 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
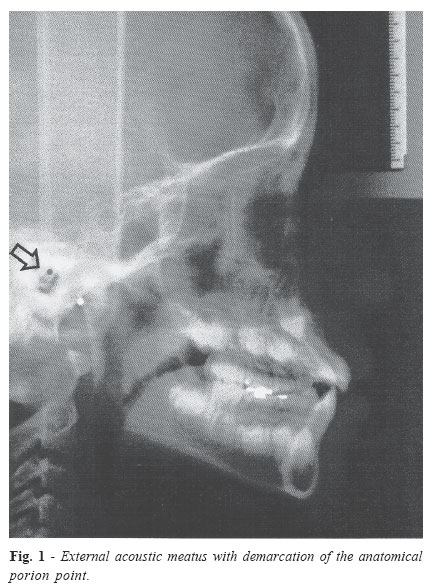
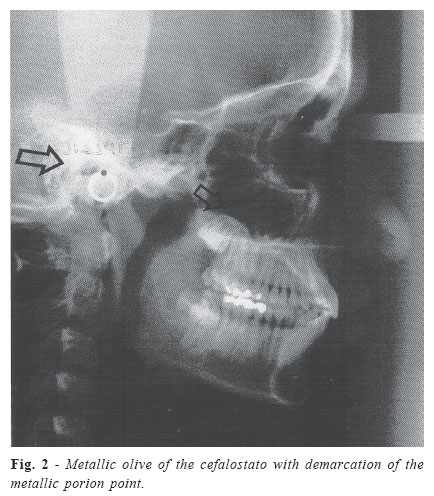
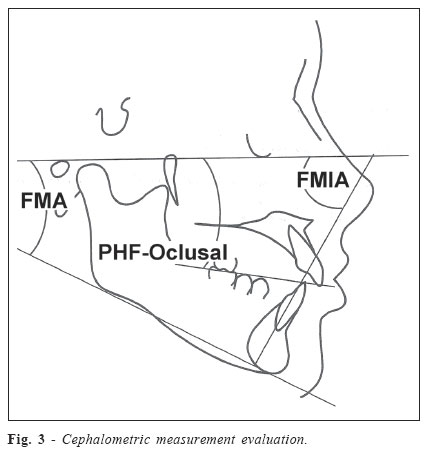
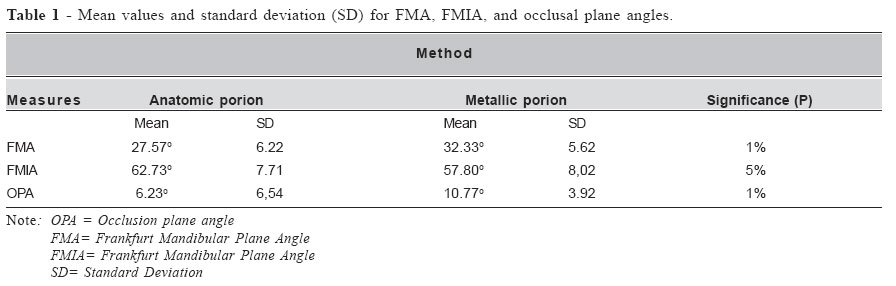
Brazilian Journal of Oral Sciences, Vol. 4, No. 13, April./June. 2005, pp. 730-734 Comparison between cephalometricsmeasure using anatomic and metallic porion point Fábio Lourenço Romano1 Edvaldo Luiz Ramalli2 Stenyo Wanderley Tavares2 João Sarmento Pereira Neto3 Maria Beatriz Borges de Araújo Magnani3 Darcy Flávio Nouer3 1MS Orthodontics, Pediatric Dentistry Department, University of Campinas, Piracicaba Dental School – Brazil; Professor, Department Restorative Prosthestic, Alfenas Dental and Pharmacy School, Brazil 2 DDS, MS, PHD student, Pediatric Dentistry Department, University of Campinas, Piracicaba Dental School – Brazil 3 DDS, MS, PHD, Professor, Pediatric Dentistry Department, University of Campinas, Piracicaba Dental School – Brazil Correspondence to: Fábio Lourenço Romano Avenida do Café, 131 Bloco E- Ap. 16 Vila Amélia - Ribeirão Preto – SP CEP: 14050-230 E-mail:flromano@aol.com Received for publication: March 04, 2004 Code Number: os05015 Abstract The aim of this study was to compare the cephalometric measures involving FMA (Frankfurt Mandibular Plane Angle), FMIA (Frankfurt Mandibular Incisor Angle), and occlusal plane angles (Frankfurt horizontal plane - occlusal plane) for cephalometric tracing by using anatomic and metallic porion points. Cephalometric tracing was performed in thirty head lateral teleradiographs divided into two groups. The anatomic porion point was marked in group 1, whereas metallic porion point was marked regarding the Frankfurt horizontal Plane (FHP). All measures were analysed. The mean values for FMA (32.33°) and occlusal plane angles (10.77°) in group 2 were statistically higher than those found in group 1 (FMA - 27.57°); occlusal plane angle - 6.23°). The mean value for FMIA angle (62.73°) in group 1 was statistically higher when compared to group 2 (57,80°). According to these results, one can conclude that cephalometric tracing of porion points (either anatomic or metallic) alter the values for FMA, FMIA, and occlusal plane angles, thus resulting in different treatment plans. Key Words:orthodontics, cephalometrics, porion point, Frankfurt Horizontal Plane Introduction The introduction of Cephalostat to the radiographic procedures in 1931 by Broadbent1 provided a standardized method of accurately recording craniofacial structures and relationships in living individuals. Lateral cephalometric radiography has become widely used in orthodontics as an important descriptive, analytic and diagnostic technique2-4. Many references on radiographic cephalomtry have been proposed and used. Some were derived from earlier craniometric studies, while others were introduced with the development of radiographic cephalometry5-6.One of these contributions from the craniometric studies was done by Von Ihering, in 1872, who idealized a horizontal plane which was selected as being the universal reference plane during the Frankfurt Congress of Anthropology held in 1884. Such a horizontal plane is a tracing from the superior part of the external auditory meatus (anatomic porion point) to the inferior rim of the left orbital cavity (orbital point), thus being named as Frankfurt Horizontal Plane (FHP). This plane is considered, even today, as a basic plane in certain cephalometric analysis7-10. Tweed10, in 1953, presented a diagnostic facial triangle based on Frankfurt horizontal plane, which is composed, by the FMA (Frankfurt Mandibular Plane Angle), FMIA (Frankfurt Mandibular Incisor Angle) and IMPA (Incisor Mandibular Plane Angle) angles. The FMA angle formed by FHP and mandibular plane (Go - Me) has a mean value of 24.57o, the FMIA angle formed by FHP and the long axis of the inferior incisor has a mean value of 68.20o, and the IMPA angle formed by the mandibular plane and the long axis of the inferior incisor with mean value of 86.93o. The anatomic porion point is localized at the uppermost external auditory meatus, thus making difficult its lateral teleradiographic visualization. Such a difficult location is due to the following: density of the petrous temporal bone, projection juxtaposition of the corresponding left and right pyramids, and kilovoltage employed, which rarely allow satisfactory visualization of such a region11-12. However, its marking should be performed despite the bad visibility since the porion may not be directly visible and as a result, it must be anatomically interpreted, that is, positioned between 8 and 10 mm at oblique plane of 45o, passing through its inferior homologue13. Because of the frequent identification mistakes, which consequently affect the marking, the use of metallic porion point was conventionally adopted in order to replace the anatomic porion point. The metallic porion point is located at 4.5 mm above the centre of the cephalostatic radiopaque image of the auricular olives12,14. While most orthodontists use the anatomic porion point, others use the metallic porion for tracing the Frankfurt Horizontal Plane without worrying about the differences, which may exist involving some cephalometric measures. In the face of the lack of standardization and the scarce literature concerning this subject, the aim of this work was to compare the FHP marking based on both anatomic and metallic porion point by verifying the degree of variability involving FMA, FMIA, and occlusal plane angles. Material and MethodsThis study was performed by using thirty head lateral teleradiographs selected from the Scientific Documentation Sector of the Faculty of Dentistry of Piracicaba, UNICAMP. All x-ray examinations were taken by the same professional, with the same equipment, at a distance of 1.50 m from the patient’s face (Rotograph Plus, Villa Sistem Medical, Italy) in order to assure the pattern and the reliability of the radiographic takings. The teleradiographs were obtained from Brazilian leucodermic boys and girls aged between 10 and 15 years who have never been submitted to orthodontic treatment before. Inside the dark room, the cephalograms were traced by one researcher only. The marking procedure involves the following materials: negatoscope with ultraphan paper of personalized size (17.5 cm x 17.5 cm and 0.07 in thickness), propelling pencil (0.3 mm lead), 0.5 mm-subdivided transparent rule, 0.1 degree protractor, template, and adhesive tape. The standard cephalograms were traced and the anatomic structures involving skull and face as well as the planes and lines of orientation were also delineated. The Frankfurt Horizontal Plane was used in this work as reference plane, being integral part of all the cephalometric measurements. This plane is located in the base of the cranium, being constituted by the porion point (anatomical or metallic) and the orbital point. The anatomical porion point (Figure 1) is located in the superior and posterior portions of the external auditory meatus. The metallic porion point (Figure 2) is located at 4.5 mm from the centre of the cefalostat’s metallic olive and the orbital point in the most inferior and posterior areas of the orbit. The angle measurements were performed for all cephalograms obtained from lateral cephalometric radiographs according to the both situations proposed: The cephalometric measures were compared between both groups (Figure 3): Occlusal Plane Angle (Downs, 1948)- Angle formed by FHP and Downs’ occlusal plane (intercuspidation of molars and incisors). Error AnalisysWith the purpose of evaluating the magnitude of the tracing error, all the thirty x-rays were traced three times at minimum interval of 10 days for each procedure so as the anatomical structures could not be memorized. Next, the mean arithmetic values of the three planes for each measurements were calculated according to the methodology proposed by Mitgard et al.15. Statistic TreatmentThe measures for FMA angle were considered non-normal according to the statistical analysis of the results by using Mann-Whitney’s test. The mean values for FMA angle are shown in Table 1, where statistically significant values at 1% (P<0,01) was found for the group using metallic porion marking. Statistically significant difference in the marking was also found between the groups according to the analysis of FMIA angle (P<0,05), thus revealing higher values for the anatomic porion group in relation to the metallic porion group (Table 1). Statistically significant difference between the samples was observed by the mean values for occlusal plane angle (P<0,01), where the mean value for metallic porion marking is higher than that for anatomic porion marking (Table 1). The radiographic cephalometrics is very useful for orthodontics, sometimes guiding both diagnoses and orthodontic treatment plan. Despite the great number of cephalometric analysis with their respective angles and values, certain cephalometric landmarks are marked in a standardized way. The anatomic porion point may not be easily visualized on many teleradiographs because of its location at the uppermost portion of the external auditory meatus. Such a difficulty is due to the density of the petrous temporal bone in addition to the projection juxtaposition of the corresponding right and left pyramids as well as the kilovoltage employed11. However, regardless of the lower visibility, if the porion is not directly visible it must be anatomically interpreted, that is, the porion is located at 8-10 mm with oblique plane of 45o, passing through their inferior homologue13. The Frankfurt horizontal plane (FHP) is reference for a great number of cephalometric measures. This plane is traced by joining both porion and orbital points, which along with other lines or planes, result in angles guiding the treatment plan during the analysis. The uppermost portion of the external auditory meatus is the correct place for marking the porion point, but in the face of the difficulty mentioned above, many ractitioners have been using the metallic porion point located at 4.5 mm from the centre of the cephalostatic image of the auricular olive12. Such a difference in the marking (anatomic or metallic porion) causes difficulties for standardizing and evaluating the results. Consequently, the way patient is treated may be significantly altered, mainly when the Tweed’s diagnostic facial triangle is used10. Statistically significant differences were found in this study when the values of cephalometric measures for FMA, FMIA and occlusal plane angles were compared in terms of anatomic or metallic porion point. The FMA angle indicating the facial type of the patient, according to Tweed10, had a mean value of 32.33o in the tracings using the metallic porion point, whereas those using the anatomic porion point had mean value of 27.57o. Such a difference of 4.76o was statistically significant and revealed facial patterns completely different. If we consider the patient, the value found in group 2 (metallic porion point) suggests a highly vertical pattern, whereas the value in group 1 (anatomic porion point) is nearly normal, thus characterizing the mesofacial aspect according to Tweed’s value (25o). Also, it was found that the mean values for FMIA angle were different. In the anatomic porion the mean value was 62.73o, whereas in the metallic porion group the mean value was 57.80o, thus characterizing the statistically significant difference between both groups. As this angle indicates the location of inferior incisor in relation to the Frankfurt horizontal plane, the first group shows the closest position to that predicted by the author (68o), whereas the second group shows a highly vestibular inclination of the incisor in relation to the reference plane. The occlusal plane angle corroborates the occlusal plane inclination (intercuspidation of molars and incisors) in relation to FHP, whose mean value is 10o. Concerning the cephalometric tracings, a statistically significant difference was found between the groups since the mean values for the anatomic and metallic porion tracings were, respectively, 6.23o and 10.77 o. The latter group has values closer to the normality, whereas the former indicates a low inclination of the occlusal plane. By analysing the cephalometric measures in order to describe the patient characteristics, the anatomic porion group showed mean values for FMA (27.56o), FMIA (62.73o), and FHP (6.23o), thus suggesting a vertical bias for facial pattern, close to normality, with labial inclination of the inferior incisor in relation to FHP and little inclination of the occlusal plane. In the metallic porion group, there was a highly vertical pattern (FMA -32.33o) with highly labial inclination of the inferior incisors in relation to FHP (FMIA - 57.80o), and proper inclination of the occlusal plane (occlusal plane angle - 0.77o). In the face of this measures, we would have distinct treatment plans for both groups because of the porion point variation. According to the analysis of the data and the results obtained we can conclude the following: 1 -The marking using cephalometric tracings (either anatomic or metallic porion point) alters the values for FMA, FMIA, and occlusal plane angles; References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}