 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
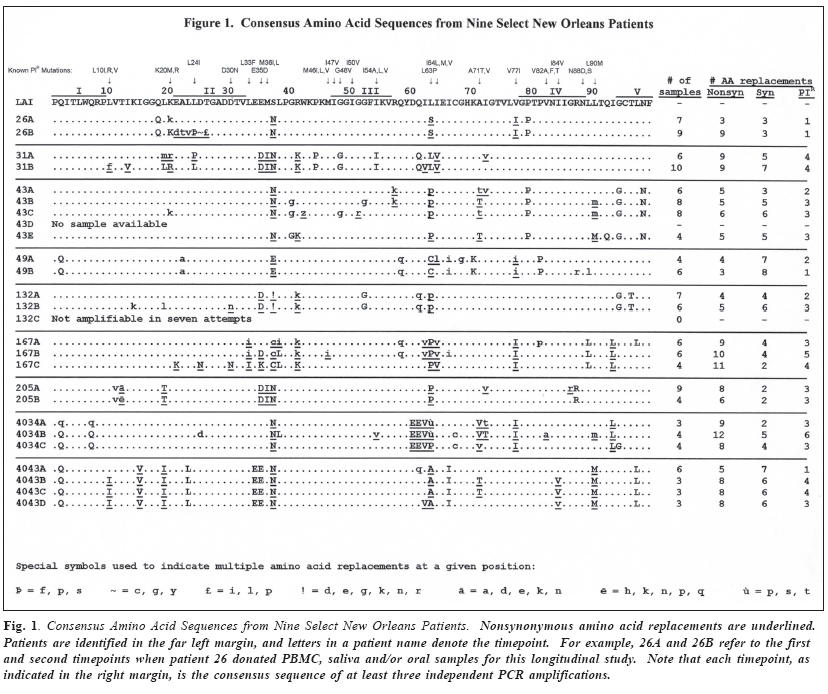
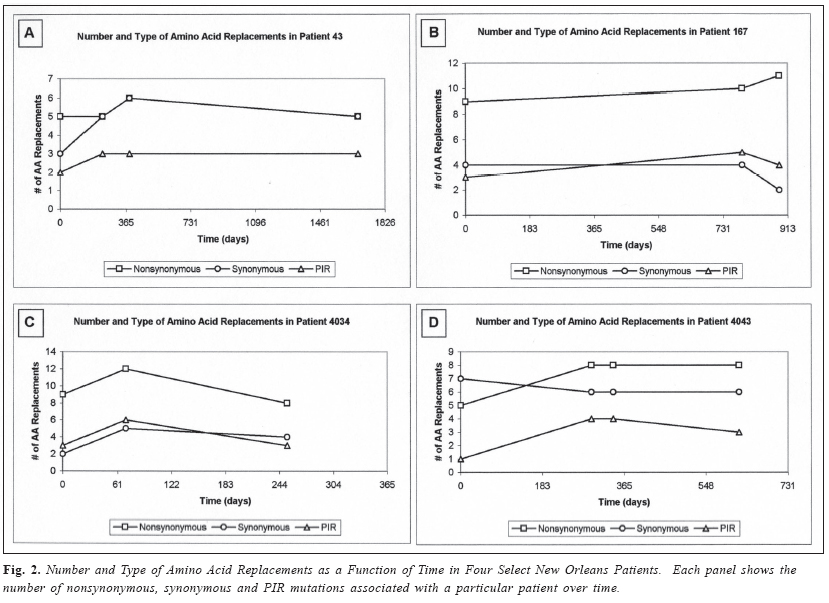
Brazilian Journal of Oral Sciences, Vol. 3, No. 11, October-December 2004, pp. 615-618 Longitudinal study of HIV protease mutations in oral tissues of selected patients Peter J. Hickman1 Janet E. Leigh1,2 Paul L. Fidel. Jr.1 Ronald B. Luftig1 1Department of Microbiology, Immunology and Parasitology, Louisiana State University Health Sciences Center, New Orleans, LA , USA Correspondence to: Ronald B. Luftig Louisiana State University Health Sciences Center 1901 Perdido Street New Orleans, LA 70112-1393 Phone: (504)568-4063 Fax: (504)568-2918 E-mail: rlufti@lsuhsc.edu Received for publication: July 08, 2004 Accepted: September 08, 2004 Code Number: os04033 Abstract Twenty-nine HIV-1 infected patients from New Orleans were enrolled as a cohort for this study over a four and one half year period. HIV-1 protease gene (pro) sequences were amplified using DNA isolated from oral tissues (gingival cuff, buccal mucosa, tongue, palate) as well as saliva and peripheral blood mononuclear cells (PBMC). PCR products were directly sequenced using a combination of manual and automated methods, and nucleotide sequences were translated using the universal genetic code. Protein sequences obtained from independent amplifications of a particular patient at a given time were consolidated into a single consensus sequence and compared to HIV-1LAI to determine amino acid replacements. The major findings were: 1) each patient had a signature sequence that probably represented the predominant HIV–1 quasispecies; 2) over periods of 19 to 1673 days mutation patterns remained relatively stable within a given patient; and 3) although nearly 40% of the initial nonsynonymous replacements in the protease signature sequences were mutations known to impart resistance to protease inhibitors (PI), over time patients did not accumulate additional PIR mutations. Key Words: HIV-1, protease gene, mutations Introduction This is a longitudinal study of a small cohort of HIV-1 infected individuals who were patients at the Dental-HOP (HIV Outpatient Clinic) in New Orleans, Louisiana, from 12/ 11/96 to 5/12/03. The protease gene (pro) is one of the most highly conserved genes in HIV-1, and it has been used along with the reverse transcriptase (RT) gene to monitor HIV-1 mutation rates in several longitudinal studies1. Our earlier research focused on mutations in pro that correlated with oropharyngeal candidiasis (OPC) and other oral diseases2-4. The poor fidelity of HIV-1 RT tends to lead to frequent mutations in many genes5. Our goal was to focus on protease mutation patterns over time in HIV-1 DNA that had been isolated from various oral tissues (gingival cuff, buccal mucosa, tongue, palate), saliva or peripheral blood mononuclear cells (PBMC). We observed previously that every patient had a unique HIV-1 protease mutation pattern2-3, and in this study we observed that each patient’s characteristic HIV-1 protease mutation pattern was relatively stable for periods of time up to 4.6 years. Material and Methods Isolation of template DNA, amplification, and purification and sequencing of PCR products. New Orleans patients were enrolled in this study only after informed consent, and procedures were performed in strict adherence to the guidelines of the Institutional Review Board of the Louisiana State University Health Sciences Center. There were 29 patients who donated amplifiable samples on at least two occasions over a 1,673 day (4.6 year) period, and four of the 29 patients provided samples on three or more occasions. Genomic DNA or cDNA was isolated from PBMC, unstimulated saliva or oral biopsy of gingival cuff, buccal mucosa, tongue or palate tissues as described previously2. Among patients with OPC, swabs of the same tissue type were generally collected from both lesion and nonlesion sites. DNA samples were amplified using nested primers specific for the HIV-1 protease as described previously2. PCR products of the predicted size were gel purified from extraneous bands and excess primers using the QIAquick Gel Extraction Kit (Qiagen, Valencia, CA, USA) according to manufacturer’s instructions, and PCR products were directly sequenced using the Thermo Sequenase Radiolabeled Terminator Cycle Sequencing Kit (USB Corporation, Cleveland, OH, USA) as described previously2 or were sequenced using an ABI 100 Model 377 Automated Sequencer. Data Analysis. All nucleotide sequences were translated into amino acid sequences using the universal genetic code and conventional single-letter abbreviations for amino acids. A capital letter indicates that the only species present in the given PCR product is different from the HIV-1LAI reference strain at that position, whereas a small letter indicates a mixture of mutant protease and HIV-1LAI-like protease at the DNA level6-7. When microheterogeneity was observed two or three times within a single codon, we assumed that all mutations were occurring simultaneously. Amino acid substitutions were identified as structurally/functionally conservative, nonconservative or radical replacements according to the system of Gallaher et al.8. ResultsThe pattern of mutations that were consistently observed within a specific timepoint of a given patient regardless of cell type from which the DNA originated (PBMC, saliva, lesion or non-lesion sites of oral tissues) is referred to as a consensus sequence2-3. The consensus sequences from select patients at various timepoints are shown in Figure 1. Of the twenty-nine patients in this study, the nine patients shown in Figure 1 were chosen because: 1) they provided samples a minimum of three times; or 2) they donated samples at two independent times and they demonstrated tissue or site specificity. Note that consensus sequences, by definition, obscure any minor variations within a patient timepoint due to tissue or site specificity.The number of nonsynonymous and synonymous amino acid replacements for a given consensus sequence are reported in Figure 1 as is the number of mutations implicated in resistance to protease inhibitors (PIR mutations)9. In Figure 2 the quantified amino acid replacements are plotted as a function of time, and the only patients shown are those that provided samples a minimum of three times. DiscussionWe and others have published data suggesting that HIV infection occurs with difficulty in the oral cavity due to a large number of inhibitors such as secretory leukocyte protease inhibitor (SLPI) and lysozyme10-12. The small amount of virus that is occasionally seen under highly sensitive assay conditions may be defective leading to few progeny virus particles, or perhaps functional virus particles are persistently released via a proviral genome form but rapidly killed. The latter explanation for low detectable viral loads is consistent with the hypothesis that once infection is established HIV-1 DNA is incorporated into quiescent T cells13. In this cohort of patients HIV-1 DNA could have been incorporated into T cells located in the buccal mucosa or other oral tissues. Since HIV has a high error rate due to poor fidelity of the reverse transcriptase and host RNA polymerase II5, one would expect to see mutations accumulate over time in the HIV-1 DNA isolated from a particular donor patient. In this study we chose to monitor pro, which is among the most highly conserved genes of HIV-1, and found surprisingly few changes in HIV-1 DNA isolated from a given patient over time. In patient 43, for example, there was a net gain of only one nonsynonymous mutation in the consensus sequence after 385 days (1.1 years) but no net gain after 1673 days (4.6 years). These data suggest that selective pressures are present in different reservoirs that stabilize the HIV-1 genome once a major quasispecies is established14. AcknowledgmentsThis work was supported in part by NIH grant DE-12178 awarded to Dr. Paul L. Fidel Jr. and Louisiana State University Health Sciences Center institutional fund. We wish to thank Mary Martin and Duncan Friedman for their technical assistance as participants in the Short research Experiences in Cancer (grant NCI CA47877) in the lab of Dr. Ronald B. Luftig. References
© Copyright 2004 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os04033f1.jpg] [os04033f2.jpg] |
| |||||||||

{kind=link}
{kind=link}