 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Depth of occlusal caries assessed clinically by fluorescence laser, conventional and digital radiographic methods Luciane Zanin2 Marcelo de Castro Meneghim1 Andréa Videira Assaf2 Vanessa Pardi2 Antonio Carlos Pereira1 Fabio Luis Mialhe2 1DDS, MPH DrPH- -Department of Community Dentistry - FOP- UNICAMPPIRACICABA-SP-BRAZIL 2DDS, MPH, Department of Community Dentistry- FOP-UNICAMP-PIRACICABA-SPBRAZIL Correspondence to: Marcelo de Castro Meneghim Avenida Limeira 901 CEP:13414-903 Piracicaba, SP, Brazil E-mail: meneghim@fop.unicamp.br Received for publication: June 01, 2004 Code Number: os05016 Abstract The purpose of this study was to evaluate the performance of conventional radiographic, direct digital radiographic and the fluorescent laser in determining the extent of caries. The results suggested that the accuracy of the radiographic method was low for detecting enamel lesions and high for dentinal lesions. The fluorescent laser showed a high percentage of false positive decisions, although, this can be considered a good method for diagnosing initial lesions and dentists should adopt a preventive approach in these situations. Key Words:dental caries, diagnosis, methods, measurements IntroductionThe decline in the rate of caries progression has been reported worldwide over the past 20 years1-2. Caries reduction has been site dependent, with smooth surfaces showing the largest and occlusal surfaces the least reduction3. However, it has become increasingly difficult to detect caries lesions, especially on occlusal surfaces4-6. The effectiveness of visual examinations in diagnosing cavity lesions seems to be unquestionable; however, in recent years there has been concern about the difficulty of diagnosing lesions in the initial clinical stages5,7. The sensitivity of visual inspection can be improved when bite-wing radiographs are used. Consequently, the bitewing radiograph exam has been used considerably in dental practice and has shown that the association of this method significantly improves the accuracy of the diagnosis of fissure caries. Thus, it could be considered as a good auxiliary clinical method for making correct treatment decisions, since the presence of a dentinal lesion is a criterion for invasive procedures5. In recent years, a variety of digital imaging systems have become available in dentistry. Studies have been conducted with a view to effecting digital conversion of a conventional film radiograph. Conventional radiographs may provide insufficient density contrast. If the object contrast can be transformed systematically to enhance characteristics of diseased and healthy tissues, the lesion may become more perceptible to the human eye. The clinical advantages of this system include dose reduction due to increased sensitivity for X-radiation on the receptor; dose reduction due to fewer repeated examinations, as the digital system provides facilities for contrast and density manipulation and facilitates image transmission8. New techniques for caries detection and quantification have also been developed and investigated. A recent introduction is a laser-based instrument for detecting caries on both occlusal and smooth surfaces, KaVo DIAGNOdent (DIAGNOdent KaVo, Biberach, Germany)9. The main unit generates laser light with a 655nm wavelength, which is absorbed by both organic and inorganic material in the tooth and re-emitted as fluorescence within the infrared region. In the presence of caries the fluorescence increases and the changes are registered as increased digital numbers10. This device has shown to be sensitive in detecting initial decayed lesions, but it is important to note that calculus, plaque, composite filling materials, remnants of polishing pastes, and stains may produce fluorescence and, therefore, cause false-positive readings11. The purpose of this study was to evaluate the performance of conventional radiographic (bite-wing), direct digital radiographic and the fluorescent laser in determining the extent of caries after operative intervention, and to relate the clinical characteristics of the surface to the depth of the lesion. Material and MethodsThe material comprised a sample of one hundred fifty-three permanent molars of 6 to 8 year-old children with small occlusal lesion “microcavities”, characterized by small surface defects12. These lesions could either be associated or not with an active white spot lesion, characterized by the presence of an opaque, wrinkled, whitish surface with a chalk-like appearance13. Only one practicing dentist experienced in dental surveys carried out the investigation. The teeth were first selected, by visual inspection, using artificial light and a plane buccal mirror. Before the visual inspection, the occlusal surfaces were dried and cleaned using only a rotating bristle brush without prophylactic paste, due to the possible interference by the paste in the fluorescent laser evaluation11. Exclusion criteria: First permanent molars, sound, but not totally erupted;
showing clinical evidence of caries in dentin; sealed or fractured; showing signs of dental fluorosis or hypoplasias were excluded from the sample. The DIAGNOdent measurements were conducted following the instructions of the manufacturer. The instrument was calibrated once against the porcelain standard before the start of the study. The conical probe tip was positioned over a site on the drawing and slightly tilted while making a circular movement around the normal to the surface. DIAGNOdent measurements range from 0 to 99 representing a measure of fluorescence. The occlusal surfaces were measured 3 times and the highest value for each measurement was registered to represent the caries status of those surfaces11. Codes and criteria used for the exam with the fluorescence laser, DIAGNOdent® device. The bitewing radiographic examinations were obtained on E-speed film (KodaK Ektaspeed) with the aid of a film holder and the processing was automated. The direct digital examination was made and evaluated on a separate day, without knowledge of the previous exams. The radiographic appearance the surfaces, for both methods, were scored according to the criteria below. Codes and criteria used in bitewing radiographic and direct digital radiographic
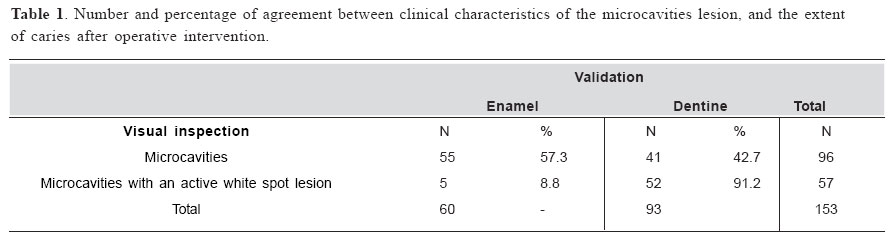
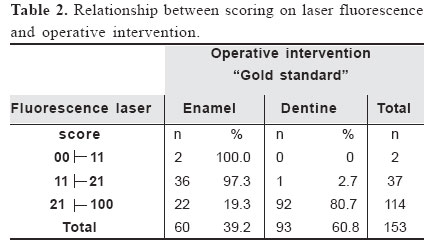
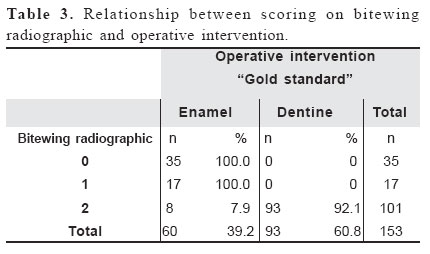
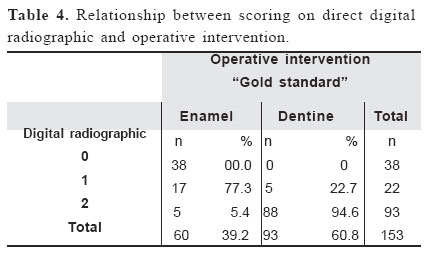
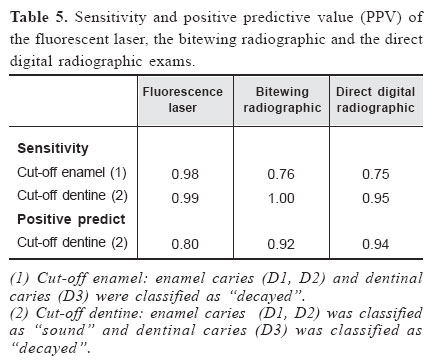
The caries tissue was removed stepwise using a diamond bur at low rotation exactly on the lesion previously analyzed by the visual inspection. After the removal of the decayed tissue, the depth of the lesion was evaluated visually and an explorer was used to verify if the decayed tissue had been removed11. After this, all lesions were recorded as enamel caries or dentinal caries. Afterwards the examiner restored the teeth. Statistical analyses Reproducibility. The examination procedure was repeated on a separate day to assess the reproducibility of the assessment. The quality of intra-examiner reproducibility was analyzed by Cohen’s Kappa statistic. This measure determines the overall level of agreement between observers while correcting for the proportion of agreement expected by chance. Kappa =1 represents perfect agreement, Kappa values above 0.75 denote excellent agreement, and those in the range 0.4-0.75 denote good agreement, while values below 0.4 denote marginal agreement14. Detection and Quantification. Sensitivity (defined as the ability to detect true disease correctly) and positive predictive value (PPV), (defined as the probability of the diseases being present when the diagnosis is positive), were calculated in relation to different cut-off levels: Cut-off enamel: enamel caries (D1, D1+D3) and dentinal caries (D3) were classified as “decayed”. Cut-off dentine: enamel caries (D1, D1+D3) was classified as “sound” dentinal caries (D3) was classified as “decayed”11. ResultsThe intra-examiner reproducibility expressed by Cohen’s Kappa coefficient was 0.86, 0.80, 0.89 respectively for the fluorescent laser, conventional radiographic and direct digital radiographic methods. The Table 1 shows that the determination of the extent of caries revealed enamel caries in 60 teeth (60.78%) and dentinal caries in 93 teeth (39.22%). Five lesions (8.8%), of the 57 microcavities associated with the white spot lesion, were in enamel and 52 lesions (91.2%) were in dentine. Of the 96 lesions that clinically presented microcavities without the presence of caries activity, 55 lesions (57.0%) were in enamel and 41 (43.0%) in dentine. By laser fluorescence, 114 teeth were assessed as having caries in dentine, 22 (19.3%) of these showed false positive decisions. Of the 37 enamel lesions, 36 were in enamel and only 1 tooth was assessed as having dentine caries (Table 2). By bitewing radiograph 101 teeth were deemed to have caries in dentine, 8 (7,9%) of which showed false positives decisions. There was total agreement with regard to the teeth diagnosed in enamel by the radiographic exam. Thirty-five teeth were assessed as smooth, but all lesions had false negatives decisions (Table 3). By direct digital radiograph 93 were assessed as having caries in dentine, 5 (5.4%) of which were false positives decisions. Twenty-two teeth were deemed to have caries in enamel, 5 (22.7%) of which were in dentinal. Thirty-eighty teeth were assessed as smooth, but all lesions had false negatives scorings (Table 4). The table 5 gives the performance of the diagnostic methods operative intervention. The fluorescent laser achieved a sensitivity of 0.99 (D3 level) and 0.98 (D1 +D3 level). The bitewing radiograph showed a sensitivity of 1.00 (D3 level) and 0.76 (D1+D3 level). Whereas, the direct digital radiograph gives a sensitivity of 0.95 (D3 level) and 0.75 (D1+D3 level). The positive predictive value (PPV) on D1+D3 level was not calculated due to the absence of smooth teeth in this sample. The positive predictive value (PPV) at D3 level was 0.80, 0.92 and 0.94 for the fluorescent laser, bitewing radiographic and direct digital radiographic exams respectively (Table 5). Table 6 gives the performance of fluorescent laser when the lesions were evaluated according to either the presence or absence of an active lesion. Fluorescent laser achieved a sensitivity of 0.78 (D3 level) and 0.67 (D1+D3 level). The positive predictive value (PPV) on D3 level was 0.66. Whereas, the sensitivity to active lesions was of 0.91 (D3 level) and 0.96 (D1+D3 level), and the direct digital radiograph gives a sensitivity of 0.95 (D3 level) and 0.75 (D1+D3 level), and the positive predictive value (PPV) at D3 level was 0.96. Discussion The fundamental basis of caries detection and quantification is the exploration of physical properties inherent to the lesion. In this study, observing the presence of a microcavity was not a safe criterion for the correct treatment decision, since 57.3% of these lesions were confined to enamel. Considering that preventive methods have been effective for deactivating initial lesions in enamel, an invasive procedure would result in over treatment in a large percentage of these cases. This data reinforces the idea that due to the great difficulty in making a correct diagnosis, the clinician feels the need to utilize other methods that increase the sensitivity of the visual method, thereby aiding the correct option for either preventative or restorative treatment to be determined. However, when the presence of a microcavities was associated with a spot white lesion, most of the lesions (91.2%) were confined to dentine and 8.8% were in enamel after validation. In these cases, the presence of a spot white lesion, characterizing caries activity, was a decisive criterion for carrying out invasive procedure, as the presence of a lesion in dentin was found. Therefore, in case of doubt in relation to the diagnosis and given the impossibility of using auxiliary resources, only the discerning observation of the lesion’s clinical characteristics can indicate the need for invasive procedures with low risk of over-treatment. The choice of treatment is based on the diagnosis15, and the accuracy of that diagnosis is very important. A restorative approach is justified when an occlusal caries has reached the dentin, because it seems to be a general opinion that dentinal caries should be treated operatively, it is important to know the amount of dentin involved in an occlusal carious lesion without visible clinical cavitations16. Checking the sensitivity values and positive prediction in different cut-offs is justified because according to the criteria used to characterize “disease” the sensitivity values and PPV can vary considerably. Different diagnostic methods have been developed and tested in an attempt to overcome the difficulties encountered by dentists in their clinical practice. The bitewing radiographic exam has been used considerably in dental practice and has shown excellent results in the correct diagnosis of dentinal lesions and for monitoring preventive therapy17. Therefore bitewing radiographic is inaccurate in detecting minimal occlusal lesions. In this study the bitewing radiographic exam as well as the direct digital radiographic exam showed high sensitivity in diagnosing D3 level lesions, these results are in agreement with others studies5,15,18. However they did not show satisfactory results at D1+D3 level, showing a high percentage of false-negative decisions and leading to an underestimation of the disease. Direct digital radiographic methods have also been used in clinical practice and have shown advantages such as, a significant decrease in the patient’s exposure to radiation, the possibility of manipulating the image, eliminating radiographic processing and the decrease in storage space, since the images can be saved in computer files19. The excellent reproducibility of results indicates that the DIAGNOdent may be of value for longitudinal observation of carious sites. Some studies show that the fluorescent laser shows high sensitivity values and specificity6,11,20. The DIAGNOdent was extremely sensitive to any alteration in the enamel structure, so that the sensitivity value at D1+D3 level was 0.99, showing good capacity in identifying the disease correctly. A high value of positive prediction was verified as well, also demonstrating the excellent reliability of the method in making correct positive diagnoses. More attention should be given in relation to the lesions at D3 level. In these cases, the sensitivity value remained high due to the capacity of the method for identifying any structural alterations; however, it showed the lowest positive prediction value for this level, due to a considerable number of false-positive diagnoses. This aspect previously discussed by Lussi et al., (2001), probably occurs due to the presence of pigmented ridges, which interfere in the measurement by the device, leading to an increase in the reading. Therefore, it is possible to reduce the percentage of diagnostic mistakes when the clinical aspects of the lesion are considered in the treatment decision. However, when the lesions were analyzed separately in relation to the presence and absence of active lesions, the percentage of false-positive results by fluorescent laser decreased from 33.4% to 3.7%. This finding supports the proposal that DIAGNOdent readings reflect changes in organic material rather than the inorganic content of tooth substance10,21-22. Thus, the presence of a single microcavity in the occlusal surface cannot be considered to be a clinical criterion for opening the cavity. It is necessary to use auxiliary methods in order to improve the diagnosis. The association of the microcavity with an active spot white lesion can be considered as a shaping clinical criterion for the verification of dentinal lesions. The bitewing radiographic and direct digital radiographic methods showed unsatisfactory performance for diagnosing caries in enamel but offered excellent results for lesions in dentin. Therefore, they could be measured as being excellent auxiliary methods in the treatment decision. Fluorescent laser demonstrated excellent results in diagnosing initial decayed lesions. However, due to the percentage of false-positives, it should not be the only method used when deciding whether to use invasive or non-invasive treatment. It should be associated with the visual method and/or other diagnostic methods to reduce the possibility of making incorrect treatment decisions. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil | ||||||||||||||||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}