 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 4, No. 12, Jan./Mar. 2005, pp. 646-650 Evaluation of quality of life and painin Temporomandibular Disorders(TMD) Anamaria Siriani de Oliveira1 1PT, Ph.D, Professor from Biomechanics,
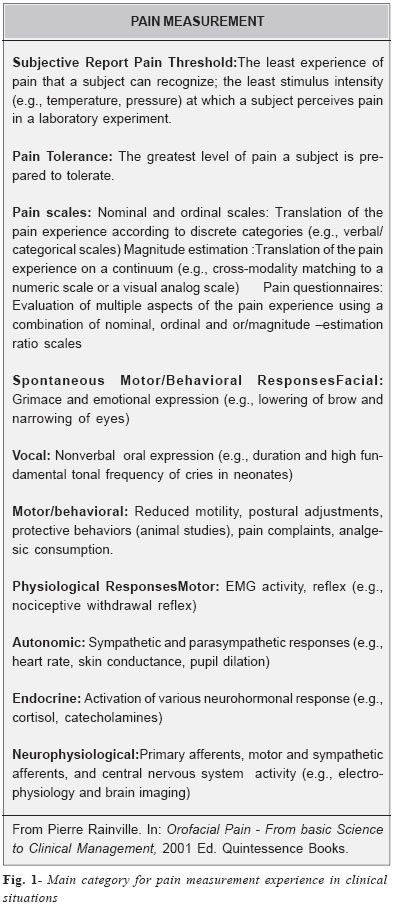
Medicine and Rehabilitation of Locomotor Apparatus, Ribeirão Preto School of Medicine, University of São Paulo –USP Received for publication: October 13, 2003 Code Number: os05002 Abstract Pain and quality of life assessment must have a multidimensional approach. This paper presents studies about the impacts that pain due to temporomandibular disorders can have in the patients’ life. Key Words: pain, quality of life, mcgill pain questionnaire, temporomandibular disorder. Introduction “An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”1 In order to understand pain complaints, especially in patients with chronic pain, it is essential to consider not only the physical and chemical components involved in a noxious activity, but also subjective and psychological aspects. Pain is always a subjective perception which results from the combination of different factors and its intensity rarely corresponds to the severity of the clinical pathology2-3. Other authors consider that pain complaint varies according to sex, occupation, culture, ethnic groups, mood, and motivation4-5. Therefore, the different aspects of pain complaint should be considered when choosing a pain assessment tool: the tool must be highly validated, reliable, and easy to administrate; it must allow the comparison between the magnitudes of change in pain features; and be relatively free of elements that could influence or bias the outcome. In addition, it must be useful to assess both experimentally produced pain and that observed during clinical practice, besides allowing the comparison between the physiological measurements obtained in humans. It is important to say that a complete pain assessment requires subject cooperation and an accurate observation of verbal and physiological signs of the patients’ experience with pain. The inclusion of affective-emotional aspects in the definition of pain, adopted by the International Association for the Study of Pain (IASP), requires the understanding and the use of a multidimensional assessment tool, in which the different aspects of pain complaint are evaluated by nominal, ordinal, and/or pain magnitude scales. In addition, such tool must have cognitive, behavioral, and psychosocial descriptors. Functional activities, quality of life, and drug use are aspects that may be included to assess the impact of pain in patients’quality of life as well as their social relations (Figure 1). Musculoskeletal conditions related to cervical regions, as well as masticatory musculature, are the main cause of nondental pain in the orofacial region and longitudinal studies have shown that the progression of pain severity is rare6. Nevertheless, the assessment of pathologies characterized by pain of the temporomandibular joint, face, masticatory and craniocervical muscles, and, consequently, in TMD and/ or in craniofacial or masticatory muscles is still controversial. According to the IASP classification (1994)7, the used term is “pain and TMD syndrome”, described as a condition characterized by pain in masticatory muscles, with severe pain, occasionally brief during mastication, frequently associated with restricted movements of the mandible and joint sounds. This variety of findings and the complex determination of TMD etiology make the assessment of pain, a symptom frequently referred by these patients, the object of different measurement trials. A numeric scale was used to estimate pain intensity in patients with TMD relating the three factors: arthrogenous features of TMD; myogenous features of TMD; and pain complaint, with the evolution of TMD in response to a conservative treatment8. Three groups were formed: patients with exclusively myogenous TMD (n=15), exclusively arthrogenous TMD (n=9), and mixed TMD (n=1). Patients with myogenous TMD showed the highest pain levels. However, these levels decrease very quickly in these patients. After the conservative treatment, a significant decrease in pain intensity was seen for patients with myogenous TMD during a period of one to two weeks after the beginning of treatment and these levels remained low during the followup period. Pain chronicity has also been reported as a factor that should be considered in the etiology and maintenance of TMD symptomatology. Sipila et al.9 evaluated the association of TMD symptoms and depression in 5.696 patients by means of the Symptom Checklist Depression Subscale (SCL-25 DS). Results showed that, for both women and men, depression was related to TMD pain chronicity during rest and movement. However, for women, the strongest relation occurred between depression indexes, pain, and the difficulty to open their mouths. Although there are reasons to believe that TMD and other conditions of facial pain may cause different kinds of impact in patients’quality of life, only few studies have documented the use of specific questionnaires or multidimensional tools to assess patients’pain. Both the sensitivity of quality of life indicators and the impact of the disease on TMD patients’life were assessed in a sample of 30 TMD patients10. Patients were recruited from dental clinics and received a questionnaire within a period of one to six months after their first visit to the clinic. The questionnaire concerned social demographic characteristics, symptoms, perception of pain, and functional capacity. Social indicators of TMD, pain, and anxiety showed to be more sensitive to oscillations of clinical conditions, demonstrating significant changes during the dental treatment. However, no differences were seen in terms of oral function, such as clicking and chewing ability. Such findings suggest that the social dysfunction associated with TMD is probably caused by the reoccurrence of unsolved oral function problems. Authors suggest that further studies are needed in order to investigate how social and psychological conditions could be related to the exacerbation of TMD pain episodes. Reisine et al.11 studied the usefulness of validated and standardized indicators, such as the McGill Pain Questionnaire (MPQ), to measure the impact of dental conditions to the quality of life of 152 patients. Patients were divided into four groups: 48 patients with TMD, 33 with periodontal diseases, 23 being prosthesis users, and 48 who had returned to seek the specialist. The first three patient groups reported different levels of impact to their quality of life, being that the impact was particularly severe to those with TMD. The indicators used proved to be sensitive in the distinction of different patient groups and also showed to be promising in epidemiological studies as well as for following the patients’quality of life. A Brazilian version of the McGill questionnaire (Br-MPQ), containing specific additional questions, was used to study the impact of pain in the quality of life of a group of 22 TMD patients12. The group was composed by 20 women and 2 men diagnosed with TMD, aged from 17 to 55 years-old (28±11years), all from the region of Araraquara, who had refered for physical therapy treatment. Results were analyzed using the distribution of data frequency into 7 categories:
Murray et al.13 assessed 121 TMD patients in their first visit to a unit specialized in craniofacial pain research, through the Oral Health Impact Profile, to measure these patients' quality of life. Outcomes showed a significant impact in patients' quality of life, and that the more common results presented strong psychological components. When compared to the population without pain complaints, the reports of functional problems, such as difficulty to chew specific kinds of food, were four times higher for these patients and depression reports were nine times higher. The relevance of psychosocial aspects in the etiology, pathology, maintenance, and aggravation of TMD has been discussed in the literature. In a clinical research carried out in Brazil, the psychodynamic and social aspects of 38 TMD patients were assessed by means of clinical interviews, a psychosocial questionnaire, and complementation phrase testing14. Patients had higher level education (91,4%), more than half of the them were married (57,1%), average family income was equivalent to 13 minimum (Brazilian) wages, they affirmed being unpleased with their jobs (71,4%), and showed anxiety, emotional tension, depression, aggressiveness, and others. MPQ is currently the most acknowledged validated multidimensional method used to study and assess the aspects of pain. The Brazilian version18 consists of 20 sets of qualitative and quantitative verbal descriptors designed to measure sensory, affective, evaluative, and miscellaneous dimensions of pain. In addition, as multidimensional assessment, it can supply data concerning the location of pain in human body diagrams and about pain intensity by means of an ordinal-word anchor scale. The questionnaire also provides a set of information about pain impact in quality of life involving the aspects of social relations and measurement types and quantities used for the eventual pain control. Mongini et al.15 employed the MPQ in its original version with the purpose to evaluate its discriminative ability in TMD (n=53) and facial pain (n=43). Results showed that the scores for 11 subclasses and PRI were higher in the group with facial pain. Descriptors chosen by patients were different between the groups, confirming a consistent discriminative capacity of findings concerning TMD and facial pain patients. Campbell et al.16 used MPQ, State-Trait Anxiety Inventory, Beck Depression Inventory, and the Pennbaker Inventory of Limbic Languidness to assess pain reports, psychological stress, and depressive symptoms of 114 TMD patients, with a history of physical or sexual abuse. A group of TMD patients (without a history of abuse) was also included in the research. Pain scores, anxiety, and depressive symptoms were more significant for patients with a history of physical abuse. Nevertheless, results haven’t shown differences between groups regarding other domains. MPQ and Visual Analog Scale were simultaneously administered to 57 patients with arthrogenous TMD and 28 patients with myogenous TMD in order to assess these patients’pain reports17. The authors reported that the higher score in the affective category for myogenous TMD patients could be explained by the influence of the anxiety component, and concluded that MPQ can be considered as an important tool to discriminate myogenous and arthrogenous TMD. Literal translations of the MPQ’s original version may lead to adaptation problems due to historical and social language derivation, whereas qualitative pain assessment is performed using a cluster of word named descriptors. Castro18, for instance, mentioned that the term “agonizing” (English Language) wouldn’t have such an intense meaning as its cognate in Portuguese Language (agonizante). In order to obtain a consistent Brazilian version of MPQ, which wouldn’t be exactly the same as the original version, Castro18 translated the MPQ’s original version to Brazilian Portuguese Language –Br-MPQ. Oliveira et al.19 studied TMD patients from the region of Araraquara with the purpose of evaluating and discriminating pain complaint by administrating Br-MPQ; patients were classified by symptom severity using an anamnesis index. This study’s sample consisted of 23 patients, two men and 21 women, aging from 17 to 55 years-old, who had been refering for a physical therapy clinic in the city of Araraquara. Patients received a detailed explanation about how to appropriately answer the questions. Of the whole sample, 8 patients were classified as moderate TMD and 15 as severe TMD. For severe TMD patients, the temporomandibular joint region was reported as being the most painful, while moderate TMD patients mentioned the cervical region as being most painful. Concerning masticatory muscles, both groups reported the temporal as the most painful. Regarding the temporal pattern of pain, 50% of moderate TMD patients described their pain as rhythmic, periodic, and intermittent. Severe TMD patients reported their pain as being continuous, stable, and constant. Present pain intensity (PPI) analysis showed that severe TMD patients reported lower levels of pain intensity than moderate TMD patients. The mean range score of pain (pondered PRI) were higher for the miscellaneous dimensions of pain in both groups. Therefore, the Brazilian version of MPQ has proved to be a useful tool, able to distinguish temporal pattern of pain, the location of higher pain complaint, and pain intensity for TMD patients classified by a diagnostic index. Nonetheless, affective perception, linked to memory and pain perception related to TMD were similar among the studied groups. References
The following images related to this document are available:Photo images[os05002f1.jpg] |
| |||||||||

{kind=link}