 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
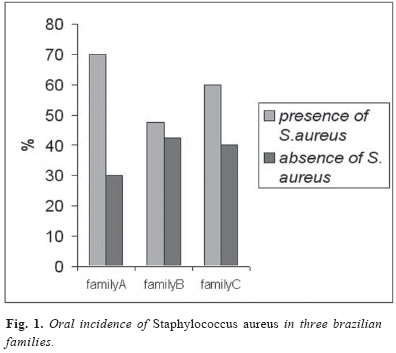
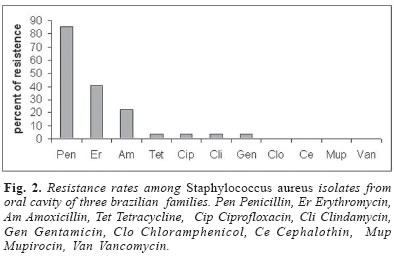
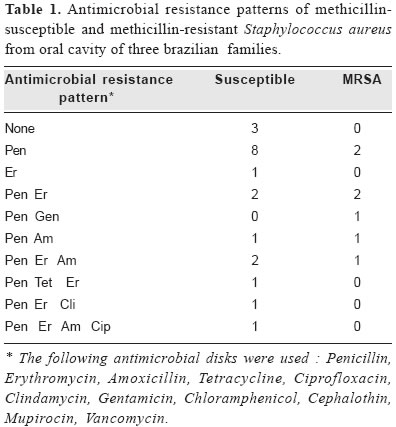
Brazilian Journal of Oral Sciences, Vol. 4, No. 12, Jan./Mar. 2005, pp. 676-679 Oral incidence of Staphylococcus aureus and antimicrobials agents resistance Vanessa Bueris 1 Fabiana Cristina Pimenta3 Izabel Yoko Ito 2 José Moacir Marin 11Ribeirão Preto Dental School, Universidade of São Paulo, Ribeirão Preto, SP, Brasil 2Ribeirão Preto Pharmacological Sciences School, Universidade of São Paulo, Ribeirão Preto, SP, Brasil 3Federal University of Goiás, GO, Brasil Received for publication: March 08, 2004 Code Number: os05007 Abstract Three health Brazilian families were examined for their oral carriage of Staphylococcus aureus the most common persistent human pathogen. The mean level of S.aureus colonization was high 56.2% and 25.9% of the individuals were methicillin-resistant S. aureus (MRSA) carriers. However, a low level of resistance to eight antimicrobial agents were found, except for penicillin (85.1%), erythromycin (40.7%) and amoxicillin (22.2%). Key Words: Staphylococcus aureus, oral incidence, MRSA, antimicrobial resistance. Introduction Staphylococcus aureus is a common human pathogen that causes various skin and mucosal infections. Besides superficial infections, the organism can also cause abscess formation, septicemia, pneumonia, osteomyelitis, and gastroenteritis1-2. Although the oral cavity harbors a complex microflora consisting of mostly non-pathogenic microorganisms, it was of interest to investigate the occurrence of S.aureus. There are several reports of the isolation of this bacterium from the oral region3-5 but no detailed characterization was done. Historicaly antibiotic-resistant strains of S.aureus were first identified in 1942, just after the begin of clinical treatments with penicillin6. In the late fifties, semi-synthetic penicillins, like methicillin, were developed to solve this problem, but only two years later, methicillin resistance was reported5. Over the last twenty years, methicillin-resistant S. aureus (MRSA) strains have emerged as important pathogens, affecting primarily hospitalized patients7. This problem seems to be moving beyond the hospital environment. Recent reports showed that the number of community-acquired MRSA, infections had increased8. The occurrence of MRSA in the nostril, skin wounds and respiratory tract has been well documented, but little is known about its presence in the oral cavity or the potential implications for the practice of dentistry6. Some reports have showed the persistence of S.aureus in the oral cavity, specially in children, suggesting that it can serve as a reservoir for MRSA with potential to spread and cause nosocomial infections4-5. In Brazil, methicillin is not used. Organisms referred to as MRSA are actually oxacillin resistant S. aureus (ORSA). However, as methicillin and oxacillin are similar antibiotics, MRSA is the usually accepted designation. This study report the persistence pattern to some antimicrobial agents of S. aureus strains isolated from the oral cavity of healthy people, as well as its incidence among families. Material and MethodsBacteria were isolated from the oral cavity of healthy individuals belonging to three families (A, B and C), from the region of Ribeirão Preto, SP, Brazil, with at least 3 generations (48 members). Whole unstimulated saliva samples (ca 2mL) were collected in sterilized tube containing glass beads, homogeneized for one minute (Mixtron-Toptronix, São Paulo, Brasil) and inoculated onto salt agar supplemented with 1% egg yolk. This was incubated at 37o C for 48 H. S. aureus was identified by macroscopic characteristics, lecithinase production and the tube coagulase test. All isolates were tested by standard disk diffusion, according to the NCCLS9 recommendations for susceptibility to the following antibiotics: penicillin (10U), erythromycin (15µg), Gentamicin (10µg), chloramphenicol (30µg), cephalothin (30µg), tetracycline (30µg), ciprofloxacin (5µg), clindamycin (2µg), amoxicillin (20µg), mupirocin (5µg) and vancomycin (30µg), (CEFAR, SP, Brazil). Methicillin-resistance was verified by the NCCLS oxacillin screening test10. The S.aureus isolates were inoculated with Steers replicator onto oxacillin screening agar plates (Mueller Hinton agar; NaCl 4%; 6µg/mL oxacillin) and after incubation at 35oC for 24 H, the strains that grew on this agar were considered methicillin-resistant. The penicillinase production test was done as reported before11. Penicillin-sensitive Micrococcus luteus (ATCC 9341) and a freshly prepared penicillin G solution was added, to cooled Mueller Hinton Medium (Difco, Detroit, MI, USA) to a final concentration of 105 –106 cfu/mL of the culture and 0.03 U penicillin per mL. The mixture was poured into Petri dishes (12.0 mL) and allowed to harden. S. aureus isolate to be tested was streaked loopfull in a form of ellipse. The plates were incubated at 37oC for 24 H. It was considered penicillinase-producer those strains that allowed the growth of Micrococcus luteus colonies surrounding the ellipse. Results and DiscussionWhile the importance of staphylococci as medical pathogens has been recognized for many years, the presence of Staphylococcus species as a component of the resident oral flora is controversial but, surprisingly, there have been relatively few detailed studies of the distribution of staphylococci in the mouth12. The families analyzed in this study showed a high incidence of oral colonization by S. aureus (Figure 1). The prevalence of S. aureus detected in each family was as follows: family A 70.0%, family B 47.8%, family C 60.0%. The incidence of S. aureus in this study was higher than those reported by Myake et al.4 33.0% and by Suzuki et al.5 43.0%. However a more recent study13 found that 64.0% of healthy children carried S. aureus in the oral cavity. Moreno et al.8 reported that the prevalence of S .aureus carriers at the community, that do not showed any risk factors (e.g hospitalization, contact with healthy workers, skin wounds, etc) is more common than expected. In their work 58.0% of the 170 S. aureus carriers have acquired the microorganism at the community and only 7.0% showed at least, one of those risk factors. The emergence of multiresistant microorganisms is an increasing problem that requeries continuous precautions to control the spread of these organisms in the community. The antimicrobial resistance pattern founded in the three families was showed in Figure 2. In general, the individuals considered in this work showed a low resistance level to the most commonly antimicrobials used in therapy. This result agree with Busato et al.14, that also observed a low antibiotic resistance level in S .aureus strains isolated from nostril. Only penicillin resistance rate was extremely high (85.1%), what was confirmed by the penicillinase production test (data not showed), erythromycin resistance and amoxicillin resistance were 40.7% and 22.2% respectively (Figure 2). All strains that were penicillin-resistant also were penicillinase producer. The production of penicillinase does not provide only penicillin resistance, but also to all b-lactam antibiotics15. However the resistance level found in this study was extremely different from those reported by Teixeira et al.16 and Oliveira et al.17 which found high resistance level for penicillin, erythromycin, gentamicin, chloramphenicol, tetracycline, trimethoprim-sulfamethoxazole, ciprofloxacin almost the same antibiotics tested in this study. We do not have an explanation for the discrepancy, but it might be due to the difference of sources, their isolates were epidemic strains of MRSA that caused infectious disease in a hospital, while ours were indigenous strains. Mupirocin interferes on protein synthesis and so is highly effective against MRSA strains. This antibiotic is commonly used to erradicate S.aureus from the nasal cavity15, where MRSA and sensitive strains can persist. In this work, was not detected any resistance to mupirocin. Even though the low methicillin resistance rate observed in this work (27.6%), the detection of MRSA strains indicates that they are already difunded at the community, and thus these individuals may serve as a reservoir and source of multiresistant and pathogenic S. aureus strains. The pattern of antimicrobial resistance of the MRSA and methicillin sensitive S.aureus (MSSA) strains were showed in Table 1. The pattern recovered for the MRSA strains were quite different for those already reported16 whose showed multidrug resistance to 9 antibiotics as the principal pattern between the isolates, while in this study only one strain showed resistance to 3 antibiotics. Suggs et al.18 studied the S. aureus colonization in children without risk factors and observed that MRSA strains were widespread in the community. From fifth hundred clildren analyzed, 27.0% were S. aureus carriers and 14.0% of the strains were methicillin-resistant. Since the emergence of MRSA strains, vancomycin has been the only uniformly effective treatment for staphylococcal infections. Hiramatsu et al.19 described the first case of a MRSA strain with reduced vancomycin sensitivite, since than several workers have documented the emergence of these microorganisms12, vancomycin resistance was not detected in this work. In this study, were isolate 7 strains of MRSA from 27 S. aureus carriers members of three families, however further studies are required to establish whether this is a transient presence. We also reported a low resistance to eight antibiotics commonly used in oral terapeutics, follow up of the S. aureus carriers are needed to check the increase in the resistance to antibiotics. Any way, the oral cavity should be considered a potential source of infectious organisms. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os05007f2.jpg] [os05007t1.jpg] [os05007f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}