 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences,Vol. 3, No. 10, July/September 2004, , pp. 526-529 Electromyographic examination in temporomandibular disorders – evaluation protocol. Cristiane Rodrigues Pedroni, Cynthia Bicalho Borini, Fausto BérzinDepartment of Morphology, State University of Campinas - Piracicaba Dental School - Brazil Correspondence to: Cristiane Rodrigues Pedroni, Faculdade de Odontologia de Piracicaba -Departamento de Morfologia Avenida Limeira, 901 - Bairro Areião CEP. 13414-903 - Piracicaba - SP. Phone: (19) 3412-5336, E-mail: pedronicr@uol.com.br Received for publication: June 30, 2004 Code Number: os04029 Abstract Surface electromyography has been a useful tool for physicians and investigators to evaluate and diagnose temporomandibular disorders, to examine the role of masticatory muscles in specific tasks, and to verify the effect of therapeutic resources in temporomandibular disorders patients. However, the lack of standardization of the methods and equipment used during the surface electromyography examination has been the target of criticism among researchers. The purpose of this article is to describe the materials, equipment and surface electromyography protocol used to evaluate temporomandibular disorders patients at the Piracicaba Dental School - University of Campinas -Brazil. This experimental protocol is used successfully in the majority of cases seen in Electromyography Laboratory at Piracicaba Dental School. Key Words: electromyography, temporomandibular disorders, evaluation protocol Introduction Surface electromyography (EMG) has been a useful tool for physicians and investigators to evaluate muscular function. In clinical research, EMG has served as an important technique to investigate general muscle alterations, to determine the initiation of muscle activation, and to assess the coordination or imbalance of the different involved muscles in the study of the movement. It has been recognized as an important tool in temporomandibular disorders (TMD) diagnostics. It has been valuable in studying the role of masticatory muscles in specific tasks and determining the effect of therapeutic resources in TMD patients1-4. Therefore, EMG could be considered an effective evaluation method for therapeutic procedures related to muscle alterations. Important applications related to the use EMG could be a) the evaluation of movement coordination, b) establishment of motor unit recruitment patterns, and c) providing an index of the muscle fatigue process5. The International Society of Electrophysiology and Kinesiology (ISEK) has established standardized guidelines for electromyography evaluations, as determined in Standards for Reporting EMG Data6. The latter is an international standard document adopted by the scientific community, and its recommendations and instructions must be followed in general electromyography studies. According to Dahltrom7 and Lous et al.8 were the first to use EMG recordings in 1970 as an evaluation tool to assess masticatory muscle function in TMD patients. These investigators demonstrated that in the jaw rest position, the activity of the temporalis and masseter muscles was significantly higher in these individuals when compared to a control group. In studies involving TMD patients, EMG has been frequently carried out with the use of surface electrode to determine electrical activity at mandibular rest position and the hyper or hypoactivity of such muscles during rest, and to examine muscle balance during chewing, dental clenching and parafuncional activity. The most accepted hypothesis among scientific researchers involving the EMG activity of masticatory muscles is that the muscle activity necessary to keep the mandibular rest position is higher in TMD patients with myofacial pain than in control individuals8-11. Some authors have also investigated the relationship between masticatory muscles and head posture using electromyography12-13. It was observed that head position could modify masticatory muscle function14, and that changes in mandibular position can contribute to significant changes in the EMG activity of cervical muscles15. Many studies have been carried out to quantify the effect of odontologic treatments, including occlusal adjustment16-18 the repositioning and stabilizing of plates19-20, and evaluating parafunctional habits, such as in bruxism or occlusal alterations in TMD patients. Recent studies of physical therapy treatments for TMD have emphasized pre and post treatment electromyographic assessment, such as transcutaneous electrical nerve stimulation (TENS)3-4,17,21 and massage therapy2. The purpose of this article is to describe the materials, equipment and the EMG protocol to evaluate TMD patients seen at the Piracicaba Dental School (FOP/UNICAMP). Electromyographic EquipmentRecordings are made on 12 channels of simultaneous EMG signal (Myosystem I® equipment from Prosecon Ltda), 8 channels for EMG and 4 for support. The analog EMG signal is amplified, band-pass filtered with cut-off frequencies of 10Hz (high-pass) to 1500Hz (low-pass). The analog signals recorded are digitized using 12 bit A/D converter at a sampling rate of 2 to 4KHz. For data collection, the instrument gain is adjusted to 50 times. After digitalization, the signal is filtered again by a digital filter pass-band of 10Hz 500Hz. Myosystem I software version 2.12 is used to visualize and process the EMG signal. ElectrodesSkin surface active electrodes (Lynx Electronic Technology Ltda.) with a contact diameter of 10 x 2 mm, parallel bars of pure silver (Ag), spaced 10 mm apart and fixed to acrylic resin of 23 x 21 x 5 mm are used. Connecting cables of 1.5 meters and electrodes with an impedance of 10 GW, CMRR of 130 dB and gain of 100 are employed as well. With the use of differential electrodes, it is possible to amplify the EMG signal before it reached the equipment, thereby decreasing the amount of noise and interference. A circular stainless steel electrode 3 cm in diameter is interfaced to the skin surface with electrode paste and is placed on electrically inactive tissue (tendons or bony parts). For TMD EMG examination, the reference electrode is attached to the volunteer’s sternum at a distance from the muscles studied, according to the Standards for Reporting EMG Data6 by the International Society of Electrophysiology and Kinesiology. Faraday CageThe function of the electrostatic Faraday cage is to isolate the research environment from external electromagnetic fields, reducing noise sources that could influence the signal. EMG data collection is performed inside of an electrostatic Faraday cage 2.3m in height, 2.8 m in width and 2.6m in length. A copper screen coated its wooden structure. It is connected to 25 mm2 by its four corners and attached by 6 connecting rods. These connecting cooper rods are 5/6" by 2.40 m, and they formed a triangle structure. The feeding cables of the equipment are connected to two line filters and to one stabilizer linked to an electric socket of 127V, as for the Faraday cage. This connection is made to minimize interference due to the 60 Hz frequency supplied by the power line, which could have interfered with the EMG signal. EMG Examination During the whole EMG examination, the volunteers sit relaxed and upright in a straight-back chair without head support, with the Frankfurt occlusal plane parallel to the floor. They keep their eyes opened and arms on their legs. Electrode Placement ProceduresBefore electrode placement, the volunteer’s skin is previously cleaned with 70% alcohol. The electrodes are positioned in relation to muscle fiber length, with the silver bars positioned perpendicular to maximize signal capture and to minimize noise interference. The preferred location of the electrodes on the muscle is in the midline of the belly of the muscle between the nearest innervation zone and the myotendonous junction. It is not recommended that the electrode be placed next to the tendon region to prevent reduction of EMG signal or increase of frequency signal and the occurrence of crosstalk. Muscle function tests must be performed before electrode placement according to the positioning criteria described by Cram and Kasman22, which are as follow:
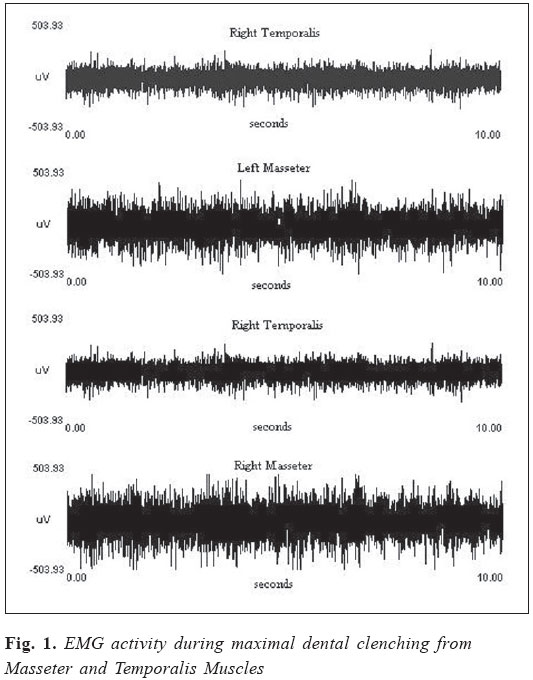
Electrodes are fixed with the use of double-sided Stampa® adhesive tape, placed between the skin and electrode capsule, keeping bars free for signal capture. EMG data aquisitionThe EMG activity is recorded during three situations: mandibular rest, during chewing and maximal biting in the intercuspal position (maximal dental clenching). In the first situation, the experimenter guide the volunteer in keeping his jaw in the rest position, and measurement of the EMG signal is begin after signal stabilization. For the chewing tests, the volunteer is requested to perform movements at a frequency of 1Hz to standardize the masticatory cycle time interval. For maximal dental clenching the volunteer is requested to maintain maximal isometric contraction of jaw elevator muscles during the recording time. To perform chewing and maximal clenching, Parafilm® material is placed between the pre molar teeth and the first and second upper and lower molar teeth. This material must be folded in five equal parts and redoubled in its total length, according to Biasotto23 who reported that Parafilm® reduced the variability of EMG signal values and could be considered the best material to record EMG activity during chewing. The time considered for EMG signal recording during the rest period and maximal isometric contraction is 5 seconds, and for chewing test it is 10 seconds. EMG signal recordings are stored in a computer for later analysis and processing. Signal AnalysesIn the first instance, EMG signal analyses are qualitative with the inspection of the raw signal (Fig.1). In the last decades, the application of mathematical models and statistical analyses has offered a better understanding of EMG signal properties, allowing the evaluation of the physiologic events of muscles. Such advances have made it possible to study muscle electrical manifestations in amplitude domain as well as wave frequency. In all the situations studied, the EMG signal is analyzed in time domain by the root mean square (RMS) application (in microvolts), which is an electronic average representing the square root of the average of the squares of the current or voltage during the entire cycle. This experimental protocol is used successfully in the majority of studies performed in EMG Laboratory at the University of Campinas - Piracicaba Dental School to evaluate TMD patients. Acknowledgement Special acknowledgements to the Brazilian Society of Electromyography and Kinesiology - SOBEC. References
Copyright 2004 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os04029f1.jpg] |
| |||||||||

{kind=link}