 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 4, No. 12, Jan./Mar. 2005, pp. 659-663 Periodontal disease in a rural community in Minas Gerais, Brazil Débora Pallos Jussara Cia Sanches Loberto José Roberto
Cortelli Sheila Cavalca Cortelli Daniela Martins de Souza Lucilene Hernandes
Ricardo.
University of Taubaté, Department of Periodontology – UNITAU – Taubaté,
SP Brazil Received for publication: February 9, 2004 Code Number: os05004
Abstract The aim of this study was to evaluate the prevalence and severity of periodontal disease and treatment needs in a Brazilian rural community, using the Community Periodontal Index of Treatment Needs (CPITN). This study included 183 individuals who were clinically evaluated. The results showed that 45% of the individuals between ages 0-5 years had bleeding upon probing, and 34% of individuals ages 6-12 presented dental calculus. Among the individuals ages 13-18, 15% of pathological pockets were found with probing depth (PD) of 4-5 mm. However, among individuals ages 19-34, 50% showed a PD of 4-5 mm and 12.5% PD ≥ 6 mm. In the group of individuals ages 35-44, 17% showed PD ≥ 6 mm. Ninety percent of the individuals up to 13 years old needed only oral hygiene instructions. Dental scaling was indicated to 70% and 95% of the individuals aged 13-18 and 19-34 respectively. A more complex periodontal therapy was indicated to 17% of individuals aged 35-44. These results showed the necessity of the implementation of dental preventive programs to this community, especially to individuals under 12 years, and curative programs for individuals ages older than 13 years old. Key Words: periodontal status, CPITN, probing depth, epidemiological survey Introduction
Periodontal disease is usually chronic in nature and has a high prevalence in the entire world. The pathogenesis of this disease leads to the destruction of the periodontium and it may eventually result in tooth loss. This common disease is found in localized or generalized forms of involvement. In addition, its destruction pattern can be classified as incipient, moderate or severe. Among the various factors that influence prevalence and severity of periodontal disease, socio-economic status and availability of local community health care resources are very important. Previous studies have shown that low socio-economic status and geographic location can influence the prevalence of missing teeth among partially dentate individuals in Nicaragua, Australia and Chile1-3. Both the prevalence and the severity of periodontal disease can be studied in a given population by the use of an index which identifies specific periodontal clinical parameters. The Community Periodontal Index of Treatment Needs (CPITN) was developed jointly by FDI and WHO4 in order to facilitate the assessment of periodontal status and determine treatment needs in large epidemiological surveys. This index provides data not only on the periodontal health of a community, but also can be used as a fundamental tool for planning and monitoring periodontal treatment needs of specific populations. The main advantages of this index are its simplicity of use and its widespread application for periodontal epidemiological studies all over the world. The aim of this study were to describe the prevalence and the severity of periodontal disease, as well as treatment needs of a small rural community located in the Southeast of Brazil. Material and Methods
This study, approved by the University of Taubaté, São Paulo – Human Subject Ethics Council, was conducted in the rural village of Campo Redondo, city of Itamonte, state of Minas Gerais, Brazil. All individuals included in the present study signed the study informed consent form. The total population of this village is comprised of 323 white individuals. One hundred and eighty-three subjects ages 2- to 84-years (19.84 ± 13.59) participated in this study. Dentate subjects were examined by one of two periodontally trained and calibrated examiners. The examination procedures for the Community Periodontal Index Treatment Needs (CPITN), as recommended by the WHO4, were followed. Special 0.5 mm ball-ended probes with color markers at 3.5 and 5.5mm were used for these measurements. A score of 0 (periodontal
health – code H), 1 (gingival bleeding – code B), 2 (calculus at any supra- or sub-gingival site – code C), 3 (pocket of 4-5mm – code P1), or 4 (pocket of 6 mm or more –code
P2) was obtained for each dentate sextant, or an X (excluded)
was recorded for edentulous or otherwise excluded sextant The examiners’periodontal training and calibration were initiated before data collection. In addition, a continuous calibration was performed during data collection in 10% of the subjects. Inter-examiner reliability was tested by means of the weighted Kappa statistics6. The weighted Kappa statistics for the CPITN scores ranged from 0.75 to 0.85. Results
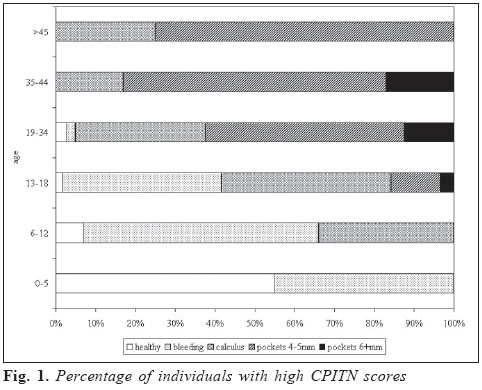
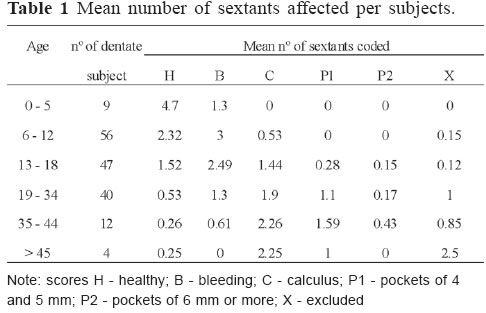
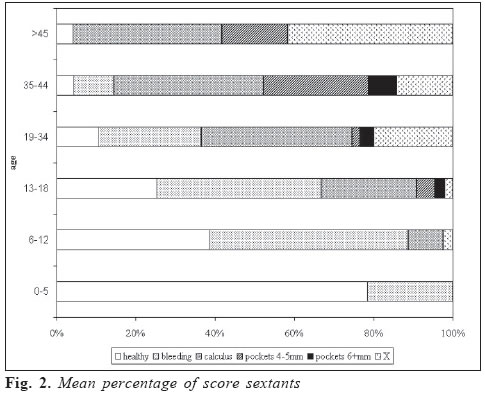
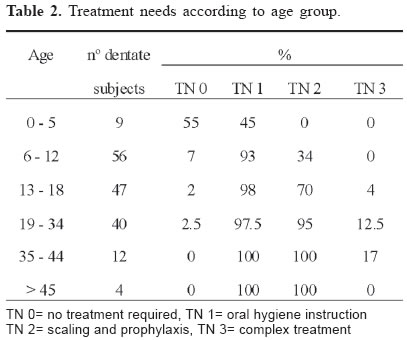
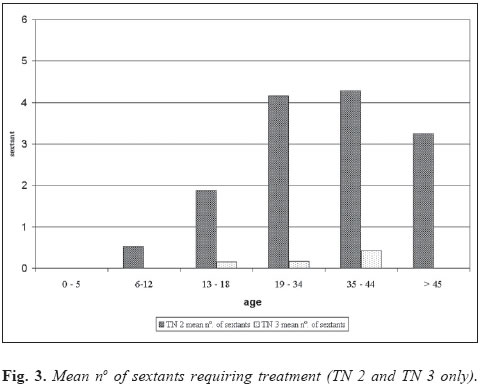
This report is comprised of data originated from 168 subjects of the initial 183 volunteers that accepted to be part of this study. Two of the individuals were excluded because they had less than two teeth in each sextant. A total of thirteen individuals were completely edentulous and therefore excluded from this analysis. The prevalence rate of periodontal disease as summarized by CPITN is shown in Figure 1 for all age groups as the percentage distribution of dentate subjects according to the highest score recorded. Only a small percentage of the subjects was scored as periodontally healthy. A relatively high percentage of subjects, 10-75% between age groups, had 4-5 mm pockets, although this varied widely (Figure 1). Pockets over 6 mm in depth were identified in only a few subjects. The most common and highest CPITN scores in the age groups 6-12 and 13-18 years old were bleeding on probing and calculus deposits. For the age groups 19-34, 35-44 and > 45-year-old, the most prevalent score was periodontal pockets with 4-5 mm. The severity of periodontal disease observed in this population is shown in Table 1 and Figure 2. The sextant status shows that the mean number of healthy sextants decreased with age. Furthermore, the mean number of code X increased with age. For the age groups 19-34, 35-44 and > 45 year-old, calculus deposits were evident in 32-38% of the sextants. In the 6-12 and 13-18 age groups, approximately 50% of the sextants were bleeding on probing. In addition, pockets with > 6 mm in depth affected only 0-0.5% of the sextants. According to the treatment needs, 55% of subjects of group 0-5 years were periodontally healthy and 45% needed only oral hygiene instructions. Almost all individuals (90 to100%) > 6 year-old needed oral hygiene instructions. Seventy per cent of the 13-18 age group needed scaling. This treatment need was also indicated to 95 per cent of the 19-34 age group. None of the subjects older than 35-years scored as periodontally healthy. The prevalence of treatment needs as scaling and prophylaxis (SC) and oral hygiene instruction (OHI) was 100 per cent for groups 35-44 and > 45 years. Deep pockets affected 17 per cent in the 35-44 age group. This same age group showed the need for complex treatment (Table 2). Only a very small number of sextants required treatment TN 3. Deep pockets affected less than 0.5 sextants in the age groups 13-18, 19-34 and 35-44. Individuals above 19 years old demonstrated need for TN 2 treatment in many sextants, and the mean number of sextants was between 3.25 to 4.25 (Figure 3). Discussion
In a recent review paper on the prevalence of periodontal diseases in Central and South America, it was stated that only a few representative epidemiological studies are available in Latin America7. The current study offers additional data on the periodontal status of a small rural community of underserved Brazilians. It is of importance to report that this rural community does not have fluoridated water and is isolated by a 40 km unpaved road to a larger town where dentists are located. Due to the low socioeconomic status of this community, its dental care needs are commonly treated by dental extractions. The CPITN has been developed to facilitate the work to express the prevalence and severity of the periodontal destruction and treatment needs in large populations. This index does not intend to report the level of periodontal disease8-10. When the objective is to determine or to follow periodontal status or treatment needs of populations, the most cost-effective method would be to examine the 10 index teeth and to record only deep periodontal pockets11, although at the moment of the treatment all periodontal measurements should be recorded. The population group comprised of individuals up to 18 years old had clearly lesser signs of periodontal disease, when compared to individuals older than 19 years (Figure 1). These results are in accordance with Smith and Lang1 who have observed an increase in the prevalence of pockets ≥ 6 mm in older individuals. Mumghamba et al.12 have also found a high prevalence of periodontal disease when comparing older age groups in a rural area of Ukonga, Tanzania. In the study by Norderyd and Hugoson13 of a Swedish adult population, age was also associated with the presence of severe periodontal disease. The older age group (50-70 years) was found to have the strongest correlation with severe periodontal destruction. Nevertheless, it is still unclear if aging per se is a risk factor for severity of periodontal disease, or if its effect is due to the prolonged exposure of older subjects to known periodontal etiologic factors. Moreover, the same authors could not find any correlation with the socio-economic status and the severity of periodontal disease. In the current study, unfortunately, the population > 45 years did not allow this continuous observation due to the fact that most of the individuals were already fully edentulous, possibly due to their very low socio-economic status. However, Gamonal et al.2 have observed that individuals who have a high socio-economic status show lower prevalence of periodontal disease and lower severity when compared to individuals who have middle or low socioeconomic status. These same authors have also shown that the mean number of missing teeth in the lower socioeconomic status group was higher than in the other two groups. Brennan et al.14 have observed in their study that the age factor has an influence in the prevalence of missing teeth in dentate individuals in Australia, and the prevalence of edentulism was higher in older individuals. According to Kawamura et al.15 the percentage of subjects having healthy gingiva by an oral rating index in adults was similar to some studies that used the CPITN index. The results of the current study have shown a mean of 0.25 healthy sextants in the age group 35-44, while Mengel et al.16 have observed 1.5 healthy sextants in the same age group in the Yemen upland, and Mumghamba et al.12 have found 2.5 in their study. It was expected to find an overall poor oral hygiene condition in this Brazilian rural population because of their inherent difficulties to both preventive and curative dental care access. Bourgeois et al.17 have reported improved periodontal health in adults living in urban versus rural areas. Baelum et al.10 have found in a rural area of Kenya only 0.26% periodontally healthy subjects. However, Katz et al.18 have found 0.96% periodontally healthy subjects in the same age group in an Israeli military force population. The presence of calculus in younger age group (6-12 years old) was equivalent to one found by Marcoantonio Jr. and Santos19 in their study published in 1998, which showed the mean number of sextants to be 0.53. The current study was able to show that most individuals examined needed some level of periodontal care. Oral hygiene instruction and scaling and root planing were the most needed procedures based on the distribution of CPITN scores. Subjects requiring complex treatment, in this population, were older individuals. Smith and Lang1 have found that over 40% of the older group (34-60 years old) needed the complex treatment, while only 17% in the current group had the same need. However, in the current study, all individuals who were older than 45 happened to be fully edentulous. Dini20 was able to demonstrate in her study the beneficial effects of the implementation of a treatment program. She observed an increase in the mean number of healthy sextants and an overall decrease in the mean number of bleeding sextants. It is known that both a preventive program and the delivery of appropriate dental care are the most important steps towards changing this situation. In conclusion, the findings of the current study highlight the need of health promotion activities to improve oral hygiene practice by dental hygienists and curative procedures by general dentistry practices. Acknowledgments
The authors are grateful to Dr. Antonio José Moretti for the English corrections. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo -
Brazil
The following images related to this document are available:Photo images[os05004f2.jpg] [os05004f1.jpg] [os05004t1.jpg] [os05004t2.jpg] [os05004f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}