 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
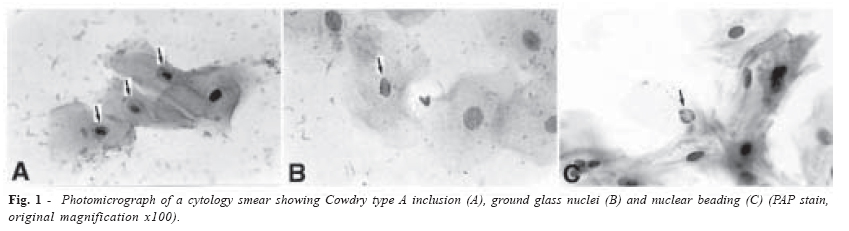
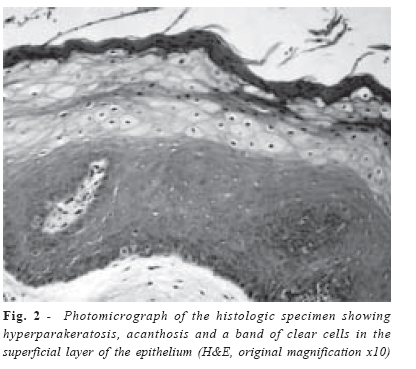
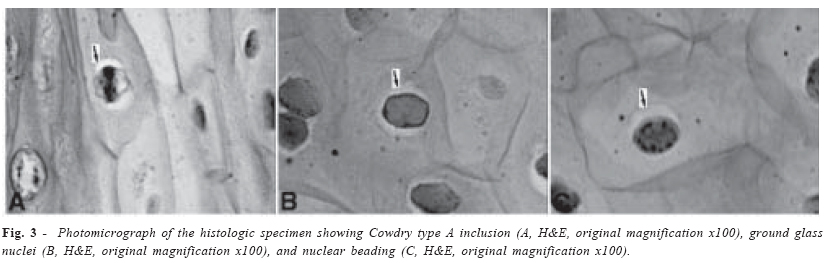
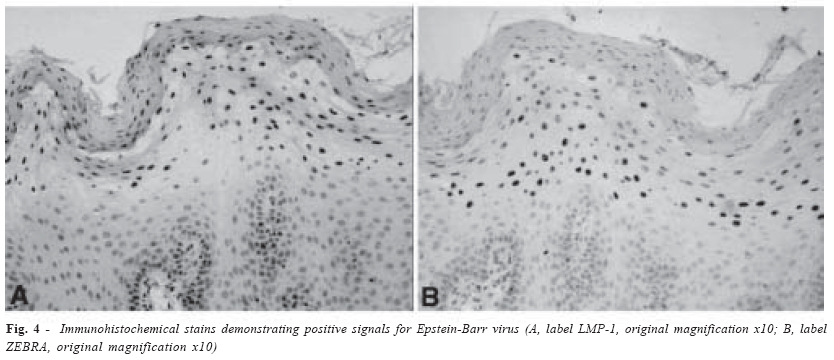
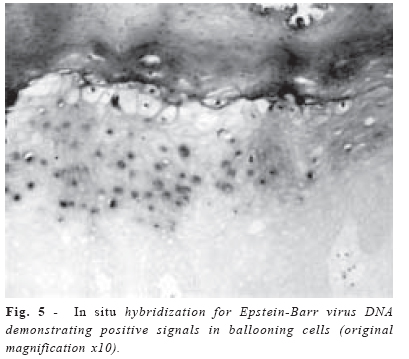
Brazilian Journal of Oral Sciences, Vol. 3, No. 11, October-December 2004, pp. 628-632 Oral hairy leukoplakia as a sign of HIV infection Arley Silva Junior1 Nikolaos Georgios Nikitakis2,5 Valli Meeks2 Claudia Cecilia Bossa Gracia3 Fernanda Maria Garcia Carvalho Saraiva3 Sonia Maria Soares Ferreira1 Eliane Pedra Dias4 Timothy Francis Meiller2,5 1 Fogarty Fellows from Institute of HumanVirology and University of Maryland,Baltimore, Department of Diagnostic Sciencesand Pathology, Rio de Janeiro University,Department of Oral Diagnosis and Pathology,Gama Filho University" Correspondence to: Arley Silva Junior University of Maryland, Dental School Department of Diagnostic Sciences and Pathology 666 West Baltimore St, Room 3D65 Baltimore, Maryland 21201-1586 Phone: 410-706-7628 FAX: 410-706-0519 E-mail: asj001@dental.umaryland.edu Received for publication: August 16, 2004 Accepted: September 30, 2004 Code Number: os04036 Abstract Described for the first time in 1984, oral hairy leukoplakia (OHL) is strongly associated with human immunodeficiency virus (HIV) disease, although some cases have been reported in HIV negative individuals. After the introduction of highly active antiretroviral therapy, the prevalence of OHL in HIV patients declined significantly. OHL has been convincingly shown to be related to Epstein-Barr virus. Cytopathologic examination is considered the best method for OHL diagnosis. This report describes a case of OHL in an HIV patient, whose HIV status was unknown at the time of OHL diagnosis. Key Words:oral hairy leukoplakia, Epstein-Barr virus, cytopathology Introduction Oral hairy leukoplakia (OHL) is a viral infection caused by Epstein-Barr virus (EBV), which is a double-strand DNA virus belonging to the human herpesvirus group1-5. The lesion is strongly related to human immunodeficiency virus (HIV) disease and was first described by Greenspan et al in 1984 as an oral manifestation in male homosexual HIV-positive patients1,6,7. The most common site of OHL is the lateral border of the tongue1,7-9. Clinically, it presents as an asymptomatic nonremovable white patch1,9,10. The histopathologic features are hyperparakeratosis, acanthosis, and ballooning degeneration of keratinocytes of the upper stratum spinosum; subepithelial inflammation is not commonly seen but, if present, it is usually mild and related to candidiasis infection1,10-13. Cytopathology is the method of choice for OHL diagnosis and is based on the identification of characteristic nuclear changes, including Cowdry A inclusions, ground glass nuclei and, in particular, nuclear beading2,7,14,15. Some researchers suggest that identification of the EBV by immunohistochemistry or in situ hybridization is required to confirm diagnosis of OHL1,4,9,11,12,16. Accurate diagnosis is important because it may be an early indicator of an undiagnosed HIV infection. Moreover, a diagnosis of OHL may be of prognostic value1,5,11,12,14. Herein the authors describe a case of OHL in an HIV patient, whose HIV status was unknown at the time of OHL diagnosis. Case ReportA twenty-six years old caucasian male was referred to the Stomathology Clinic of Universidade Gama Filho in May 2001 with a chief complaint of a “white patch in the mouth”. His past medical history was unremarkable except for an ear infection two months prior to his visit, which was treated with antibiotics for twenty days. The patient denied tobacco, alcohol, or illicit drug use. Extra-oral examination was unremarkable except for the presence of bilateral fissures at commissures. On intra-oral examination, yellowish-white pseudomembranous patches were observed on the hard and soft palate, oropharynx, dorsum of tongue, and on buccal mucosa bilaterally. A presumptive diagnosis of angular cheilitis and pseudomembranous candidiasis was considered. Systemic antifungal therapy was initiated, consisted of Ketoconazole 200 mg tablet once a day for 10 days. Patient returned to the clinic one week later for follow-up examination. During that time, the bilateral commissural fissures and intraoral pseudomembranous lesions were resolved; however, bilateral non-removable white patches were still observed on the lateral borders of the tongue. Clinical differential diagnosis for the persistent lesions included frictional hyperkeratosis and OHL. Two cytology smears were done on each of the lateral borders of the tongue and an incisional biopsy was performed on the left side of the tongue. A complete blood count (CBC) was also ordered. The specimens were sent to the Serviço de Anatomia Patológica do Hospital Universitário Antônio Pedro / Departamento de Patologia da Universidade Federal Fluminense. Cytopathologic examination revealed nuclear changes consistent with OHL, such as Cowdry A inclusion, ground glass nuclei and nuclear beading (Figure 1). Histopathologic examination also revealed changes consistent with OHL, including hyperparakeratosis, acanthosis, a band of clear cells in the superficial layer of the epithelium (Figure 2), and characteristic nuclear changes (Figure 3). Immunohistochemical analysis for EBV-related antigens LMP-1 and ZEBRA was subsequently performed. Both antibodies showed positivity in the superficial layers of the epithelium (Figure 4). Moreover, in situ hybridization for EBV was done and a positive reaction was identified in the superficial layers of the epithelium (Figure 5). Complete blood count revealed 0.4 x 103/UL lymphocytes (normal range 0.7 to 4.5 x 103/UL). In light of these results, the patient was referred for an HIV investigation. Elisa and Western Blot tests were positive for HIV. A complete medical work up was initiated and antiretroviral therapy was started. Dental care and management of oral lesions has been undertaken at the General Dental Clinic and Stomathology Clinic of Universidade Gama Filho. DiscussionSnijders et al.17 in 1990 proposed EBV as the etiologic agent of OHL. Before the advent of highly active antiretroviral therapy (HAART), OHL was a frequently observed oral manifestation of HIV disease, with a prevalence of 5% to45.1% in HIV positive patients; in patients with advanced disease or AIDS stage, the prevalence could be as high as 80%18-20. After HAART, a significant decline in the prevalence of OHL has been observed and the current prevalence is estimated to be between 2.8% to 26.6%3,21,22. The lesion is not commonly seen in HIV positive children, among which prevalence ranges from 1.96% to 2.0%23,24. OHL has been also reported in heart, kidney, liver and bone marrow transplant recipients; in patients with ulcerative colitis or Behçet’s syndrome; and in patients taking antibiotics or corticosteroid medications25-28. A few cases have been reported in immunocompetent individuals25. Most cases of OHL occur on the lateral border of the tongue and this predilection seems to be linked to the presence of receptors for EBV at this site1,8,9. Clinical presentation is that of an asymptomatic white, non-removable patch of variable size with a smooth, corrugated or “hairy” surface1,8,9,13. Differential diagnosis for OHL includes hyperplastic candidiasis, lichen planus, white sponge nevus, frictional hyperkeratosis, geographic tongue, keratotic reaction associated with electrochemical interaction, squamous cell carcinoma, or any other white non-removable lesion in the mouth1,10,13. The case of OHL that we presented affected a patient with signs of immunosuppression exhibiting oral candidiasis and decreased lymphocyte count. Identification of OHL prompted appropriate investigation, which established the diagnosis of HIV. Indeed, OHL may be an early sign of HIV infection in individuals whose HIV status is unknown, despite frequent presence of risk factors for HIV disease12,14. Moreover, the relationship between OHL and the depletion of the immune system in HIV positive patients is well documented and accepted, suggesting a potential prognostic significance of OHL.1,10 Nonetheless, Sabine Jahn et al.29 in 1998 proposed that it is difficult to regard OHL as a prognostic factor in HIV infection without considering HAART, because the new antiretroviral medications, including Protease Inhibitors (PI), have changed the natural progression and prognosis of HIV infection. The diagnosis of OHL is based on patient’s history, clinical features, cytopathology, histopathology, immunohistochemistry, in situ hybridization, polymerase chain reaction (PCR), and electron microscopy1,14,15. Fraga-Fernadez et al.14 in 1990 described for the first time the histopathologic criteria for OHL diagnosis. In this report, the authors called attention to three distinct nuclear changes described as Cowdry A inclusions, ground glass nuclei and nuclear beading, as the main features for OHL diagnosis. Subsequently, Fraga-Fernandez and Vicandi-Plaza15 (1992), Migliorati et al.7 (1993), Epstein et al.11 (1995) and Dias et al.2 (2000) reported that conventional cytopathology can be used as a method for the diagnosis of OHL based on nuclear changes, mainly nuclear beading. Treatment for OHL is not necessary, although some reports suggest the use of different modalities such as podophyllin 30%, retin A, or antiviral therapy, e.g. acyclovir and zidovudine (AZT). Recurrence is often noted with discontinuation of therapy1,9,30. We concluded that it is very important for the clinician to be aware of the more common oral manifestations associated with HIV infection. OHL is related to immunosuppression and its presence in the absence of a known cause of immunosupression should suggest HIV infection. Early identification of OHL and subsequent diagnosis of HIV are of particular importance because they allow initiation of treatment and control of the disease. Cytopathology for detection of characteristic nuclear changes, mainly nuclear beading, is a noninvasive, safe, inexpensive, easy to perform, and foremost reliable approach for the diagnosis of OHL. AcknowledgmentThanks for the support from the John E. Fogarty International Center AIDS International Training Research Program (AITRP). References
© Copyright 2004 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os04036f4.jpg] [os04036f1.jpg] [os04036f3.jpg] [os04036f5.jpg] [os04036f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}