 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
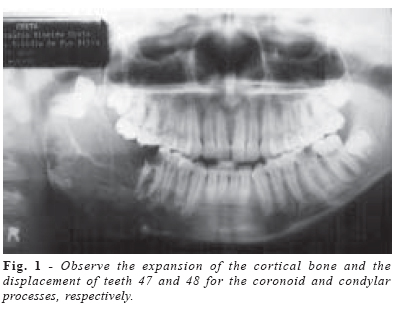
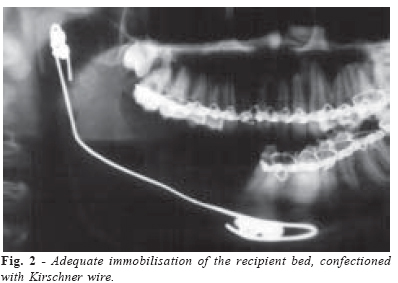
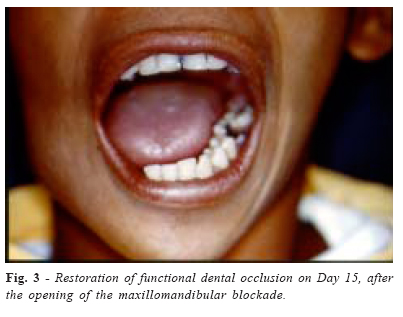
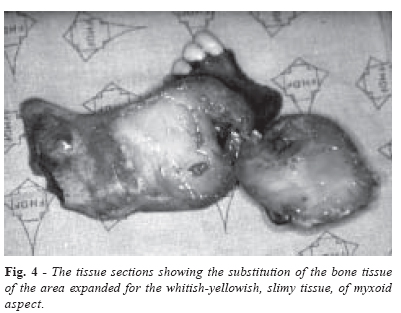
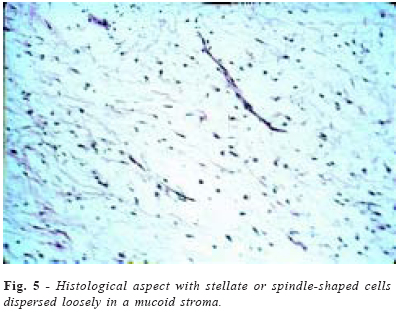
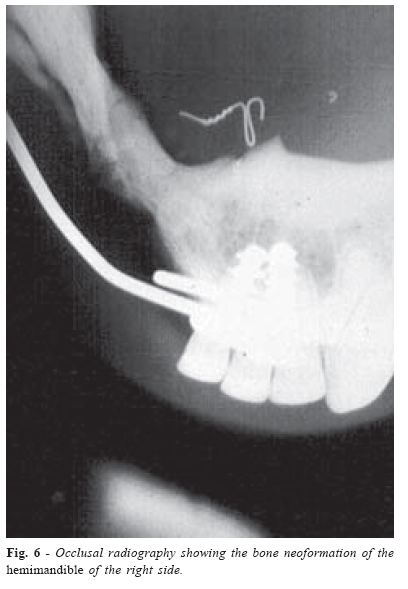
Brazilian Journal of Oral Sciences, Vol. 3, No. 11, October-December 2004, pp. 639-643 Odontogenic myxoma in an adolescentpatient – report of a clinical case Elvidio de Paula e Silva1*Everton Luis Santos da Rosa2*Moema PinheiroVeloso3*Luiz Cezar de Moraes4**Julio Cezar de Melo Castilho5**Patricia Pasquali Dotto6**1Residence in Oral and Maxillofacial Surgery (UERJ), Responsible for the Oral Maxillofacial Surgery Unit 2Master Degree Holder in Oral and Maxillofacial Surgery (PUC-RS) and a Staff of the Oral and Maxillofacial Surgery Unit 3Staff of the Pathological Anatomy Unit 4Titular Professor in Oral Radiology 5DDS Professor in Oral Radiology 6Graduate student in Oral Radiology Correspondence to: Luiz Cesar de Moraes Avenida Engenheiro Francisco José Longo, 777 São José dos Campos – São Paulo – Brazil – CEP: 12245-000 Phone: (55 12) 3947-9054 – Fax: (55 12) 3947-9010 E-mail: moraes@fosjc.unesp.br Received for publication: April 13, 2004 Accepted: July 08, 2004 Code Number: os04038 Abstract This paper presents a case of odontogenic myxoma affecting a black boy, 16 years old. In his case, the body and ascending ramus of his mandible, on his right cheek, had been affected by the tumour. The treatment applied was the partial resection of the mandible, in a way that its condyle was preserved. Two years later, the neoformation of the bone in the area of the resected mandible was observed clinically and radiographically. Key Words: odontogenic tumors, myxoma, mandible, radiography dental. Introduction Odontogenic myxomas are rare, benign tumors that affect the maxillofacial skeleton. These present a slow growth and are most of the time asymptomatic, recurring and locally destructive. They can cause paresthesia and dislocation of the anatomic structures at more advanced stages. In a study carried out at the Oral Pathological Service Unit of Western Ontario University, Canada, Daley et al.1 reviewed a total of 40,000 biopsies from their archives. 445 (1.11%) of these biopsies were mandible tumors, 24 cases (5.10%) of which were histologically compatible with odontogenic myxoma. Odontogenic myxoma normally affects people in their second and third decades of life. It is not common among the youth below the age of 16 . Kesler et al2. reported 10 cases of odontogenic myxomas, involving individuals below that age. Among the 80 cases of odontogenic myxomas diagnosed at their service unit, 10 (12.5%) had affected patients whose ages were between 5 and 16. Rennie et al.3 reported a case involving the mandible of a five-year-old child. Ries Centeno et al.4 described an operation case involving the maxilla of an eight-year-old boy. Nowadays, there is still a controversy over the true origin of this tumor. In a histochemical study, using cell surface markers (Vimentin, Actin and S-100 protein), in fresh samples, Moshiri et al.5 claimed that these tumors originate from the mesemchymal portion of the dental germ, specifically from the dental papilla. Odontogenic myxoma attacks the maxilla and mandible equally6. Clinically, it could be asymptomatic, causing pain and paresthesia at more advanced stages. Many times, they lead to the expansion of the cortical bone, causing facial deformation. This results in malocclusion and displacement of the teeth. In a radiographic evaluation, one can observe some unilocular or multilocular images, sometimes causing the expansion of the corticals, which are poorly defined with thin trabeculae of different lengths, centrally crossing the lesion. These images are frequently described as “tennis rackets”, “honey comb”, or “bubbles”. Histologically, this tumor is composed of relatively acellular, loose myxomatous connective tissues. Fibroblasts and myofibroblasts benign with variable quantities of collagen are found in a mucopolysaccharide matrix. Patches of trabeculae of woven bone and capillaries are found dispersed by the lesion. Odontogenic residues rarely appear in these tumors6. The treatment of odontogenic myxomas includes: enucleation and curettage, peripheral resection with a margin of 1 to 1.5 mm maintaining a strip of cortical bone, and large resection with a margin of 1 to 1.5 cm. The more aggressive the surgical act used is, the less chances the recurrence of the tumor7. The rate of recurrence in the interventions of little aggressiveness is about 25%3-4,6,8-9. Case ReportThe patient, G.R.S, 16 years-old, presented to the Oral and Maxillofacial Surgery Clinic of the “Hospital de Base” of the Federal District. He complained of swollen face, which had been with him for six months and had presented no type of symptomatology. During the clinical examination, the relevant facial deformation was observed with the expansion of the mandibular body on the right side. There were no signs of inflammation nor hyperthemia, and the patient had not used any type of medication. Upon palpation, a solid mass in the mandibular body could be felt. The lymphnodes of the submandibular region of the right side had increased and were painful. In the examination of the oral cavity, the cortical expansion of the lingual and vestibular surfaces of the mandible were observed, as well as, the absence of first and second right mandibular molars. The mucous membrane that covered the injury presented inflammatory signs and a fenestration on the surface. In the radiographic study, radiolucent images with poorly demarcated limits were observed, involving the mandibular body and ramus. Inside it was crossed by thin bone trabeculae. Second and third right mandibular molars were displaced for the coronoid and condylar processes (Figure 1). The radiographic limits in the mandibular symphysis level appeared quite diffused, making it considerably difficult to locate the actual limits of the previous lesion. An incisional biopsy was carried out under local anaesthesia of the area, and a histological examination was solicited, in which the odontogenic myxoma was confirmed. The surgery proposed was a mandible partial resection, with a submandibular access, whereby, preserving the mandibular condyle and osteotomy in the symphysis region between central and lateral right mandibular incisives, after confirming the probable previous limit of the injury through periapical roentgenograms. The right mandible was removed along with the affected ganglion and oral mucous membrane. An adequate immobilisation of the recipient bed, confectioned with Kirschner wire, was screwed into the remnants of the mandible condyle and the mandibular symphysis, using 4 stainless steel screws (Figure 2). The surgical wounds were closed and the maxillomandibular blocked, using vestibular bars which remained for six weeks. The patient was discharged from hospital on Day 5 postoperative for follow up. Four weeks postoperative and control radiographs were solicited, which showed the formation of the radiopaque tissue in the site. Next, the radionuclide bone scan was performed, and it confirmed the formation of the bone tissue throughout the extension of the right body mandible that was removed. After the opening of the maxillomandibular blockade, the patient was oriented on a liquid and pasty diet. There were improvements in the restoration of the functional dental occlusion and excursive movements of the conserved mandible (Figure 3). After twelve weeks of follow up, the patient was able to chew harder food items. According to the histological study, the material consisted of a segment of the right mandible, measuring 11.0 x 6.0 x 4.0 cm, showing vestibular and lingual bone expansion, with a thinning of the mandibular body and ramus. The presence of lateral incisive, canine and first and second right mandibular premolars areas of mucous membrane exposure was observed, featuring a soft and white tissue, in the molar region, measuring 2.0 x 1.5 cm. In the tissue section, the bone tissue of the whole-expanded area had been substituted for a white, soft, slimy tissue of myxoid aspect. The presence of two nonerupted teeth second and third right mandibular molars (Figure 4) was observed. The histological diagnosis presented an odontogenic myxoma (Figure 5). Twenty-four months after the surgical act, a complete neoformation of the right mandible was observed clinically and radiographically, making any other type of reconstruction unnecessary (Figure 6). Discussion All the authors claim that odontogenic myxoma is a rare tumor which exclusively affects the maxillofacial region2,5,10. It is a separate clinical entity11, originating in the mesenchymal, portion of the dental tissues11, and the dental papilla is usually pointed out as its probable origin5. It is a lesion with benign characteristics. It has an aggressive behaviour and a slow growth. It does not cause metastasis, but has a very destructive capacity2,7,12. Many times the patients look for treatment when the tumor has reached considerable proportions, causing the compression of important nervous and anatomical structures or when compromising the facial aesthetics. Despite the fact that most world reports claim that odontogenic myxomas affect individuals in the second and third decades of life13-14, there are several studies which show that this tumor also affects children at very young ages2-4. Based on their analyses, Kesler et al.2 say that this tumor has greater incidence in childhood, than other types of more aggressive tumors. Anamnesis and detailed clinical exams should be done, as a means of diagnosis for these tumors. The biopsies are always indicated, in order to confirm certain clinical suspicions and also differentiate this lesion from other similar pathologies, as in the cases of ameloblastoma, fibrous dysplasia, central granuloma of giant cells12, central hemangioma, calcifying epithelial odontogenic tumor, ossifying fibroma and idiopathic histiocytosis6. Besides the conventional radiographs, computerized tomographies can be used, as auxiliary means, especially on lesions affecting the mandible, in order to establish the limits of the expansion of the tumor12. Magnetic resonance imaging is not widely used, but it could help in differentiating inflammatory processes involving the maxillary sinus of a tumor12. When this tumor is diagnosed in an initial phase, the surgery is quite conservative. This does not always happen, though, due to the gradual and asymptomatic growth of these lesions. Tumors with large extensions usually demand invasive and radical surgeries, such as: maxilla or mandible partial resections, which lead to large mutilations in the patient as in our agree12. The authors agree, as they claim that in surgeries with little aggressiveness, the rate of recurrence is high3-4,6,8-9,12,15. Reconstructions in extensive surgeries are complex. The autogenous grafts are always the first choice, but they require a donor site, a difference between the donor and recipient areas, and the inconvenience of a surgical intervention. The meshes and plates of reconstruction are indicated in the mandible surgeries, but they are expensive and not available in all the public hospitals. References
© Copyright 2004 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os04038f6.jpg] [os04038f5.jpg] [os04038f3.jpg] [os04038f4.jpg] [os04038f2.jpg] [os04038f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}