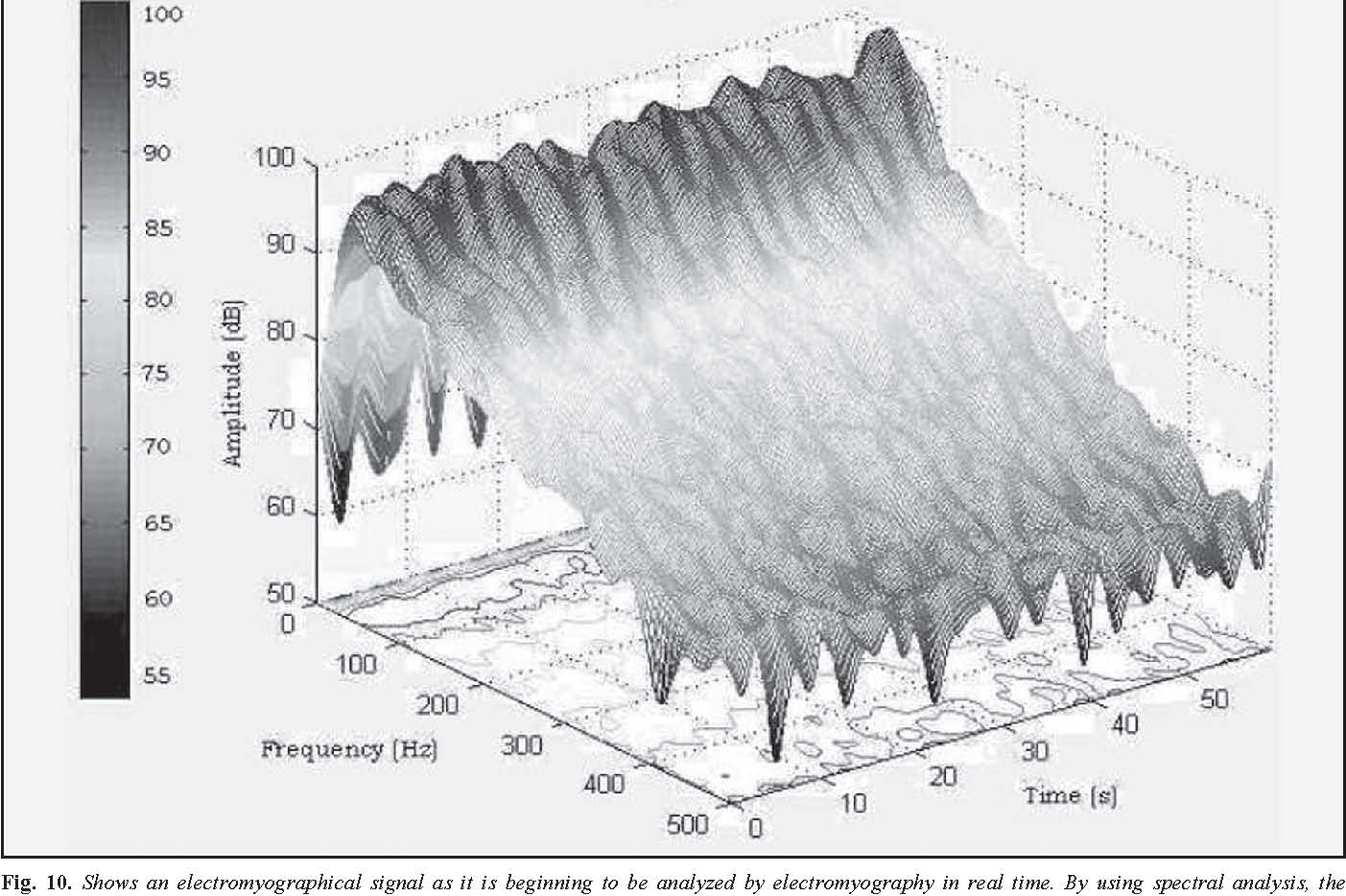
Brazilian Journal of Oral Sciences,Vol. 3, No. 10, July/September 2004, , pp. 480-483 Surface eletromiography in the diagnosis of syndromes of the cranio-cervical pain Fausto Bérzin DDS, PhD, Dean Professor, Department of Morphology, Piracicaba Dental School, State University of Campinas, São Paulo, Brazil Correspondence to: Fausto Bérzin, Faculdade de Odontologia de Piracicaba-UNICAMP Av. Limeira, nº 901, Areião CEP: 13414-903, Piracicaba, SP, Brasil Fone: (55) (19) 3412-5336 Fax: (55) (19) 3412-5218 e-mail: berzin@fop.unicamp.br Received for publication: May 30, 2004 Code Number: os04021 Abstract This paper first provides a review of the anatomy and physiology of striated muscles, focusing on the muscle fiber, motor unit and μ neuron. We also commented on the factors that affect the depolarization of this neuron, resulting in its excitation or inhibition, and thereby altering the contractions of the motor unit, which in turn alters the equilibrium of the muscle dynamics. The changes caused by these factors, such as muscular hyperactivity, found mainly in the temporal muscles, with the jaw the resting position and chewing are also discussed. However, muscular hypoactivity is most frequently observed in the masseter muscles. The suprahyoid muscles, responsible for the positioning of the tongue, also show a large number of alterations. We also commented on the changes observed in the contractions of the posterior cranio-cervical musculature, sternocleidomastoid muscles and the upper fibers the trapezius, which are sources of referred pain. Key Words: electromyography, chewing, masticatory muscle, pain, TMD Eletromiography is a seductive Muse because it provides easy access, it’s destriment, electromyography is easy to use and consequently easy to abuse. Electromyography Today Electromyography associated with the medical field is referred to as electroneuromyography in Brazil. It involves the study of the velocity of nerve conduction, motor units and morphology of their action potential, the presence of this potential in muscles at rest, and the study of evoked potentials. Electromyography is considered an auxiliary tool in the diagnosis of pathologies connected to the nervous and muscular systems. Another aspect of electromyography involves the physiological study of muscles and nerves, related to the individual structures that comprise them. With the tremendous development of electronic equipment during World War II (1939-1945), some studies led to changes in spectrum electromyography, contributing to a major advance in the electromyography focus known as kinesiological electromyography, which employs preferentially surface electrodes. With the advent of informatics, data acquisition systems for muscle potentials, which were previously analog, became digital. This facilitated data handling and diminished instrument costs, which thereby provided various professionals access to this new diagnostic technique. Today, kinesiological electromyography is a tool for a vast number of specialties, such as dentistry, psychology, kinesiology, biomechanics, physiotherapy, speech pathology and audiology, occupation therapy, otorhinolaryngology, orthopedics and many others that require an objective parameter to evaluate muscular activity to plan therapeutic intervention and to also assess results. In the beginning, these applications in odontology were restricted to kinesiological studies of the masticatory musculature. Moyers1 was a pioneer in the application of electromyography in odontology. Today, however, its application is broader and more varied. The use of electromyography is spreading as an important aid in the diagnosis of TMD and the evaluation of its treatment. Although instrumentation is easy to manage, interpretation of the results requires training, capability of interpreting data and above all a totally unbiased position regarding the results. The latter is important in order not to produce a diagnosis that could indicate for example invasive intervention of ATMs when unneeded or even dangerous for this articulation. The diagnostic value of electromyography has been questioned because of the variability of results shown in numerous investigation due to the lack of standardized instruments, electrodes, and methods of signal acquisition and processing, and due to the lack of adequate understanding and training among the personnel involved in the studies. Therefore, the ISEK (International Society of Electromyography and Kinesiology), with the aim of standardizing these studies, as done earlier in the United States, established and published a series of norms, accessible at the website http://shogun.bu.edu/isek/ index.asp, which should be able to guide electromyography studies. In a recent publication, The European group SENIAM2 has also presented norms and recommendations for electromyography tests (as shown in a recent publication, European Recommendations for Surface Electromyography, 1999)2, which when adopted should minimize the variation in results. Muscle Contraction The functional unit of the muscle is called the motor unit. Each motor unit of a muscle is composed of an a motor neuron situated in the anterior horn of the gray matter of the spinal cord or in the motor nucleus of the cranial nerve, connected to a variable number of muscle fibers. The most popular idea is that when the muscle contracts, all of its fibers remain contracted during this state. However, what occurs is that this contraction does not proceed simultaneously in all of its fascicles. Updated concept to take into account is that a muscle fiber stays contracted for a period of at least 1 to 2 milliseconds, followed by a complete and rapid relaxation. Depending on the size of the motor unit, which varies for example from 2 fibers per a motor neuron for the right lateral external muscle of the eye, up to about 1700 for the gastrocnemius muscle, a motor unit of a normal muscle takes about 5 to 12 msec to contract all its fibers. During contraction, a normal muscle generates an electric potential with an amplitude of about 200 to 500 mVolts, when measured extracellularly. Therefore, in a contracting muscle, what is observed are contracted motor units (muscle fibers), to maintain isotonic or isometric muscular action. While some motor units are relaxing, others are contracting to maintain the action. In other motor units at rest during the refractory period, their fibers prepare to contract anew, so that new contractions and units are ready to be recruited to substitute for those beginning to relax This process produces electrical potentials continuously. Thus, muscular force can be controlled in two different ways: by increasing or decreasing the discharge frequency of the motor units, or if necessary by recruiting a larger number of motor units at the same time3. An a motor neuron, situated in the motor nucleus of the trigeminus nerve, receives about 10,000 synaptic terminals. Some of these terminals are excitatory, that is, the µ neuron thereby activates and depolarizes the muscle fibers of its motor unit, which in the case of the masticatory muscle involves between 700 and 900 fibers. It is possible that inhibitory synapses predominate, blocking the a motor neuron and causing each motor unit to cease from activating about 700 to 900 muscle fibers, which would cause hypoactivity in the innervated muscle. The a motor neuron of the motor nucleus of the trigeminal nerve receives influences from all levels of the Central Nervous System (CNS): cortex, limbic systems, nucleus of the base, cerebellum, substancia nigra, etc. Peripherally, through the sensitive nucleus of the spinal tract, this neuron undergoes influences from the facial, hypoglossal and vagus nerves, whose fibers make synapses in this nucleus and make connections with motor nucleus of the trigeminal nerve through the substancia nigra, which has the capacity to inhibit or weaken an impulse in various ways. As the sensitive nucleus of the spinal tract descends caudally through the spinal cord, it also receives influences from the cervical muscles, and transmits impulses that are indirectly amplified or attenuated to the a motor neurons in the motor nucleus the trigeminal nerve. Therefore, any proprioceptive or exteroceptive alteration of the region determines an action on the a motor neuron of the trigeminal nerve, which causes hyperactivity or hypoactivity in the muscles of mastication. Furthermore, this influence can be extended to a motor neurons of the anterior horn of the spinal cord, altering the kinesiology of the cervical muscles innervated by these a motor neurons4. Myogenic Myofacial Pain The theory proposed by Sherrington in 19065 states that the CNS keeps postural musculature in a state of semi-contraction even at rest. Such an idea was extended to all the muscles of the body, creating a wrong concept of muscle tone. This concept was definitively modified by modern studies using electromyography, which demonstrated conclusively that muscles at rest, do not show contractions of motor units. It also demonstrated that the µ motor neuron, which controls the motor units of a muscle, is inactive when a muscle is at rest6. With respect to the masticatory muscles, various authors have demonstrated the inactivity of the jaw elevator muscles in this condition7-11. The viscoelasticity of muscles and ligaments, sub-atmospheric pressure and the articular capsule should be sufficient to maintain the jaw in the resting position without muscular activity. The CNS would not depolarize µ neurons, but proprioception (neuromuscular fusions) would activate small random and infrequent discharges to maintain this condition, when there would be a need to reposition the jaw as gravity were to overcome little by little this static resistance to its lowering. Electromyography of Musculature of the Head and Neck To obtain a better recording, the examination of the musculature of this region should be conducted on two procedures: a) With the instrument calibrated at 20 µvolts per division, we study the muscles with the jaw in resting position. *It is not possible, due the presence of electrical signals from neighboring muscles because “cross talk,” to analyze separately the anterior belly of the digastric muscle using surface electrodes12 These are performed with previously moistened cotton Q-tips or Parafilm, which are products utilized to reduce the coefficient of variation in results13. 02) Next, with the patient seated, the posterior cervical, M.suboccipitales, (also impossible to individualize), sternocleidomastoid and trapezius (upper fibers) muscles are examined, using surface electrodes with the instrument calibrated at 20 µvolts. 2.1) Comments Rest: It was seen that in about 43% of the cases there was no electrical activity with the jaw in the resting position. In 57% of the cases, activity was seen in both isolated and combined muscles. The right and left temporal muscles are those most often showing electrical activity (70% and 56%, respectively), followed by the right (56%) and left (58%) suprahyoid muscles The right and left masseters are less often active, with respective frequencies of 48% and 47%. Not all patients with Temporomandibular Disorder (TMD) demonstrate muscle activity with the jaw in the resting position, but an incidence of 57% is substantial. EMG activity with the jaw in the resting position can cause muscle fatigue and pain. Since the right and left temporal muscles are the most active muscles with the jaw at rest, this could explain in the majority of cases the high incidence of pain in this region14. In mastication: The figure 3 shows the electrical tracing considered normal during chewing with occlusion Class I, where there was no orthodontic treatment, no missing teeth, no history of stress and good posture. It is noted from the tracing that the masseters are muscles that show the highest action potentials. Together with the medial pterygoid, they draw fibers to the edge of the jaw and are thus force muscles for jaw elevation, due the morphology of their fibers, which are short and arranged in an enclosed manner to effectively resist traction. It is also seen that the temporal muscles show weaker signals, since despite their size these muscles are positioners of the jaw and not muscles of force. It is seen that when there is electrical silence in the temporal and masseter muscles, a low activity is recorded in the suprahyoid musculature acting in the lowering of the jaw. The figure 4 illustrates the complete disorganization of this picture in a patient with TMD complaining of intense pain, with the right masseter appearing to be antagonizing the raising of the jaw. In the tracings of patients with headache, mainly in the temporal region, the temporal muscle shows uni- or bilateral action potentials that are greater than that of the masseters, assuming thereby the role of a muscle of force, for which it is not built (Figure 5). Another interesting observation in the patients is the activity of elevator muscles during the lowering of the jaw when they should be completely inactive (Figure 6). This action antagonizes the jaw-lowering muscles (lateral pterygoid and digastric), producing an overload due to the resistance to be overcome, which can cause pain. Notably, this activity disappears as well the associated pain when TENS is applied. Muscle hyperactivity never appears isolated during mastication. More than one muscle is always hyperactive in patients with TMD. There are 23 combinations of hyperactivity in the muscles studied. Twelve percent of the cases do not present with muscle hyperactivity. In 88%, hyperactivity is observed and among these about 46% show a predominance of hyperactivity in the anterior part of the temporal muscles, which could explain the episodes of headache, mainly in the temporal region. The masseter and suprahyoid muscles each show about 20% hyperactivity, suggesting alterations in jaw elevation respectively in the lingual positioning, which could be associated with aggravation of TMD. In the majority of cases (88%), myofascial pain can be associated with some type or a combination of different types of muscle hyperactivity. Given the complexity of these combinations, it is concluded that the planning of treatment for myogenic myofascial pain should be individualized, taking into account the muscle hyperactivity picture of each patient15. It is interesting to note that the suprahyoid muscles show hyperactivity parameters that are quite similar to those of the masseter muscles as seen in Figure 7. They can also act on the raising of the jaw by antagonizing the elevator muscles of the jaw, which can cause fatigue in both musculatures, even though its action can be easily overcome by the elevator muscle. This finding would explain the reduced incidence of overbite in their orthodontic and orthopedic treatment. Hypoactivity We can also see muscle hypoactivity in patients with pain. Despite that this has been extensively debated and sometimes repudiated, it can be seen in Figure 8 that the right masseter muscle shows a lower tracing (activity) than all the other muscles in the mastication cycle, signifying a fewer number of motor units recruited and consequently less force, which then overloads the homologous temporal muscle and even the contralateral masseter. Some kind of hypoactivity is observed in 22% of the cases in one muscle or more than one in 10 different combinations. The left and right masseter muscles show the most frequent hypoactivity (19.8%), on both sides, followed by the temporals, 8.8% for the left and 7.7% for the right. The suprahyoid muscles show a 2.2% incidence for both sides15 TMD is often associated with muscle hyperactivity, but can occur in the presence of hypoactive muscles, mainly the masseter muscles16. The latter can cause alterations in articular biomechanics that can lead to overload of the temporal muscles, which are positioners in the mandibular condyle, causing loss of chewing force, jaw deviations, pain and muscle fatigue. Considering the variety of combinations of hypoactive muscles found, the therapeutics of TMD lacks an specific and multidisciplinary approach that takes into account among other aspects the phenomenon of muscle hypoactivity. Examination of the neck musculature involves: The Figure 9 shows that there is a high activity in this musculature in the resting postural position of the patients17. The electrical activity recorded in this musculature suggests the presence of trigger points, comprised of tense bands, which give rise to reflex pain in upper regions, including pain in the form of an umbrella, which ascends through the neck, goes around the auricular pavilion and ends with top of umbrella situated above the ATM18 erroneously interpreted as indicative of surgical intervention in this articulation19. Figure 10 shows an electromyographical signal as it is beginning to be analyzed by electromyography in real-time. By using spectral analysis, the degree of muscle fatigue can also be inferred, among other aspects. ** Due to cross talk, it is not possible to examine individually the muscles studied using surface electrodes. Acknowledgments The author wishes to thank Dr. Sergio Roberto Peres Line, Scientific Editor of Brazilian Journal of Oral Sciences for the helpful correction of technical presentation and English revision of this manuscript. Also wishes to thank Joelma Aparecida Macchi that typed this work patiently and Susane Sperandio Brossi for the important aid in the EMG drawns. Acknowledgments The author wishes to thank Dr. Sergio Roberto Peres Line, Scientific Editor of Brazilian Journal of Oral Sciences for the helpful correction of technical presentation and English revision of this manuscript. Also wishes to thank Joelma Aparecida Macchi that typed this work patiently and Susane Sperandio Brossi for the important aid in the EMG drawns. References
Copyright 2004 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}