 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 4, No. 12, Jan./Mar. 2005, pp. 670-675
Odontogenic cysts - A descriptive clinicopathological studyLuís Monteiro 1 Jesus de la Peña 2 Liliana Fonseca 1 António Paiva 3 Barbas do Amaral 21 Instituto Superior de Ciências da Saúde
- Norte 2 Hospital Geral Santo António –Porto 3 South Manchester University Hospitals, U.K. Received for publication: August 10, 2004 Code Number: os05006 Abstract Odontogenic cysts are lesions that deserve every attention, mainly because of all complications they can cause. To study their characteristics, the authors did a retrospective clinicopathological analysis of 124 oral biopsies that were diagnosed as odontogenic cysts, in Hospital Geral de Santo António – Porto. Clinical variables such as age, sex, location, clinical diagnosis and histological diagnosis were studied. Inflammatory radicular cysts were the most commons (48.4%) followed by dentigerous cysts (21.0%), residual cysts (17.7%) and keratocysts (12.1%). The most frequent clinical manifestation was swelling (62.9%). Age appears to be related to the type of cyst, expressing the etiopathologic characteristics of each one. It is concluded that a definitive diagnosis is based on a triad of radiology, clinics and histology, which presupposes a tight cooperation between the clinician and the histopathologist. Key Words: oral pathology, developmental cysts, inflammatory cysts, jaw cysts, Gorlin syndrome. Introduction Cystic pathology owes a lot of its particular characteristics to the presence of teeth and its associated tissues. Its special nature tends to be related with the embryologic development of teeth and the dynamic interactions of epithelial elements with mesenquimatous elements. A cyst is a pathological fluid, semi-fluid or gaseous-filled cavity lined by epithelium that, in turn, is lined by a capsule of connective tissue. They deserve one’s attention, mainly because of all the complications they can originate, such as facial aesthetic changes, jaw fractures, infections, and occasional neoplasia of its epithelium1-4. Many classifications of jaw cysts have been proposed and used, according to different criteria such as its embryologic origin, aetiology, pathology, or its clinicalmorphological manifestations. The World Health Organization (WHO) more recently, classifies epithelial cysts (or true cysts), as odontogenic cysts and nonodontogenic cysts. The first type includes two categories: inflammatory and developmental. Non-odontogenic cysts are also developmental cysts and include nasopalatine and nasoalveolar cysts, amongst others. Cysts without epithelial lining, also called pseudo-cysts, are nowadays considered to be non-neoplasic bone lesions and include solitary bone cysts and aneurysmal bone cysts5. The purpose of this paper was to study the frequency of several types of odontogenic cysts and some of its clinical-pathological characteristics. Material and Methods
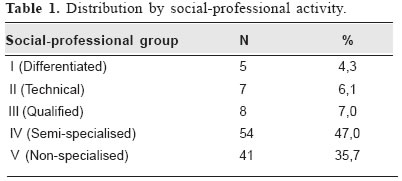
It was performed a descriptive study. All histopathological reports (n=153) of oral cavity lesions with histological diagnosis of odontogenic cyst were reviewed. These diagnoses were made by the Anatomic Pathology Service of the Hospital Geral de Santo António (Porto), in the course of a three-year period, between January 1999 and December 2001. In all cases, histological preparations were reviewed and clinical reports were analysed, along with the complementary means of diagnosis (plain radiographs, orthopantomograms and computer tomography). Twenty-nine cases were excluded due to lack of clinical information or non-concordance of data. Therefore, 124 patients with odontogenic cysts established the final sample. Variables such as, age, sex, occupation, location, clinical manifestations, radiographic appearance, clinical and histological diagnosis, were studied. Recurrences were analysed over a follow-up period of 1 to 3 years. Classification of these lesions was made according to the WHO (Kramer and Pindborg, 1992)5. Classification of the social-professional groups was based on the British Registrar-General6. The location of the cystic lesions was divided into maxillary or mandibular and anterior sector (incisors and canines) or posterior sector (premolars and molars). Statistical analysis included the chi-square test to analyse the categorical variables, and the t-student test and the Kruskal-Wallis test were used to analyse the continuous variables. For this purpose it was used the SPSS 10.0® specific computer program. The admitted level of significance was p<0.05. This study was approved by the Health Ethics Commission of Hospital Geral de Santo António –Porto. Results
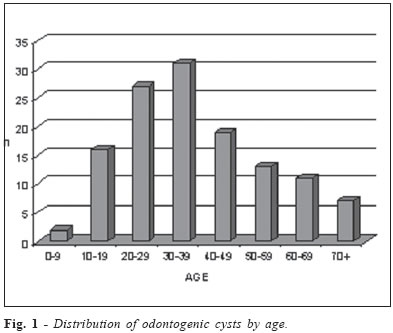
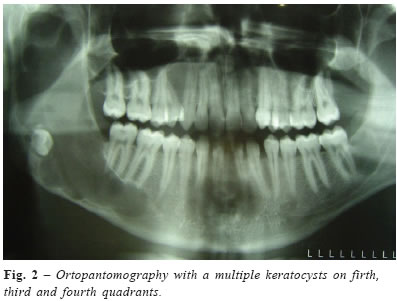
The studied sample included 124 patients, 72 of them were men (58.1%) and 52 were women (41.9%). The most frequent type of cysts was the radicular cyst with a total of 60 cases (48.4%), followed by 26 dentigerous cysts (21.0%), 22 residual cysts (17.7%), 15 keratocysts (12.1%), and 1 paradental cyst (0.8%). The age interval at diagnosis with the greatest number of cases (25.0%) was the one ranging from 30 to 39 years old. The median age was 34 years, the youngest being 7 years old and the eldest 79 years old. When age and cyst type were related, dentigerous cysts were more frequent on the second and third decade, radicular cysts were more frequent on the fourth decade, residual cysts were more frequent on the fourth, fifth and sixth decade and keratocysts were more frequent on the second and third decades of life. The median distribution of each type of cyst, displayed on table 2, shows a significant difference (p=0.002). (Figure 1) The most representative (47.0%) social-professional group on this sample was the semi-specialised group (table 1). About 10.5% of all patients (n=13) had more than one cyst, which makes a total of 144 cysts on the final sample. Thus, 89.5% had 1 cyst (n=111), 5.6% had 2 cysts (n=7), 2.4% had 3 cysts (n=3) and 2.4% had 4 cysts (n=3). As for the location of the cysts (n=144), 53.5% (n=77) of all cysts were on the maxilla and 46.5% (n=67) were on the mandible. In the maxilla, the most affected sector was the anterior (59.7%, n=43), whereas in the mandible, the most affected sector was the posterior (81.5%, n=53) (p<0.001). The most frequent location of inflammatory cysts (radicular and residual cysts) was the maxilla, and for developmental cysts (keratocysts and dentigerous cysts) was the mandible, mainly in the posterior sector (table 2). The most common clinical manifestation was swelling that was present in 62.9% of cases (n=78). Other symptoms, by decreasing order of appearance were spontaneous drainage of fluids in 21.0% of patients (n=26), infection (20.2%, n=25), pain (17.7%, n=22), caries (15.3%, n=19), face cellulitis (7.3% n=9), teeth mobility (2.4%, n=3), sinusitis (1.6%, n=2), trismus (1.6%, n=2), changes in alveolar healing (1.6%, n=2) and paresthesia (0.8%, n=1). In a large number of patients these complaints were associated. It is important to point out that in 36.4% of patients, cysts were discovered by accidental radiological finding (n=44). This situation was more evident for keratocysts and less evident for radicular cysts (p=0.019). Clinical diagnosis made before histological ones, had a positive histological confirmation in 82.9% of cases (n=92). Patients underwent cystectomy, 86.0% (n=107) of which were performed under general anaesthesia and 14.0% (n=17) with local anaesthesia. The cyst’s radiological image was unilocular (90.6%, n=116), followed by unilocular with lobulated margins (6.3%, n=8) and multilocular (3.1%, n=4). Cyst’s size was between 1 to 10 centimetres. Radicular cysts had a median size of 2 centimetres, thus smaller than dentigerous cysts and keratocysts (median = 3cm). This difference was significant (p=0.02). Clinical diagnosis made before histological ones, had a positive histological confirmation in 82.9% of cases (n=92). Patients underwent cystectomy, 86.0% (n=107) of which were performed under general anaesthesia and 14.0% (n=17) with local anaesthesia. Recurrence occurred in 4.4% of all cases. In patients with keratocysts, it were found 3 cases of Gorlin’s syndrome, in individuals with multiple keratocysts. They also showed the typical alterations of this syndrome such as several basal cell naevi, hydrocephaly, calcification of the falx cerebri, broad nasal root, hypertelorism, history of basal cell carcinoma, mild mental retardation and family history of jaw cysts and brain calcifications. Other variables connected to keratocysts and other odontogenic cysts are shown on table 2. About 47.8% (n=11) of all keratocysts were associated to impacted teeth (p<0.001). Histologically, about 86.7% of keratocysts were parakeratotic (n=13). It is important to mention that 18.2% (n=4) of keratocysts recurred, while other types of cysts rarely recur. The paradental cyst (n=1) occurred in a 30-year-old woman, located on the mandible in the posterior sector. It was an occasional radiological finding and the histological diagnosis confirmed the clinical diagnosis. (Figure 2 and 3) Discussion Inflammatory odontogenic cysts were 65.9% (n=83) of the total sample and 32.5% (n=41) were developmental odontogenic cysts. The most frequent inflammatory cysts were radicular (47.6%, n=60) followed by residual cysts. In the group of developmental odontogenic cysts, dentigerous cysts were the most common (20.6%, n=26). Many studies, support these results. Daley et al.7 in a study of 40000 oral biopsies made on the Diagnosis and Oral Pathology Service of the Western Ontario University (Canada), found a percentage of 64.9% for radicular cysts, 24.1% for dentigerous cysts and only 4.8% for keratocysts. On the other hand, Mosqueta-Taylor et al.8 analysed 856 cases of odontogenic cysts in Mexico and found a percentage of 21.5% for keratocysts. The frequency of keratocysts is, therefore, variable from study to study, maybe because of the different criteria used in the histological diagnosis, because of the lack of communication between physician and pathologists or because of the heterogeneity of the studied populations. Shear et al.9 mention a study of 2616 cysts diagnosed in the Department of Oral Pathology of the WitWatesrand University in South Africa, where a frequency of 52.3% for radicular cysts and 11.2% for keratocysts was found, which are very close to those obtained in this study. The studied sample showed a slightly higher frequency in men. Men were also more affected by the several types of jaw cysts, except for keratocysts. Most studies also show a higher frequency in men8,10-11. Unlike other studies8,12-13, in this study, the keratocysts slightly affected women more frequently than man. Taylor et al.8, in their sample, also found that women were more affected but only by radicular cysts, while men were more affected by keratocysts and dentigerous cysts. These results are thought to be more related to the type of populations studied than to the specific characteristics of these cysts. The present study revealed that this pathology might appear at any age. However, certain types of cysts seem to appear mostly at certain ages, which can be seen when analysing the median of ages. Dentigerous cysts were more frequent in young individuals, whereas radicular and residual cysts were commoner in adults and elder individuals. Such results, partially confirmed by other studies, express the etiopathogenic characteristics of each type of cyst 12. The most frequent location for inflammatory cysts (radicular and residual cysts) was the maxilla, whereas for developmental cysts (keratocysts and dentigerous cysts) was the mandible, mainly in the posterior sector. The most frequent radiological feature of these lesions was unilocular as the multilocular appearance was only seen in keratocysts, which seems to be a characteristic of such lesions. In a study of odontogenic keratocysts performed by Zhao et al.11 in the Wuhan University, in China, it was found that 16% of keratocysts were multilocular. It should be pointed out that the radiological feature unilocular lobulated and multilocular are distinct, although they can be confused in conventional radiology. That’s why CT scan images should be used in its classification, as it was done in this study. It was also keratocysts that had the highest recurrence rate (18.2%, n=4) after a follow up period of three years. Radiological features showed no relationship with recurrence. Their recurring nature is a typical characteristic for this type of cysts, mostly in the first 10 years after their first presentation4,10,12. In this study, it was found three Gorlin syndromes (in 20% of the cases with keratocysts) associated to multiple keratocysts of the parakeratotic type. Not all published papers present identical results. Oda et al.10, in a study made in the USA with 393 patients with keratocysts, found that 5% had Gorlin’s syndrome. Of the 87 cases reported by Kakarantza-Angelopoulou and Nicolatou14, in a study made in Athens, 8.8% had the syndrome. In a paper published by Cabral et al.12, in a sample with 238 epithelial maxillary cysts, no Gorlin’s syndromes were found. When the diagnosis of a keratocyst is made, especially if there are multiple recurrent lesions, it is essential to search for a possible Gorlin’s syndrome. If cysts are slow growing, expansive and usually symptomless lesions, it is understandable why, in this study, the most frequent clinical manifestation was swelling, which represents an advanced stage. It was also established that cysts frequently were accidental radiological findings. Thus, 36.0% (n=44) of cases in the total sample were radiological findings. That demonstrates the value of periodical x-ray examinations for the screening of such pathology. Keratocysts corresponded to the largest number of radiological findings (60.0%, n=9). They were the ones with the least clinical manifestations, but when they were present, the lesion was usually in an advanced stage. It should be mentioned that in some cases, other signs and symptoms were identified after the radiological finding. In several cases, the clinical diagnosis did not match the histological one, which demonstrates the importance of having a histopathological examination done. The clinical concordance was highest for dentigerous cysts, followed by radicular cysts, which means that these types of cysts have more obvious clinical-radiological features than other types of cysts such as keratocysts. The latter were the ones with the least clinical concordance in this sample, which shows that for the diagnosis of this type of cyst, the histological examination is extremely important. It’s thought that the presence of impacted teeth makes the clinical diagnosis easier for dentigerous cysts, but it can be an element of error for the assumption diagnosis of keratocysts. In fact, almost half of the keratocysts in this sample were associated to an impacted tooth, which may cause its mistake for a dentigerous cyst. That’s why, in such cases, histological examinations allows confirmation of dentigerous cysts or might diagnose the presence of keratocysts or even neoplasic lesions. In the same way, there were several cases where the histopathologist was only able to tell the type of cyst after receiving clinical and radiological information, which demonstrates its importance. It should be pointed out that it’s very important to send all surgically removed specimens for histological examination, in appropriate conditioning, along with all clinical and radiological information, thus allowing an adequate, complete and conclusive diagnosis. One might say that the definitive diagnosis is based on a triad composed by clinical observations, radiological features and histological examining, which requires an open dialogue and a close cooperation between the dentist/ surgeon and the histopathologist. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os05006f1.jpg] [os05006t2.jpg] [os05006f2.jpg] [os05006t1.jpg] [os05006f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}