 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
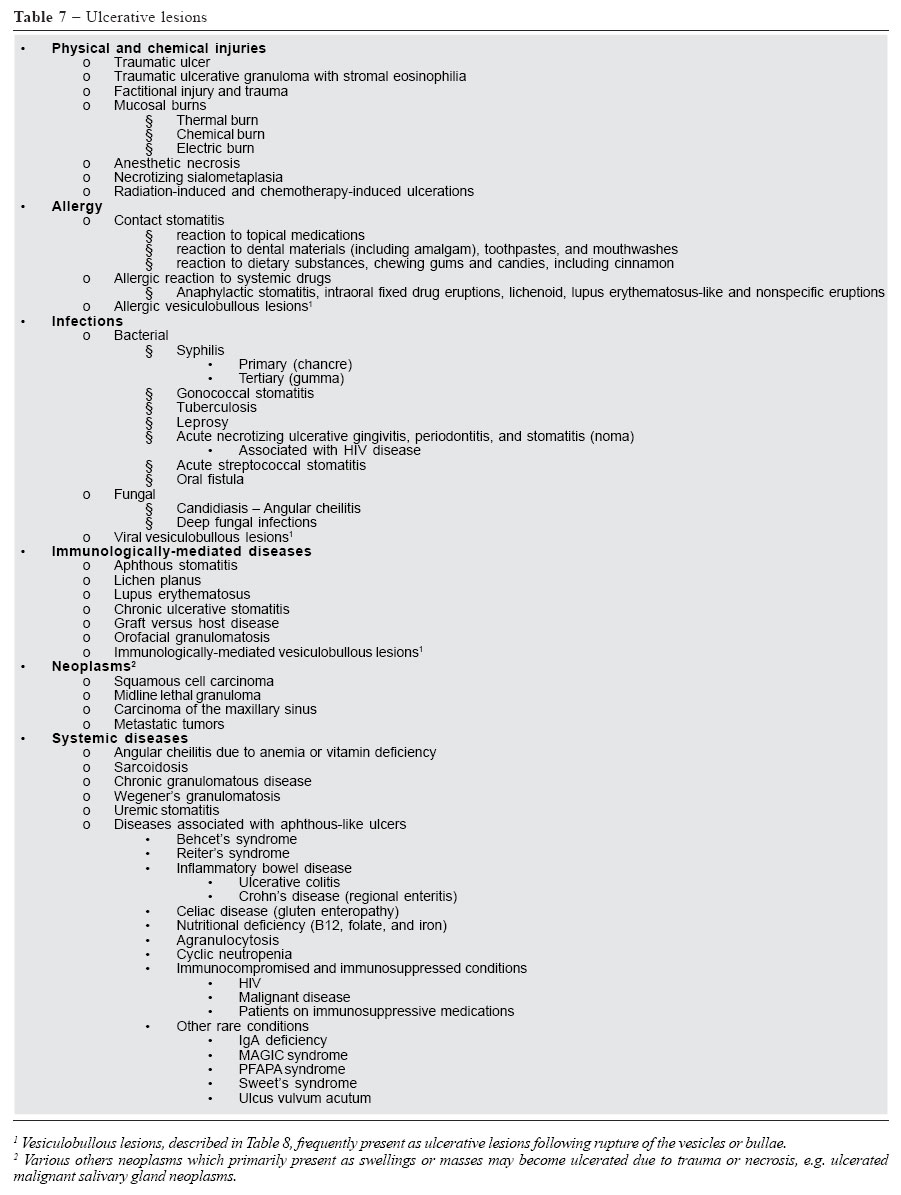
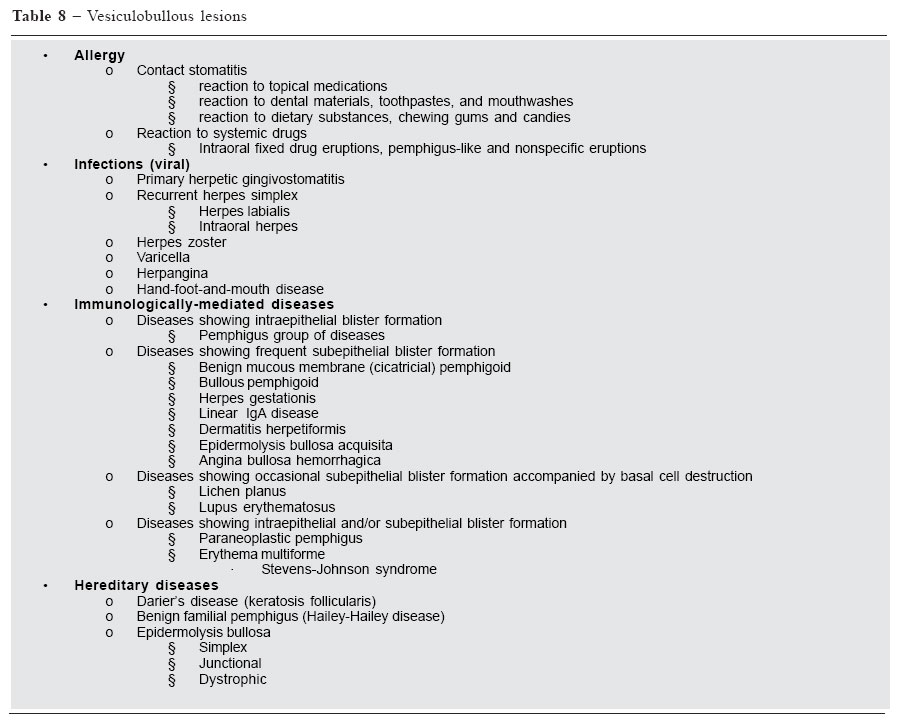
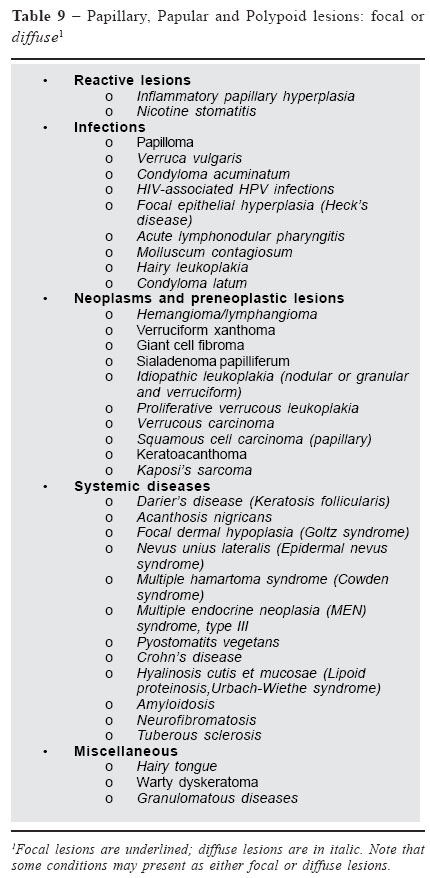
Oral soft tissue lesions: A guide todifferential diagnosisPart II: Surface alterations Nikolaos G. Nikitakis DDS, PhD, Assistant Professor and Program Director, Department of Diagnostic Sciences and Oral soft tissues are affected by a multitude of pathologic conditionsPathology and Greenebaum Cancer Center, University of Maryland, Baltimore, USA Correspondence to: NG Nikitakis Department of Diagnostic Sciences and Pathology, Room 4-C-02 Dental School, University of Maryland, Baltimore 666 West Baltimore St., Baltimore, MD 21201 Phone: 410-706-7936 / FAX: 410-706-0519 E-mail: nin001@ dental.umaryland.edu Received for publication: January 10, 2005 Code Number: os05012 Abstract Oral soft tissues are affected by a multitude of pathologic conditions of variable etiology and significance; their appropriate management relies on their accurate diagnosis. Considerable overlapping of the signs and symptoms produced by these diverse conditions poses significant problems for their diagnosis, which can be resolved only through a thorough knowledge of the clinicopathologic characteristics of each condition and a systematic approach to diagnosis. An essential component of the diagnostic process is the formulation of a differential diagnosis, which encompasses the possible diseases and conditions that could account for a specific constellation of oral signs and symptoms. To facilitate the challenging task of differential diagnosis, this review provides comprehensive lists of the various pathologic conditions that pertain to specific oral soft tissue changes. The latter are classified into three major categories: 1) changes in color, 2) surface alterations, and 3) masses or swellings. The first part of this review offered some general considerations for the differential diagnosis of oral mucosal and submucosal lesions and presented the various pathologic conditions that result in color alterations of oral soft tissues. In the second part, lesions producing surface alterations will be reviewed. On the basis of their clinical presentation, the surface alterations of oral tissues are classified into 1) ulcerative, 2) vesiculobullous, and 3) papillary, papular or polypoid lesions; these lesions are further subclassified according to their etiology and/or pathogenesis. The salient features of each disease category and the most important specific diseases are reviewed and recommendations for specific diagnostic approaches and tests are provided. Key Words: ulcerative lesions, vesiculobullous lesions, papillary lesions. C. Surface Alterations1 A plethora of pathologic conditions may affect the normal morphologic characteristics and intactness of the oral mucosa, presenting as surface alterations. These changes on the surface of the oral mucosa can be divided into 3 major groups: 1) ulcerative, 2) vesiculobullous, and 3) papillary, papular or polypoid lesions. While both ulcerative and vesiculobullous lesions eventually manifest a similar clinical appearance, consisting of mucosal ulcerations and/or erosions, their difference lies in their initial presentation: the loss of tissue in vesiculobullous lesions is preceded by the formation of blisters which eventually rupture to form ulcers and erosions; in contrast, the so-called ulcerative lesions appear as ulcers from the outset in the absence of a previously identifiable clinical stage. On the other hand, papillary, papular or polypoid lesions would encompass lesions caused by pathologic changes involving the mucosa that distort the normal appearance of the mucosal surface and assume an exophytic presentation, without significant extension to the deeper submucosal tissues. Involvement of deeper structures causes a clinical manifestation of a mass or swelling and will be covered separately.2 C1. Ulcerative lesions A number of pathologic conditions that afflict the oral mucosa are characterized by loss of tissue and present as erosions (superficial loss of tissue that involves only the epithelium) or ulcerations (deeper lesions that extend into the connective tissue). As mentioned before, only lesions that begin as erosions or ulcers will be described in this paragraph, classified according to their etiology and/or pathogenesis (Table 7). Nonetheless, the possibility that the observed loss of tissue is the result of a rupture of previous blisters should be evaluated by questioning the patient and by careful clinical examination for the presence of remaining intact vesicles. It should be also kept in mind that erosions or ulcers may be covered by a fibrinous pseudomembrane, imparting a whitish or yellowish clinical appearance; close clinical examination is usually sufficient to distinguish between bona fide white lesions and pseudomembrane-covered ulcerations. Additionally, an erythematous or white periphery is a usual component of specific ulcerative lesions, which can facilitate their diagnosis. In general, the morphology of the ulcerative lesion including its shape, size, border and base characteristics, as well as the presence or absence of a pseudomembrane and/ or peripheral component, provide important and sometimes definitive clues to the diagnosis. Equally important to the accurate description of the morphologic features of ulcerative lesions is the assessment of their number (single vs. multiple), onset and duration (acute vs. chronic), and potential for recurrence (recurrent vs. non-recurrent). Although overlapping features among ulcerative lesions of widely variable etiology and significance are expected, the combination of a thorough history, careful clinical examination and sometimes physical evaluation, and appropriate laboratory investigations, including biopsy, will afford a definitive diagnosis. Reactive lesions, including physical and chemical injuries and allergies must always be included in the differential diagnosis of oral ulcerative lesions. Especially, traumatic ulcers, either accidental (e.g. tongue biting) or less often factitious in origin, are among the most commonly encountered oral ulcers. Identification and removal of the traumatic stimulus should induce complete healing in no more than 2 weeks. Failure of the lesion to heal after elimination of suspected traumatic (or other reactive) causes should always prompt a re-evaluation of the diagnosis and biopsy. Nevertheless, persistent oral ulcerations of traumatic etiology have been described as traumatic ulcerative granulomas with stromal eosinophilia; the persistence of these lesions along with their atypical clinical features (e.g. indurated hard borders) raises the possibility of malignancy and dictates the need for biopsy. Mucosal burns of diverse origin, already described as potential causes of white and/or red lesions,3 may be severe enough to induce loss of tissue with resulting formation of erosions or ulcers. Similarly, oral ulcerative lesions are a common manifestation of severe radiation-induced and chemotherapy-induced mucositis. Anesthetic necrosis and necrotizing sialometaplasia constitute less frequent reactive ulcerative lesions, which have both been associated with ischemia; the clinical and histopathologic similarity between necrotizing sialometaplasia and malignant palatal tumors necessitates biopsy and careful histopathologic analysis of this innocuous, self-limiting lesion. Finally, both local factors (e.g. topical medications, dental and dental hygiene products and dietary substances) and systemic drugs may induce allergic reactions that, instead of or in addition to previously described white and/or red lesions,3 may show mucosal ulcerative changes. Systemic drug reactions may be nonspecific, may constitute components of an anaphylactic or fixed drug reaction, or may resemble other conditions, such as lichen planus or lupus erythematosus. Discontinuation of the suspected allergen, detection of which is often challenging, should eliminate the lesion, thus confirming the diagnosis. Ulcerative lesions of the oral mucosa may have an infectious etiology. Sexually-transmitted diseases may generate oral ulcers, such as the chancre and gumma of the primary and tertiary syphilis, respectively; history of contact with an infected individual, detection of other signs and symptoms of the disease, and proper laboratory investigations will secure a final diagnosis. Infectious granulomatous diseases, including tuberculosis, leprosy and deep fungal infections, may also produce oral ulcers, which may resemble oral cancer or other ulcerative conditions; biopsy of these lesions will show the characteristic features of granulomatous inflammation, while the use of special stains (e.g. acid fast for M. tuberculosis and M. leprae) and other laboratory techniques (e.g. culture or polymerase chain reaction) will reveal the presence of specific pathogenic organisms within the granulomas. Acute ulcerative necrotizing gingivitis (ANUG), periodontitis, and stomatitis form a spectrum of related entities of similar bacterial etiology, featuring different degrees of clinical involvement. ANUG is limited to the gingiva, typically causing “punched-out” blunting of the papillae, associated with pain, fetid odor and variable constitutional symptoms. Extension of the necrotic ulcerative tissue to the periodontium (periodontitis) and surrounding mucosa (stomatitis) or even to the underlying bones and facial skin (noma) is possible. All these entities are frequently precipitated by stress or immune suppression, including cases associated with HIV infection, therefore identification and correction of a potential immunocompromised status is essential. Moreover, oral fistulae, representing drainage tracts of periapical or periodontal abscesses, osteomyelitis or actinomycosis, may be clinically indistinguishable from oral ulcerations; tooth vitality tests, probing with a gutta-percha point and radiographic examination will point to the correct diagnosis. Finally, erosions caused by the rupture of preexistent virally-induced vesicles are described later as vesiculobullous lesions. One of the most common causes of oral ulcers is recurrent aphthous stomatitis, a condition associated with a T-cell mediated immunologic reaction and stimulated by a myriad of possible predisposing events. Knowledge of the clinical variations of the disease (minor, major and herpetiform), location in non-keratinized mucosa (with the exception of herpetiform ulcers that may also affect hard tissue-bound mucosa), and history of recurrences should allow a strong presumptive diagnosis, which, in questionable cases, is corroborated by the histologic findings of a non-specific ulceration. The remainder of the oral ulcerative lesions of immunologic etiology usually begins as blisters and is described along with the vesiculobullous lesions. However, lichen planus and lupus erythematosus (previously described as potential causes of white and/or red lesions)3 frequently demonstrate an erosive/ulcerative component in the absence of a previous vesiculobullous stage. Chronic ulcerative stomatitis and graft versus host disease can also present with erosive lesions of lichenoid appearance. Definitive diagnosis of these lesions requires biopsy and histopathologic examination often combined with immunofluorescence studies. A vast array of systemic diseases are associated with the formation of aphthous-like ulcers in the oral mucosa; hence, evaluation for and treatment of diverse conditions such as Behcet’s syndrome, gastrointestinal disorders, hematological abnormalities, and immunosuppressive states, are recommended in cases of severe or recalcitrant aphthous-like ulcers or when the medical history suggests an underlying systemic abnormality. Systemic granulomatous diseases, such as sarcoidosis, chronic granulomatous disease, and Wegener’s granulomatosis, should be included in the differential diagnosis of oral ulcers and distinguished from cases of idiopathic (oral granulomatosis) or infectious (mycobacterial or fungal) etiology; in this regard, assessment of systemic signs, chest radiographs, special stains for microorganisms, and specific laboratory tests (e.g. angiotensin converting enzyme levels for sarcoidosis or antineutophil cytoplasmic antibody detection for Wegener’s) provide valuable diagnostic information. Lastly, angular cheilitis, which manifests itself as ulceration or erythema of the commissure, may be attributed to systemic causes, (anemia or vitamin deficiency), infection (fungal or staphylococcal), or local factors (loss of vertical dimension). Lastly and more importantly, oral ulceration is the most frequent clinical presentation of squamous cell carcinoma, the most common type of cancer to affect the oral cavity. Although induration, irregular shape, rolled borders and location along the lateral border of tongue or floor of mouth constitute the most frequent characteristics of oral cancer, any location may be affected by lesions that may mimic the clinical features of other benign ulcerative lesions of the oral mucosa. Thus, squamous cell carcinoma should be always included in the differential diagnosis of an oral ulcer; biopsy and histopathologic examination is diagnostic and necessary in all cases, with the exception of oral ulcers that heal completely in less than 2 weeks either spontaneously (e.g. aphthous ulcers) or after removal of an identified etiologic factor (e.g. traumatic ulcer). It should be kept in mind that, besides oral squamous cell carcinoma, other types of malignancies that afflict the oral cavity, including metastatic tumors, may manifest an ulcerative component due to trauma or necrosis. C2. Vesiculobullous lesionsDiseases and conditions of diverse etiology and prognosis may manifest in the oral cavity as fluid-filled blisters, which according to their size may be further distinguished as vesicles (less than 5mm) or bullae (more than 5mm) (See Table 8). Clinical identification of intact vesicles and bullae is more difficult in the oral cavity than the skin in that the oral lesions tend to rupture easily because of the friable nature of the oral mucosa and the continuous exposure to mechanical irritation. Moreover, the friability of oral vesicles and bullae depends on their exact position with intraepithelial lesions being more prone to rupture. As mentioned before, rupture of an oral blister results in the formation of erosions or ulcerations, eliciting a differential diagnosis which includes not only vesiculobullous but also ulcerative lesions (see Table 7). The location and distribution of vesiculobullous lesions in the oral mucosa, as well as their acute, recurrent, or chronic nature, provide valuable clues to their diagnosis. In addition, the presence or absence of accompanying skin lesions and constitutional symptoms, such as fever, facilitate their accurate classification. Allergic reactions to local factors or systemic medications, already incriminated in the development of white/red3 and ulcerative lesions of the oral mucosa, may be also responsible for the formation of oral vesiculobullous lesions. Some of these reactions may mimic specific disease entitities (e.g. lichenoid or pemphigus-like lesions), while others are nonspecific, often featuring a combination of erythematous, blistering and erosive/ulcerative areas. Identification of a potential allergen should be based on the temporal relationship between the exposure to the allergen and the development of the lesions. In cases of contact stomatitis, the location of the lesions should also coincide with the areas of allergen exposure. Nevertheless, detection of the responsible offending agent is often a difficult task, especially in cases of chronic allergic reactions. Skin or direct oral tests may be used, while resolution of the oral lesions upon elimination of the allergen will provide confirmation of the diagnosis. A number of viral infections, caused by members of the human herpesvirus and Coxsackievirus families, may affect the oral mucosa and present as vesicles. Human herpes simplex virus (HSV) type I (and less frequently type II) are responsible for primary and secondary herpetic infections, which constitute the most common vesicular lesions, as well as the most common viral diseases of the oral cavity and lips. The first exposure to the virus is frequently asymptomatic; however, symptomatic disease, termed primary herpetic gingivostomatitis, occurs often, characterized by diffuse involvement of the oral mucosa and gingiva, constitutional symptoms of fever, malaise and lymphadenopathy, and spontaneous healing in 10-14 days. Whether symptomatic or not, exposure to the virus results in indefinite latency in the ganglia of the nervous system; reactivation of the virus, instigated by various predisposing factors (such as sun exposure, respiratory illnesses, and stress) gives genesis to episodes of secondary or recurrent herpes, usually involving the lips (herpes labialis) but also sometimes affecting intraoral sites. In immunocompetent patients, the intraoral lesions of recurrent herpes are restricted to the gingiva and palatal mucosa, which helps to rule out a number of diseases (e.g. minor or major aphthous ulcers) from the differential diagnosis. Focal clustering of the herpes-induced vesicles is typical. Although the aforementioned clinical features are usually sufficient for a strong presumptive diagnosis, special tests for confirmation are available, including examination of cytologic smears for typical herpes-induced epithelial nuclear changes, biopsy, viral culture, or serologic assessment of antiherpes antibodies. Atypical and persistent presentations may suggest the possibility of immunosuppression, including AIDS. Varicella-zoster virus (VZV), another member of the human herpesvirus family, may cause oral lesions due to primary exposure, which causes the childhood infection varicella (or chickenpox), or due to reactivation of the latent virus, which presents in adults as herpes zoster (or shingles). Chickenpox features a characteristic skin exanthema accompanied by constitutional symptoms, while shingles is typified by unilateral vesicular, painful lesions which follow the distribution of a sensory nerve. If necessary, confirmation of the diagnosis can be obtained by cytologic examination of the vesicle content for nuclear changes, viral culture or determination of VZV antibody titers. Coxsackievirus may also cause oral vesicular lesions in the form of herpangina, with lesions essentially limited to the soft palate and oropharynx, or hand-foot-and-mouth disease, with a pathognomonic distribution of vesicles in the mouth and distal extremities. Again, viral culture and measurement of antiviral antibody titers may confirm the clinical diagnosis. Many diseases of immunologically-mediated origin involve the oral mucosa producing vesiculobullous lesions; some of these conditions are exceedingly rare, while others constitute a common problem for many patients. In general, the oral lesions consist of blisters of varying size which rupture to produce erosions or ulcerations; a positive Nikolsky sign, i.e. induction of a blister in normal-looking mucosa by exerting pressure, is frequently positive but not capable of distinguishing between the different immunologically-mediated oral blistering diseases. Although the oral clinical features of these conditions are similar and largely indistinguishable, knowledge of the systemic associations of each disease, including the potential for skin or other organ involvement, facilitates their discrimination. For example, pemphigus vulgaris and bullous pemphigoid are characterized by skin involvement in virtually all cases; however, the frequency of oral lesions differs, with pemphigus vulgaris showing oral involvement in nearly all cases, while bullous pemphigoid only occasionally shows oral manifestations. On the other hand, cicatricial pemphigoid very rarely involves the skin, being primarily a mucosal condition, which, in addition to mouth, may affect other mucosal surfaces including the eyes; notably, the ocular lesions, if left untreated, may progress to blindness. Further, certain immunologic diseases that affect the oral mucosa exhibit additional specific clinical findings, such as the presence of targetoid lesions and hemorrhagic crusted lips in erythema multiforme. Moreover, some of these diseases are pathogenetically linked to other pathologic conditions, as is the case between erythema multiforme and a preceding herpetic recurrence or between paraneoplastic pemphigus and neoplasms of lymphoreticular origin. Despite the aforementioned clinical correlations, the final diagnosis is largely based on the results of the biopsy; on many occasions, the histopathologic findings should be supplemented by direct or indirect immunofluorescence studies in order to render a specific diagnosis. Lastly, hereditary diseases may also account for the formation of oral vesiculobullous lesions. Among those, epidermolysis bullosa (which also occurs in adults as an immunopathologic condition) affects children and is classified into various subtypes, showing disparities in the mode of inheritance, clinical findings, and severity. Oral blistering lesions are mainly present in the dystrophic variants of the disorder, in contrast to dental defects that are primarily seen with the junctional type. C3. Papillary. papular and polypoid lesionsThe various conditions that cause papillary, papular and polypoid lesions of the oral mucosa are listed in Table 9, classified on the basis of their etiology. Although these lesions are by definition morphologically different, with papillary (or verrucous) lesions exhibiting pointed or blunt finger-like projections, papular lesions featuring small sessile elevations, and polypoid lesions consisting of larger, often pedunculated, exophytic growths, they are overall similar and can be confused with each other. For the purposes of formulating a thorough differential diagnosis, it is practical to consider all these lesions as a group, characterized by exophytic distortions of the oral mucosa in the absence of a significant submucosal component. Specific characterization of these conditions can be facilitated by dividing them into two major categories, focal and diffuse (see Table 9); nevertheless, several of them may present as either focal or diffuse, complicating their diagnosis. Two common reactive conditions of the palate, inflammatory papillary hyperplasia and nicotine stomatitis, are included in the differential diagnosis of diffuse papillary/papular lesions. The former is almost always associated with chronic trauma induced by a maxillary denture and is occasionally complicated by a fungal infection (denture stomatitis), while the latter is a smoking-induced reactive condition which causes an almost pathognomonic combination of white papules with red depressed centers. Interestingly, nicotine stomatitis is not a premalignant lesion itself but, as a sign of heavy smoking, should prompt a complete evaluation for identification of dysplastic or malignant changes elsewhere. Various human papillomavirus (HPV) subtypes may cause papillary lesions of the oral mucosa. Papilloma, a focal pedunculated or sessile growth with a cauliflower surface, is the most frequently encountered HPV-induced lesion in the oral cavity. On the other hand, verruca vulgaris, the most common wart-like lesion of the skin, is infrequent in the mouth, with the exception of the vermillion border. Condyloma acuminatum, a sexually transmitted disease, shows almost identical lesions, which, however, exhibit a diffuse or multifocal distribution; a strong presumptive diagnosis can be made on the basis of the presence of similar genital lesions or history of sexual contact with affected individuals. HPV-induced oral papillary lesions are seen with increased frequency among HIV-infected individuals; these lesions are multiple, associated with rare HPV subtypes, and occasionally harbor dysplastic changes. HIV patients may also develop lesions resembling focal epithelial hyperplasia; the latter is a multifocal papillary condition mainly seen in children of Native American or Eskimoan descent. Biopsy and histopathologic examination may reveal subtle histomorphologic differences among HPV-associated entities contributing to their accurate diagnosis; moreover, DNA in situ hybridization and immunohistochemical techniques allow specification of the responsible HPV subtype, a finding of potential significance in the face of the purported association between specific HPV species and dysplasia. In addition to HPV, other viruses may also generate papillary or papular oral mucosal lesions, including the Coxsackievirus-induced acute lymphonodular pharyngitis that preferentially involves the oropharynx in the presence of constitutional symptoms of infection. Hairy leukoplakia, an Epstein-Barr virus-induced white lesion seen in HIV-infected and other immunocompromised individuals and typically located along the lateral border of tongue, may appear as a papillary lesion due to multiple keratin projections on the surface of the lesion. A number of preneoplastic lesions and neoplasms may incur a papillary/papular/polypoid appearance of the oral mucosa. Most of these lesions are usually associated with characteristic color changes and were described in the first part of this review.3 For example, hemangioma and Kaposi’s sarcoma are vascular neoplasms with a red, bluish or purplish hue, occasionally producing a papular configuration of the overlying mucosa. Similarly, lymphangioma, a neoplastic or hamartomatous lesion of lymphatic vessel origin, usually presents as a mass covered by multiple, clustered translucent papules assuming the appearance of frog eggs or tapioca pudding. Verruciform xanthoma, a rare lesion that may exhibit a white, red or yellowish discoloration, is a well-demarcated nodule with a papillary or roughened surface. Giant cell fibroma is histologically and clinically similar to an irritation fibroma with the additional features of stellate-type giant cells and a frequent pebbly surface. Sialadenoma papilliferum belongs to the family of benign salivary gland tumors of papillary histomorphology; because of its origin in the superficial portion of the excretory duct system, the lesion frequently manifests clinically as a papillary mucosal lesion. Specific diagnosis of all the aforementioned neoplastic lesions relies upon biopsy and identification of their corresponding histopathologic features. Likewise, histopathologic examination is of paramount importance for the diagnosis of the premalignant lesions of the oral mucosa that may cause a papillary mucosal alteration; lesions in this category include the nodular, granular and verruciform variants of leukoplakia, as well as the clinical entity of proliferative verrucous leukoplakia. The latter is a very high risk form of leukoplakia characterized by: a predilection for women and non-smokers, a multifocal, verruciform clinical appearance, a relentless spreading growth, and a high rate of malignant transformation to verrucous or squamous cell carcinoma. Squamous cell carcinoma itself, already described along with the ulcerative lesions of the oral mucosa, may appear as an exophytic mass that assumes a fungating, papillary, or verruciform configuration. Induration, frequently accompanied by surface ulceration, raises the suspicion of malignancy, the definitive diagnosis of which should be always confirmed by biopsy. Finally, verrucous carcinoma is a low-grade variant of squamous cell carcinoma, often seen in individuals using smokeless tobacco; its typical clinical presentation is that of an extensive, papillary or verruciform mass of white or less commonly red color. Although this tumor very rarely metastasizes, it is locally destructive, may be associated with concurrent or metachronous development of squamous cell carcinoma and should be treated with complete removal. A vast array of systemic diseases may produce oral papillary, papular and/or polypoid lesions. Although the clinical features of the corresponding oral lesions are not identical, they show significant similarities, including a common tendency for diffuse and/or multifocal involvement of the oral mucous membranes. Because of the commonalities in appearance, a long differential diagnosis is usually formulated, the resolution of which requires knowledge of the systemic manifestations and the histopathologic characteristics of each one of these diseases. Family history is particular important in that many of these diseases are hereditary, e.g. keratosis follicularis, neurofibromatosis, multiple endocrine neoplasia type III, tuberous sclerosis or Cowden syndrome are often transmitted as autosomal dominant traits, while hyalinosis cutis et mucosae and focal dermal hypoplasia are inherited in an autosomal recessive and X-linked dominant fashion, respectively. Moreover, the presence and pattern of skin lesions and/or internal organ involvement may help narrow the list of potential diagnoses; for instance, rough, pruritic skin papules in keratosis follicularis, multiple neurofibromas and café au lait macules in neurofibromatosis, or gastrointestinal signs and symptoms in Crohn’s disease and pyostomatitis vegetans offer significant diagnostic clues. Additionally, an association with internal malignancies is typical of several of these disorders: acanthosis nigricans, Cowden syndrome, multiple endocrine neoplasia, neurofibromatosis, and selective types of amyloidosis are all associated with increased risk of specific types of malignancies; therefore, diagnosis of these systemic diseases by the presence of oral lesions in combination with other signs and symptoms will allow recognition of the risk for malignant transformation followed by institution of appropriate preventive measures. Biopsy of oral lesions and identification of specific histologic findings, such as amyloid deposits in amyloidosis, plexiform neurofibromas in neurofibromatosis, fibroepithelial polyps in Cowden syndrome, or mucosal neuromas in multiple endocrine neoplasia type III is often instrumental for the final diagnosis. Nonetheless, the complexity of these disorders will often require co-ordination with other medical specialties in order to establish the diagnosis and implement proper therapeutic and preventive interventions. Finally, a few miscellaneous conditions that are not easily classified in anyone of the above categories may be responsible for papillary or papular lesions of the oral cavity, including hairy tongue and warty dyskeratoma. The former refers to an elongation of the filiform papillae of the tongue and may cause a white or pigmented appearance of the dorsal tongue,3 while the latter is a solitary lesion with histologic features that resemble follicular keratosis. Further, the oral lesions of various granulomatous diseases of diverse origin, for example tuberculosis or histoplasmosis, may evince a granular or papillary surface, in addition to aforementioned granulomatous ulcerations. Footnotes
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}