 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 4, No. 12, Jan./Mar. 2005, pp. 680-684 Cephalometric evaluation of Class III malocclusion by a modified Tweed-Merrifield analysis Mayury Kuramae1 Maria Beatriz Borges de Araújo Magnani2 João Sarmento Pereira Neto2 Darcy Flávio Nouer3 Paulo Roberto Aranha Nouer4 1MDS, DDS Student, FOP/UNICAMP 2DDS, Professor of the Pediatric Clinic, FOP/ UNICAMP 3Chairman, Department of the Pediatric Clinic, FOP/UNICAMP 4Coordinator of the Postgraduation Course, CPO -São
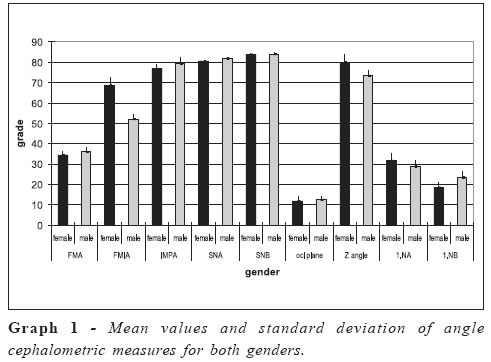
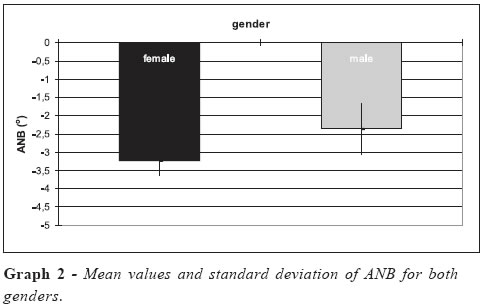
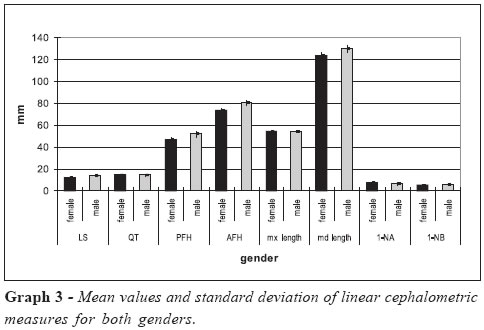
Leopoldo Mandic. Received for publication: March 08, 2004 Code Number: os05008 Abstract A sample of cephalograms of 20 White Brazilian subjects (9 males, 11 females) of 17-36 years old, who presented Class III dental malocclusion was selected and traced. Results showed statistically significant differences among genders for FMIA, SNA, SNB, 1.NB, PFH, AFH, 1-NB and mandibular length. Anteroposterior jaw relation, as shown by SNA and SNB, presented a maxilla correctly positioned, as well as mandibular protrusion, which was related to a normal upper jaw length and an augmented lower jaw length. A vertical growth pattern prevailed, as evidenced by FMA, AFH, PHF and OCC.PL. Angle. The Z Angle, total chin and upper lip failed to clearly show any disturbance of facial esthetics and IMPA, 1.NA, 1- NA, 1.NB and 1-NB revealed dental compensation. Key Words: cephalometrics, class III malocclusion, mandibular prognatism. Introduction
The Class III malocclusion is characterized by a lower jaw mesially positioned in relation to upper jaw, mainly skeletal origin, and its etiology is basically hereditary1. It presents a low prevalence, though this varies among studied regions. In White subjects, it comprehends only 1-2%, but it is more frequent in Asian countries, such as Japan, where it affects about 4-13% of the population2. In Brazil, a prevalence of about 2.93% is estimated3. Class III malocclusion does not imply on a typical facial pattern, and several skeletal profiles can be associated to it and be grouped according to various extents of upper and lower jaw retrognatism4-6. Lower jaw size and position may vary, thus generating a variety of Class III types. Compensation of cephalometric measures such as a low gonial angle while in presence of a large cranial base would neutralize a large lower jaw7. The most significant difference between Class III malocclusion and normal occlusion lies: in the ANB angle, specially due to the protruded lower jaw; in a shorter cranial base which, when rotated, may result in a relative maxillary deficiency, and in an obtuse gonial angle where the temporal fossa is located relatively farther in an anteroposterior direction1. Class III malocclusion presents some striking characteristics, such as dental compensation rate, labialization of upper incisors and lingualization of inferior incisors, especially in permanent dentition. In most of the subjects who show a Class III facial pattern, a facial deficiency is shown in the zygomatic region, especially in the infraorbital area, indicating some degree of midface deficiency; the excessive lenght of the chin-neck line shows the mandibular prognatism5-6,8-9. The purpose of this study was to perform a research based on the Tweed-Merrifield Analysis10 and other measures1112 related to Class III malocclusion, in order to determine mean values for these measures, and verify the occurrence of sexual dimorphism, as well as to interrelate all acquired measures. Material and Methods
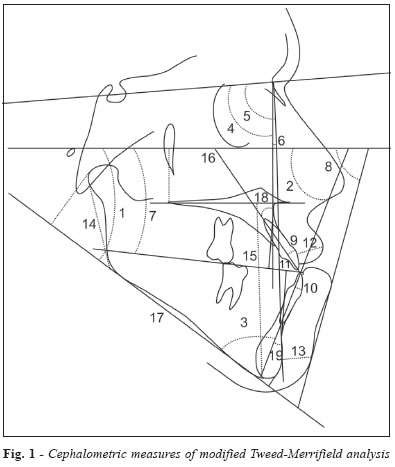
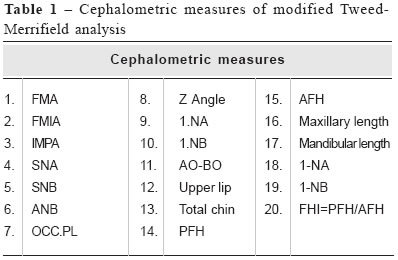
About 400 orthodontic outpatient files were examined from the archives of the service of scientific documentation, Postgraduation Course in Orthdodontics of the College of Dentistry, FOP/UNICAMP, all belonging to White Brazilian subjects of 17-36 years and 4 months old. Twenty of all examined files met the following criteria: Class III molar and canine relationship, confirmed by dental casts and cephalometric measures such as FMA (< 30°) and SN.Gn (<68°), showing a vertical growth pattern. The management of the outpatient files followed the standards of the Health Ministry and the resolution number 196/96 of the National Health Council and was also approved by an Ethics in Human Research Committee - FOP/UNICAMP. The cephalometric tracings were performed by the researcher who was responsible for each subject. Anatomical reference structures were marked, and lines and planes were drawn in order to generate Tweed-Merrifield Analysis10 and other measures11-12 (Figure 1, Table 1). In order to determine the cephalometric tracing error, 20 of the radiographs were twice traced after 10 days, and the arithmetic mean was calculated13. The mean values underwent to a variance analysis and Van der Warden test for non-parametric data at significance level of 5%. Results
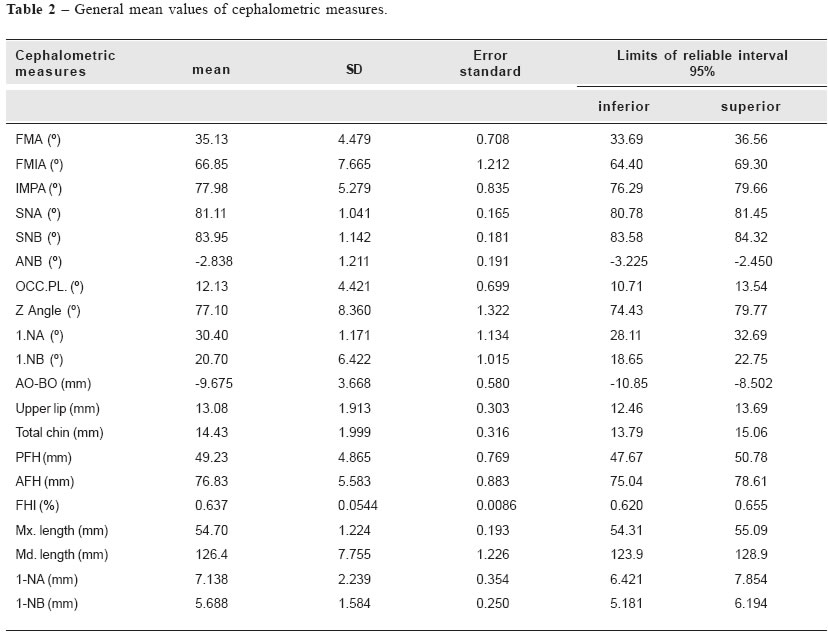
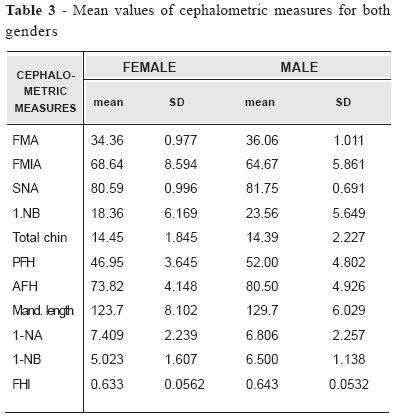
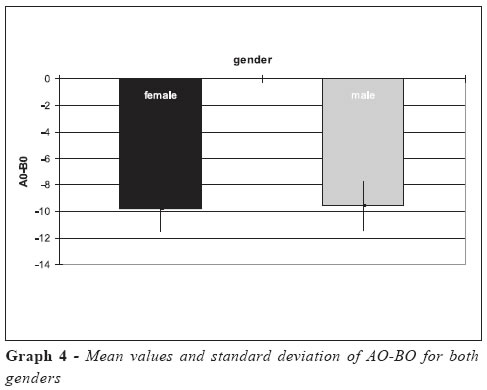
Gender-related statistic data which were evaluated during this study are displayed at Table 2 and 3, Graph 1, 2, 3 and 4. According to the variance analysis, there were statistically significant differences between genders related to the following variables: FMIA, SNA, SNB, 1.NB, PFH, AFH, 1-NB and mandibular lengths (Table 3). Discussion The mean FMA for males was 36.06º, and 34.36º for females, which showed no sexual dimorphism. As this angle indicates the growth direction of the lower face, such results indicate a non-favorable growth vector and a bad prognosis14. The FMIA angle showed a mean value of 64.67º for males and 68.64º for females; such gender differences were statistically significant. IMPA presented a mean value of 79.28º and 76.91º for males and females, respectively, and no statistically significant difference between genders. Proper facial esthetics and balance are only achieved when lower incisors are upright on basal bone with an IMPA variation14 of 90º ± 5º. The mean value observed for IMPA was quite elucidative on lingual inclination of the lower incisors, in relation to the mandibular plane, as a means of compensating the Class III malocclusion1,4,6,8,15-16. For males, the mean value of SNA of 81.75º was observed to be statistically different from the mean value of 80.9º for females. These results showed that the position of upper jaw, as related to the cranial base, was close to the standards. Mean values of SNB were 84.11º for males and 83.82º for females, presenting statistical difference between genders. Vertical growth displaced the pogonion into a lower position, while anteroposterior growth leaded it anteriorly. These growth directions can result either in prognatism or retrognatism, depending on each facial pattern. ANB mean value was -2.36º for males, and -3.23º for females, and presented no significant differences. This means a mandibular protrusion relating to the cranial base, since the upper jaw was in a normal position. Results then demonstrated an evident mandibular protrusion1,4, and also showed that, for this sample, while the upper jaw was correctly positioned relating to the cranial base, the lower jaw was the responsible for the Class III malocclusion. Maxillary lengths were observed to be larger for males (54.89mm) than for females (54.55mm), and mandibular lengths were also statistically different for males (129.70mm) and females (123.70mm). Thus, though the upper jaw was correctly positioned, its length, as well as the mandibular length, was not on normal standards. The mean values for the Z Angle17, for males (73.44º) and females (80.09º) were not significantly different. These values showed angular values almost similar to normal standards; this might be explained by the vertical facial type of these subjects, which displaced pogonion downward and backwards. Mean values for upper lip of this sample were 13.89mm for males and 12.41mm for females, and also did not show gender dimorphism. The soft tissues represent upper lip and total chin and reflect the subjacent skeletal structures. AO-BO measured -9.55mm for males and -9.77mm for females, showing no gender-related differences. The Wit’s appraisal, according to the resulting values, queries the ANB angle18, though our results evidence the great anteroposterior divergence of both jaws, which excluded possible measuring errors resulting from cephalometric point variations and rotational effect of the jaws. The mean values for PFH (posterior facial height)19 were 52.00mm for males and 46.95mm for females, showing statistically significant difference between genders. Mean values of AFH (anterior facial height)19 were 80.50mm for males and 73.82mm for females, showing statistically significant difference between genders. The higher value of AFH in the Class III malocclusion showed mandibular growth and a clockwise rotation, what would result in a vertical growth pattern with steep horizontal planes5,6. In the case of FHI (facial height index)20, mean values for males (0.64) and females (0.63) did not show significant difference between genders. There were no significant differences between genders for 1-NA, which has shown values of 6.81mm for males and 7.41mm for females. The resulting mean values for 1.NA were 28.89º for males and 31.84º for females. Both of these measures reflected a dental compensation to protrusion and inclination of the upper incisors that occur in Class III malocclusion1,5-6,8-9. 1-NB presented mean values of 6.50mm for males and 5.02mm for females, showing sexual dimorphism. 1.NB presented mean values of 25.36º for males and 18.36º for females, indicating higher values for males and, thus, the lingual inclination in females was greater. In this study the occlusal plane (OCC.PL.) angle was 12.5º for males and 11.82º for females, showing no significant difference. The steeper of all occlusal planes showed a greater divergence, caused by the clockwise rotation of the jaws, thus presenting a greater challenge to orthodontic therapeutics. Acknowledgments To FAPESP, for providing a master degree scholarship (process nº 00/04351-2). References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os05008t1.jpg] [os05008g4.jpg] [os05008g1.jpg] [os05008t3.jpg] [os05008g2.jpg] [os05008g3.jpg] [os05008t2.jpg] [os05008f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}