 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
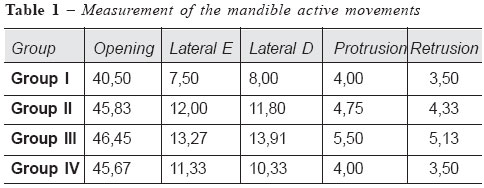
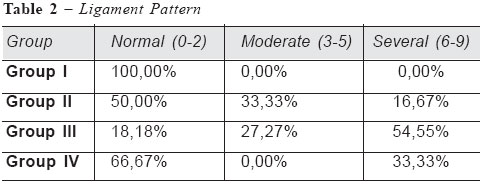
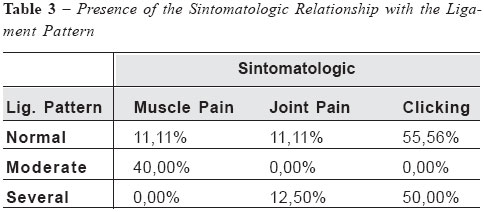
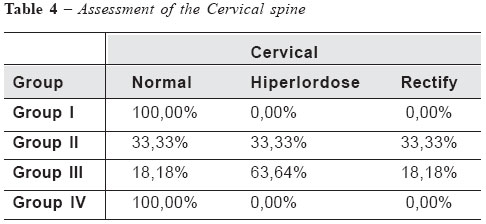
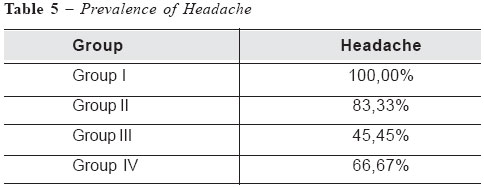
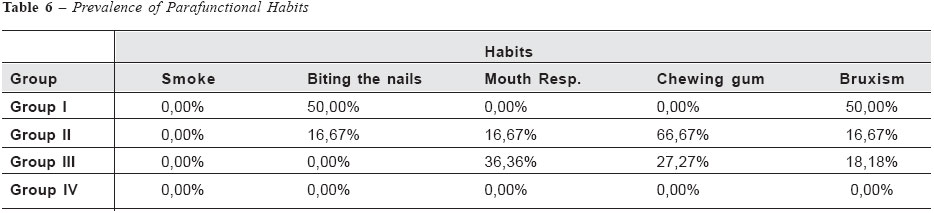
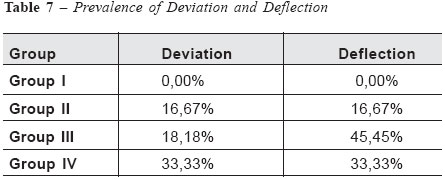
Brazilian Journal of Oral Sciences,Vol. 3, No. 10, July/September 2004, , pp. 522-525 Physiotherapy assessment of temporomandibular joint in pregnant women and prevalence of dysfunctional signs and symptoms Juliana P. Tosato, Daniela Ap. Biasotto-Gonzalez, Tabajara, O. Gonzalez. Department of Physical Therapy, University of Mogi of Cruzes, São Paulo, Brazil. Correspondence to: Juliana de Paiva Tosato Jacarandá st, 232 Condomínio Arujazinho IV 07400-000 Arujá - SP, Brazil Phone: 55 11 46541840 Email: julianadepaivatosato@ig.com.br Received for publication: February 23, 2004 Code Number: os04028 Abstract In the pregnancy many transformations and adaptations occur. These alterations can be predisposing factors to Temporomandibular Disorders (TMD), once the Temporomandibular Joint (TMJ) is vulnerable to intrinsic and extrinsic factors. The proposal of this study was to evaluate the TMJ of pregnant women, checking the prevalence of signs and symptoms of disorder in this joint. To accomplish the study, 22 pregnant were analyzed and divided in first, second, third trimester and those who have baby in the past three months. The dynamics of the mandible movements was observed and the higher amplitude was found in the third trimester. Was noted in the same group a generalized hipermobility and signs of Temporomandibular Disorders, including muscular pain and joint symptoms. It was also observed cervical posture alterations which could be responsible for the presence of symptoms in the others trimesters. Parafunctional habits were also checked in all groups. Therefore, the adaptations presented in the pregnant women such as joint hipermobility, posture alteration, and other modifications can influence the TMJ biomechanic, provoking TMD in pregnant women and in other people who also present these disturbances. Key Words: pregnant, temporomandibular disorders, hipermobility. IntroductionThe pregnancy is a normal physiologic episode in the woman’s life, and for this, the entire organism prepares itself, experiencing transformations and adaptations1. These alterations act as predispose factors to Temporomandibular Disorders (TMD). Studies proving this relationship cannot be found, but the influence of these modifications in the stomatognathic system is know to people in general (not pregnant women), once the Temporomandibular Joint (TMJ) is vulnerable to intrinsic and extrinsic factors2. The posture alteration, caused by the uterus volume expansion, interferes in adjacent regions, due to the fact that the human body segments are anatomically and functionally related3. The head posture modification influences the position of the mandible4-5. Consequently, this can change the occlusion and the masticatory muscles, affecting the TMJ6. Also, the tension of the posterior cervical muscles can compress the occipital nerve, causing a headache7. The hipermobility present in the pregnant women, due to the hormonal alterations, can provoke TMD, because the changes in condyle movement, predispose the TMJ to overload8. This factor allows temporomandibular hipermobility, which can be localized or part of a generalized hipermobility syndrome. Some signs and symptoms are frequent in these patients, including: excessive joint mobility, lateral deviation of the mandible during elevation or depression, clicking, pain in TMJ, and pain in the masticatory muscles6. A study analyzed the frequency of the generalized joint hipermobility in symptomatic and asymptomatic subjects, and a significant statistical difference between the two groups was noticed. The symptomatic group presented the greatest prevalence of hipermobility joint, while in the asymptomatic group, physiologic found predominated9. Psychological modification is common in pregnant women. The emotional factors had also been studied, and it can cause TMD10-12. This disorder includes pain and functional alterations in the masticatory system13. Muscle and joint pain, clicking, humming, headache and other signs and symptoms are common2,6,14-15. Therefore, the TMD diagnostic is not simple, requiring the comprehension of the principles on diverse areas16, It also is very important to consider in the TMJ assessment the joint and the muscles involved, the posture, and the patient’s ligament characteristics and clinical history6. The proposal of this work is also assess the TMJ of pregnant subjects, checking the prevalence of signs and symptoms of disorder in this referred joint. Material and MethodsVolunteers Group I: two subjects in the first trimester of pregnancy. To be included in this study, the pregnant subjects could not present any risk of pregnancy. To achieve this research, a TMJ physiotherapeutic assessment protocol was used, which was developed by Biasotto-Gonzalez . Conducts The assessment began with the collection of the volunteers personal information, including the trimester of pregnancy. After collecting the clinical history, the major complains were checked: pain in the TMJ, headache, humming, clicking, and other symptoms, along with the presence of parafunctional habits such as bruxism, biting the nails, smoking, and chewing gums. Finishing this step, the palpation of the condilar movements was preformed, observing if the volunteer had deviations or deflections. The palpation of the masticatory muscles, including the temporalis, masseters, medial and lateral pterygoids. Was also done, along with the measurement of mandibule opening, lateral movements, protrusion and retrusion. Finally, the assessment of the ligamentar pattern was performed with specific tests. After these tests, the patients were considered with normal ligament pattern, moderate hipermobility or severe hipermobility. More over, the cervical posture was also assessed. Results and DiscussionTable 1 shows the values obtained in the measurement of the mandible movements. It is noted that an increased in all variations occurs until the third trimester. And in the group IV, the mean values declined. Table 2 indicates the ligament pattern presented by the pregnant subjects. It can be noted that in Group I, 100,00% of the volunteers presented a score between zero and two, indicating a normal ligament pattern. In the Group II, the prevalence of score between zero and two was high, (50,00%), but the score between three and five was noted, along with a smaller proportion of scores between six and nine. In the Group III, 54,55% obtained the scores between six and nine, classifying these pregnant women with a severe hipermobility. Furthermore, the Group IV predominance was the subjects with normal ligament pattern (66,67%). These data collected is justified by the hormonal influence in the joints17. Some authors defend the idea that the peak ligament hipermobility occur in the last weeks of the pregnancy. But other authors explain that the Relaxin concentration which is responsible for these alterations, increase in the first trimester and decrease in the second trimester of pregnancy18. The biggest amplitude of the mandible movements along with the alteration in the ligament pattern suggest that the TMJ is also concomitant with the generalized ligament hipermobility Table 3 illustrate the presence of symptoms in the different ligament pattern groups it was observed. In the pregnant subjects with normal joint mobility, and also on the ones with severe ligament hipermobility, a high predominance of joint involvement, including pain in the TMJ, and presence of clicking. In the group with a moderate hipermobility, the pain in the masticatory muscles was more frequent. The muscular and articular symptoms can be caused by the ligamentar hipermobility, among other factors6. Now, the presence of changes in the group with normal ligament pattern is explained by other modifications presented in pregnancy, such as posture alterations, which affect the biomechanic joint5-6, and psychological factors. These psychological factors can act as predispose factors of TMD, responsible for the parafunctional habits such as bruxism, which decrease the intra articular space and generate muscular hyperactivity. The assessment of the cervical posture is demonstrated in Table 4. It is observed that 100% of the pregnant subjects in Group I and IV presented a normal posture of this body segment. There was a homogeneous distribution in the possible postures in Group II. Cervical hiperlordosis was predominant in the Group III, which was made of subjects in the third trimester (who also presents the biggest adaptations). Changes in the cervical posture influence the head leading to chronic headaches7. In Table 5, the prevalence of headache in all of groups is noted. This symptom is frequent in TMD patients6. Table 6 shows the prevalence of parafunctional habits. These habits cannot be found in the subjects of group IV. Table 7 demonstrated the assessment of condyle movements through the opening of the mouth. Group I did not present alterations. However, it was observer the presence of deviation or deflection in the other groups, indicating one diagnostic hypothesis of anterior dislocation of the disk. This sign is common in patients with hipermobility of the TMJ, which provoke instability of the joint8. According to the results of this study, it changes in the stomatognathic system were noted in the assessment of the pregnant women, with increase in the amplitude of the mandible movements, concomitant with the alteration in the ligament pattern and in the posture. TMD signs and symptoms were also observed, which proved the TMJ susceptible and its associated structures to modification of other systems. Acknowledgements The authors would like to thank to Guilherme Manna Cesar. References
Copyright 2004 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}