 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 4, No. 12, Jan./Mar. 2005, pp. 664-669
Morphological and proliferative analysis of the healing tissue in human alveolar sockets covered or not by an e-PTFE Membrane: A preliminary immunohistochemical and ultrastructural studyRenata Penteado 1 Giuseppe Alexandre Romito 2 Francisco Emílio Pustiglioni3 Márcia Martins Marques41PhD in Periodontics, Division of Periodontics,
School of Dentistry, University of São Paulo,
Brazil. Received for publication: November 3, 2003 Code Number: os05005 Abstract Healing tissues of extraction sockets have been used, as autografts, for the treatment of periodontal bony defects. These tissues have proved to be more effective in inducing bone formation than mature bone. However, there are limited data regarding the nature and proliferative activity of its cells. The aim of this pilot study was to analyze the nature and the proliferative activity of cells present in newly formed tissue from human extraction sockets, covered or not by an e-PTFE membrane. The healing tissue of 6 pairs from human alveolar sockets covered or not by an e-PTFE membrane, collected 4 weeks after tooth extraction was analyzed. The specimens were observed using light and transmission electron microscopy (TEM). The immunohistochemical characterization of the tissues included type I collagen, osteonectin and bone sialoprotein detection. The proliferation rates of the tissues were obtained using PCNA labeling. Cells and extracellular matrix were labeled for type I collagen, osteonectin and bone sialoprotein, in both groups. PCNA antibodies revealed significant higher proliferation rates in the coronal areas than in the apical areas of the tissues, independent of which group they belonged to. TEM showed cells containing a Golgi apparatus, rough endoplasmic reticulum and mitochondria indicative of secretory cells, in both groups. In the apical area of the test and control groups, the extracellular matrix exhibited more bundles of collagen fibrils than in the coronal area. The cells of healing tissue of dental sockets are osteoblastic in nature. Additionally, they present higher proliferating rates in the coronal areas, independent of the use of the e-PTFE membrane. Key Words: bone healing; guided bone regeneration; immunohistochemistry; transmission electron microscopy. Introduction
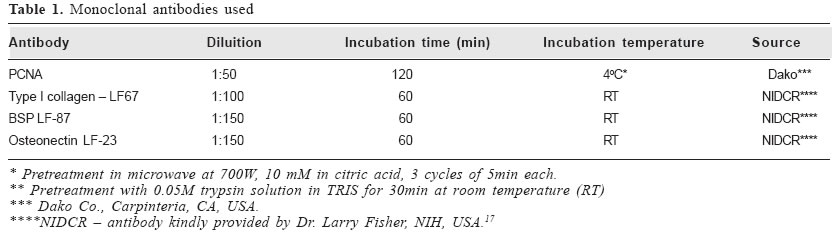
Highly differentiated tissues, such as bone tissue, present lower proliferation rates than nonosteogenic connective tissues1. Thus, the ingrowth of these less differentiated tissues into an osseous defect may disturb or totally prevent osteogenesis in the area2. To avoid this ingrowth, the guided bone regeneration technique, based on the placement of a mechanical barrier has been used2. It is known that, when one or several teeth are extracted, maintenance of the alveolar ridge is important for future implant placement, as well as for the placement of any type of prosthesis. The preservation of this ridge can be favored by using osseous regeneration techniques, at the moment of tooth extraction3-5. Therefore, a greater amount of bone in this alveolar socket would be expected when a mechanical barrier is placed on it and it is covered by the mucoperiosteal flap. Currently, the expanded polytetrafluorethylene (e-PTFE) membrane is the best-documented material for the purpose of promoting guided bone regeneration6. The healing tissue formed inside extraction sockets has been used, as an autograft, for the treatment of periodontal bony defects7-8. Fortunately, tooth extraction stimulates an extensive osteogenic activity in the alveolar socket8. In clinical trials, in humans, this immature osseous tissue, used as an autograft to treat periodontal infrabony defects, exhibited an encouraging osteogenic potential8. This tissue proved to be three to four-fold more effective in inducing bone formation than mature bone marrow9. The aim of this pilot study was to analyze the newly formed tissue, collected four weeks after tooth extraction, from human extraction sockets, covered or not by an e-PTFE membrane. We studied the nature and the proliferative activity of cells present in this tissue. Material and Methods Sample collection Six patients participated in this study (4 females and 2 males, mean age 50.5), and six pairs of sockets were obtained from them. During anamnesis, no systemic alterations were detected in these patients. Only no smoking patients were included. They had, at least, one pair of single-rooted teeth indicated for extraction for prosthetic reasons. Each tooth had half the root attachment in the socket showing neither periodontal disease nor mobility. Before surgery, patients received detailed information on the treatment about to be performed on them. Patients who agreed to participate in the study signed a previous informed consent document. This study was approved by the Ethics Committee of the School of Dentistry at the University of São Paulo. Pre and post-surgical medication was comprised of amoxicillin1 500mg10, every 8 hours, during 7 days. Immediately before surgery the patients used 0.12% chlorhexidine2 mouthrinses for 1 minute11 and, thereafter, twice a day, during 4 weeks after each surgical procedure12. After local anesthesia, internal beveled incisions were performed from the gingival crest to the alveolar bone crest, following the gingival margins of the teeth to be extracted, both buccally and palatally or lingually. The full-thickness flaps were elevated exposing the underlying bone and roots. The teeth were removed carefully in order to preserve the alveolar bone13. Dental sockets were thoroughly debrided§. Sockets of the test and control sides were chosen at random. The sockets of the test side were covered by an oval-shaped membrane||, trimmed to overlap the periphery of the alveolar crest by approximately 2mm14. The flaps were then displaced to completely cover the membrane15, and mattress sutures16 provided primary wound closure. In the control side the same procedures were performed, except for the placement of the membrane. The patients were followed on a weekly basis until the membrane was removed. The sutures were removed 14 days after the surgery. Four weeks after the extractions, all dental sockets were reopened. In the test side, the membrane was removed to allow for the manipulation of the tissue from the dental socket. In both the control and test sides, the tissue formed inside each dental socket was gently lifted out, as an entire plug, by means of a surgical curette ¶. The tissue removed from each dental socket was longitudinally sectioned (from bottom-apical to top-coronal), in two halves. One of the halves (6 pairs) was used for light microscopy analysis and the other (6 pairs) for transmission electron microscopy (TEM) analysis. After curettage, degradable membranes were placed over every socket# . These membranes were totally covered by full-thickness flaps, which were then sutured. Transmission Electron Microscopy All samples (6 pairs of healing tissue) were fixed in 2% glutaraldehyde in 0.1M sodium phosphate buffered solution, at pH 7.4, for 2 hours and post-fixed in 1% osmium tetroxide in the same buffer, for 45 minutes. After washing in distilled water, samples were stained “en bloc”with 0.5% uranyl acetate for 3 hours, rinsed and dehydrated in graded ethanol. After immersion in propylene oxide, samples were embedded in Epon** and polymerized for 72 hours at 60°C. Semithin sections (1 µm) were cut and stained with a mixture of 1% azure II, 2% methylene blue and 2% borax in distilled water. Ultrathin sections were stained with lead citrate and uranyl acetate and examined in a JEOL 1010 transmission electron microscope. Light microscopy For light microscopy, all specimens (6 pairs of healing tissue) were immediately fixed in 10% neutral formalin for 24 hours. Then, they were embedded in paraffin, sectioned at 5µm, and stained with hematoxylin and eosin (H&E). Immunohistochemistry Paraffin sections (3 µm) were used for streptavidin-biotin immunohistochemical assay. Immunolabeling was carried out at room temperature. The incubation times, source, concentration of antibodies and pretreatments used are listed in table 1. After incubation with primary antibodies, sections were washed and exposed to secondary antibodies†† (biotinylated anti-mouse). After further washing, sections were exposed to a strepto-avidinbiotin complex. Diaminobenzidine‡‡ was used as a chromogen. Sections were then counterstained with Mayer’s hematoxylin. Positive controls were bone trabeculae present in the periphery of the specimens. Cell Proliferation From each group and region (apical and coronal), 100 spindleshaped cells, chosen at random, were counted and the number of PCNA-labeled nuclei were recorded, yelding data on the cell proliferation rate. Results
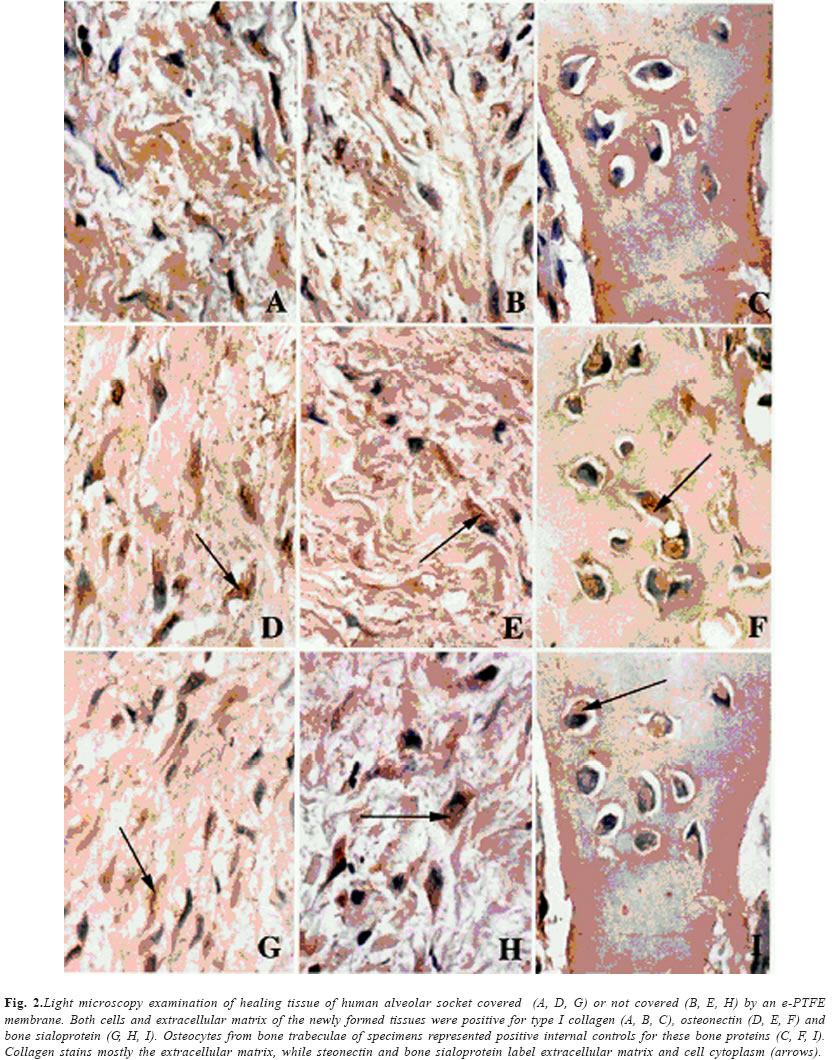
Transmission electron microscopy Under TEM, the healing tissues collected within human extraction sockets, 4 weeks after extraction, were similar in control and in test sockets (Fig. 1). The cell population consisted mostly of one type of cell that closely resembled a fibroblast. Almost all tissue cells were spindle-shaped with cell processes. The nucleus was indented with moderate margination of condensed heterochromatin. The cytoplasm was rich in intermediate filaments and had variable amounts of organelles. Cells presented a prominent Golgi apparatus, abundant rough endoplasmic reticulum. Banded collagen fibrils in the stroma were found in close contact with the cells. The only difference noted was between the extracellular matrix of the coronal (Fig. 1A) and apical areas (Fig. 1B). Therefore, the extracellular matrix exhibited more collagen fibrils in the apical area than in the coronal one. However, the thickness of collagen fibrils did not exhibit differences in different areas of the socket. Immunohistochemistry Most of the test and control specimens exhibited a macroscopic funnel aspect, whose apex corresponded to the apical region of the dental socket. Trabecular bone could be noted, in some specimens, outlining the newly formed tissue. Both tissues from the test and control sockets were represented by a connective tissue rich in cells, with collagen fibers interspersed and newly formed blood vessels. Some degree of inflammatory infiltrate was present in both groups, being more evident in the tissues of the control sockets. Both the cells and the extracellular matrix of the newly formed tissues were positive for type I collagen (Figs. 2 A, B, C), osteonectin (Figs. 2 D, E, F) and bone sialoprotein (Figs. 2 G, H, I). Labeling of test groups are shown in Figs. 2 A, D, G, and control groups in Figs. 2 B, E, H, osteocytes from bone trabeculae of specimens represented positive internal controls for these bone proteins (Figs. 2 C, F, I). There were no differences on labeling of the tissues for the studied proteins, neither in different regions of the healing tissue (apical and coronal), nor in different experimental groups (test and control). Cell proliferation The percentage of PCNA positive cells varied among teeth and patients. Additionally, in all specimens, the percentage of labeled cells in the coronal region was always higher than in the apical region. Discussion The cells of healing tissue of dental sockets 4 weeks after tooth extraction are osteoblastic in nature. The concomitant presence of both type I collagen, BSP and osteonectin in our specimens showed the commitment of these cells to form bone tissue. Additionally, independently of the use of the e-PTFE membrane, these cells present higher proliferating rates in the coronal areas of the socket tissues. We used membranes in order to prevent alveolar bone loss after extraction and to obtain, within it, a larger volume of tissue with osteogenic properties. We chose to place a membrane on the socket immediately after extraction to take advantage of the acute wound. In these wounds, bony walls present multiple exposed marrow spaces that favor communication of the vascular and cellular elements associated with bone growth16. For this reason, we elected for our study, the central portion of the healing tissue within the socket, which would be the last region to differentiate, since the healing of a socket occurs in a centripetal form17. There was no overall difference between the proliferation rates of tissues covered with an e-PTFE membrane when compared with controls. This was expected, since the membrane is inert and biocompatible6. However, the membrane offered mechanical protection to the tissues, leading to a smaller mononuclear inflammatory infiltrate in the coronal area of the test group when compared to the control group (not covered by the membrane). Our results showed significantly higher proliferation rates of cells in the coronal region than in the apical region, both in the test and in control groups. Tissue in the apical region is probably in a more advanced phase of the healing process, with cells being more differentiated and less proliferative than those in coronal region. This could be in consequence of the distance to sources of vessels and cells (base and lateral walls of the socket). In apical area the sources are closer than in the coronal area. The TEM results complemented the results of light microscopy. The larger concentration of collagen fibrils found in the extracellular matrix of the apical region of the healing tissue, in comparison to the coronal region, is an additional sign that the extracellular matrix protein synthesis is in a more advanced stage in the apical region than in the coronal region. According to Devlin and Sloan18, have shown that osteoprogenitor cells in the residual periodontal ligament and bone marrow may contribute to bone regeneration following tooth extraction, in agreement with our results. The identification of areas of higher cell proliferation rates can be of importance for electing the area of osteogenic tissue to be used in grafts. The graft is placed in areas of tissue loss, which must be reconstructed. A tissue with a higher cell proliferation index should fill the area to be reconstructed faster and more adequately than a tissue with a lower index of cell proliferation, supposing that this tissue maintains its proliferative and osteogenic capacity, when used as an alograft. In conclusion, data from the present pilot study suggest that the cells of healing tissue of dental sockets 4 weeks after tooth extraction are osteoblastic in nature. It thus corroborates other studies that indicate the use of this tissue as an autograft for the treatment of periodontal bony defects. Additionally, they present higher proliferating rates in the coronal area, independent of the use of the e-PTFE membrane. This indicates that the tissue at the apical region of the healing socket is in a more differentiated stage of the bone formation compared to that of the coronal region. Thus, this study suggest that the coronal areas of the healing socked tissue should be preferentially used as an autograft, because it is still in proliferation, the cells of this tissue are more suitable for filling in the bony defects, before the final bone differentiation phase is reached. Acknowledgements
We are indebted to Ms Elisa Santos, Ms Edna Toddai and Ms Patricia Galdino for their technical expertise and assistance. We also thank Dr. Cristiane França for helping with the photographic documenting. The study was supported by a grant from the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP). (Footnotes)
1 Amoxil- SmithKline Beecham, São Paulo,
Brazil. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os05005t1.jpg] [os05005f2.jpg] [os05005f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}