 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 4, No. 13, April./June. 2005, pp. 741-744 Risk factors of laryngeal cancer in patients attended in the oral oncology center of Araçatuba Marcelo Coelho Goiato1 Aline Úrsula Rocha Fernandes1 1Maxillofacial Prosthesis area of the Oral Oncology Center from the Dentistry School – UNESP, Araçatuba.– SP – Brasil. Correspondence to: Marcelo Coelho Goiato Faculdade de Odontologia de Araçatuba – UNESP Depto. de Materiais Odontológicos e Prótese Rua José Bonifácio 1193 – Vila Mendonça, CEP 16050-050 Araçatuba – SP – Brasil Phone an Fax: +55-18-3636-3245 E-mail: goiato@foa.unesp.br
Received for publication: October 19, 2004 Code Number: os05017 Abstract The laryngeal cancer is the second most common respiratory cancer worldwide. The aim of this study is to perform a survey on data related to the incidence of laryngeal cancer that would enable its analysis among patients with larynx cancer attended at the Oral Oncology Center from the Dentistry School - UNESP, Araçatuba-SP-BR. Out of the 66 cases of cancer registered at the Oncologic Treatment Center between 1991 and 2003, 64 cases were identified in men. Information of gender, age, race, tobacco and alcohol use and occupational history were obtained from patients through a standardized questionnaire. The largest number of cases of laryngeal cancer occurred among farmers, building constructions workers and drivers. The incidence was higher among smokers, white individuals with ages ranging from 50 to 60 years. In conclusion, the risk of laryngeal cancer was associated to several factors, also occurring due to the effect of the socio-economic status, diet, income and educational level. Key Words:laryngectomy, incidence, laryngeal cancer, larynx. Introduction
The laryngeal cancer treatment was considered as complicated until the 19th century, mainly due to the fact that despite ancient physicians had already known about the occurrence of tumors; a larynx examination technique had not been yet developed until the middle of that century. Before that, there were a countless advances on the larynx anatomy and surgery1. Cohen2, in the year of 1883 published a series of 63 laryngectomies; however, one third of the patients died before accomplishing one month of surgery. Advances on anesthesia, pre and post-operative cares, antibiotics development and the care with surgical instruments handling became possible; a correct patients selection with the objective that most of them would survive from surgery1. The laryngeal cancer is the second most common respiratory cancer worldwide, following the lung cancer3. The world incidence was in the ratio of 5,69 in 19994. The laryngeal cancer is widely related to the tobacco and alcohol use5, however, occupational and environmental factors also contribute6. Substances such as nickel, solvents, inks and oils have also been related7. Differences in the life style, labor conditions and occupational expositions may also affect the individual. The incidence of laryngeal cancer is generally low, presenting remarkable exceptions including Brazil, France, Italy, Spain, India and southern Asia8-9. Among women, the highest indexes are low, if compared to indexes found in men, according to the several populational groups1. The laryngeal cancer levels among occupational groups may be explained through the effect of the socio-economic status7. Patients submitted to total laryngectomy have as result from surgical resection the complete phonation loss and the transfer of the airways function to the tracheostomal neck opening10. There are techniques developed for the manufacturing of a tracheostoma aesthetic prosthesis from the molding and manufacturing of a acrylic resin tube in order to protect the stoma, the stomal mucosa and the neighboring tissues, to filter the air and to promote the aesthetics11. The quality of life of patients is improved and, as result, patients feel more comfortable about their social life. The objective of this study is to perform a survey on data related to the incidence of laryngeal cancer that would enable its analysis among patients with larynx cancer attended at the Oral Oncology Center from the Dentistry School - UNESP, Araçatuba, at the period from 1991 to 2003. Material and Methods
This study was approved for the IRB for Human Studies of UNESP, Process FOA 870/ 2003. Material
Human Material: Laryngectomized patients registered on the Oral Oncology Center from the São Paulo State University UNESP, Araçatuba Campus in the period from 1991 to 2003. 66 patients were selected from both genders with ages ranging from 37 to 83 years. Technical Material: data collecting filling cards containing the patient identification and factors that might be related to the disease etiology.
Methods
The methodology consisted of the filling of the data-collecting card and of the quantitative survey of the information collected. Filling of the data-collecting card: the information regarding the patient identification and the laryngectomy reason were given by the own patient or by the responsible. The ages were grouped into 6 groups: less than 40 years of age, from 40 to 49 years of age, from 50 to 59 years of age, from 60 to 69 years of age, from 70 to 79 years of age and above 80 years of age. After the filling of the data-collecting card, the results obtained were analyzed through averages in percentage and illustrated with the aid of tables. Results and Discussion
The results obtained from the data quantitative survey for the variables proposed are presented and discussed below. 1. Gender, age and race
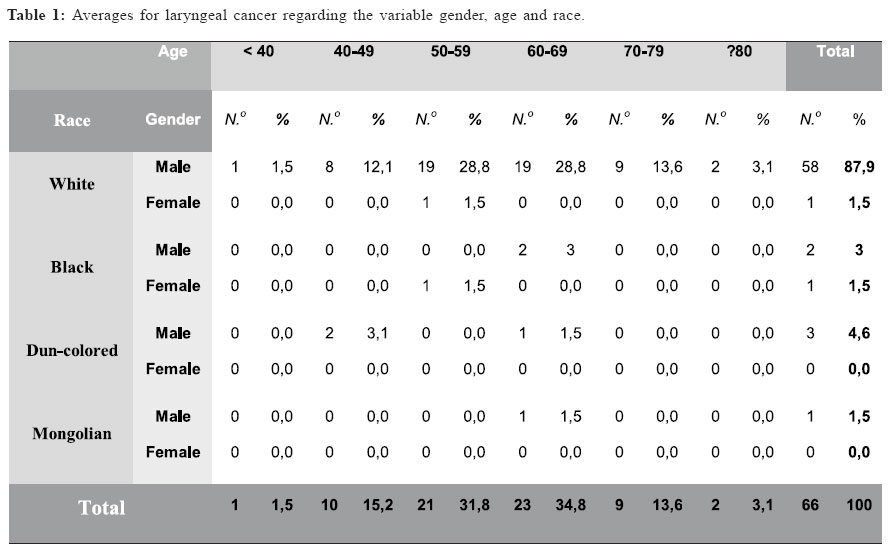
The Table 1 shows the percentage values found for the variables gender, age and race. The gender male represents 97% of cases. The finding can be related to the larger number of men exposed to environmental factors and smoking habits and alcohol use precedings, however, Kruk-Zagajewska et al.12 reported that such divergence may be also explained by endogen factors, through sexual hormones. In a preceding study, 67 patients submitted to larynx cancer surgery were assessed for values of estradiol, progesterone and cortisol binding to globulin in the blood serum. High values of estradiol and cortisol binding to globulin were observed, while normal values of progesterone were found in a significant number of patients. Crocetti & Paci13 evaluated the differences of incidence occurred between male and females with regard to the modifications of exposition to carcinogenic substances observed during two different decades, 1980 and 1990, in central Italy. They observed that among the younger subjects, a reduction on the larynx cancer incidence was observed with the reduction on the prevalence of smokers among men and increase among women. The prevalence differences found between periods of time within the same region or between different regions may be explained by the differences found with regard to the exposition of populational groups to risk factors of laryngeal cancer. The age range of highest incidence of laryngeal cancer was between 50 and 69 years of age, holding 53% of cases. The values found corroborate with the findings of Maier & Tisch14, when studied the population of Heidelberg, in Germany. Muscat & Wynder15, in 1995, conducted a study in New York and asserted that the predominating age group is found above the 40 years of age. Young patients seem to be exempted maybe because the fact that the carcinoma is a multi-factorial disease, originated from the chronic exposition to risk factors. White individuals prevail with 88% of cases, followed by black and dun-colored individuals, both wit 5% each. Rafferty et al.1 mentioned in his article that the highest incidence in all races has been observed among black individuals, when the black population in the United States and the populations of India, Anglo-Saxon and France were studied. Our study was carried in a region in which the predominant ethnic group is white, what could explain the high incidence among white individuals. The variable race was not yet directly related to the risk factors of laryngeal cancer. 2. Precedings and profession
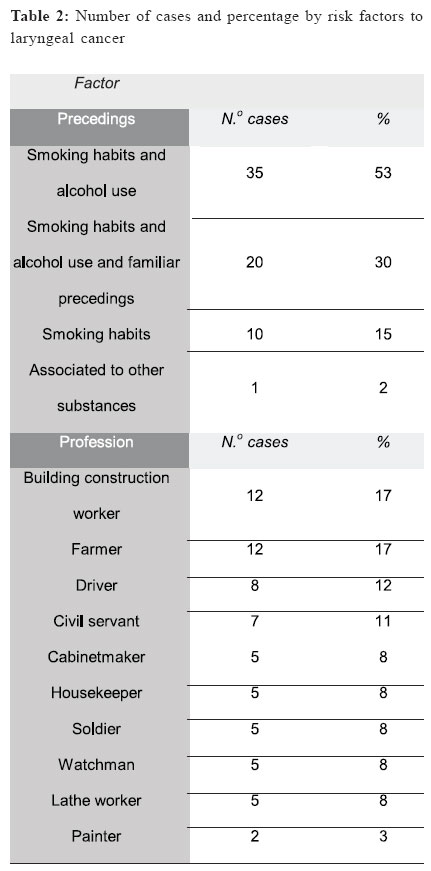
The Table 2 shows the percentage values found for the variables precedings and profession. The smoking habit and alcohol use prevail with 53%, compared to the other cancer risk factors. The tobacco smoking and the alcohol use are the highest risk factors established for laryngeal cancer. Tuyns et al.16 asserted that the risk decreases in less than 10 years after smoking halt and that the association of the smoking habit with the alcohol use promotes a multiplicative relative risk to laryngeal cancer. Rafferty et al.1 mentioned a finding in the southern of Europe in which the reduction on the alcohol use only would prevent one fourth of the larynx carcinoma cases. The laryngeal cancer is less strongly associated to the alcohol use and more strongly associated to the tobacco smoking than the oral cavity and esophagus cancers16. When the excessive alcohol ingestion is associated to the smoking habit, the risk is increased for supra-glottis cancer. Patients with larynx cancer who still smoke and drink have decreased cure possibilities and increased risk of appearance of a second tumor at the head and neck regions17. From those patients who informed the profession, 17% were farmers and building construction workers, followed by drivers, with 12% and civil servants, with 11%. A study carried out in Turkey related the occupation conditions with larynx cancer risk factors, finding higher risk factors among watchmen, production supervisors, textile workers, drivers and building construction workers7. According to Elci et al.7, the deficits of larynx cancers between occupational groups such as managers and directors, may be due to the effect of the socio-economic status and reflects the impact of diet, income and educational level. Based on the results obtained, one may conclude that the laryngeal cancer is multi-factorial, being influenced by gender, age and exposition to agents such as tobacco and alcohol associated to the individuals’ socio-economic status and occupation. The laryngeal cancer is dependent on time and on the exposition to risk factors. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}