 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 4, No. 13, April./June. 2005, pp. 745-748 Extensive gas-forming infection of thedeep neck and laryngeal spaces Ashwani Sethi1 Deepika Sareen2 Sumit Mrig3 A.K.Agarwal4
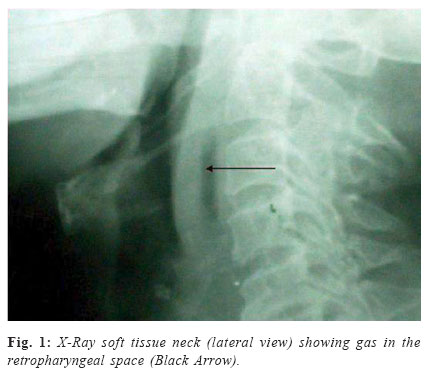
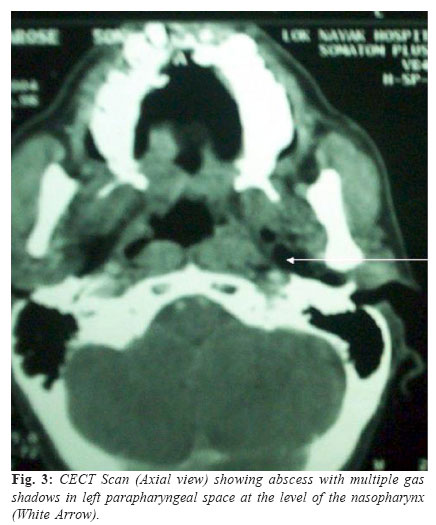
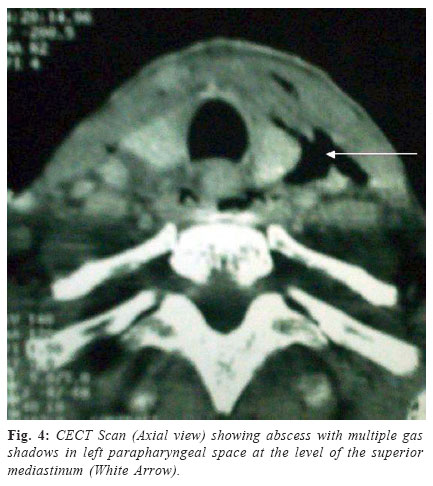
Received for publication: February 24,2005 Code Number: os05018 Abstract We report the case of a 46-year-old diabetic male who presented to us with swelling in the neck associated with dysphagia and respiratory discomfort following dental infection. The CT-scan and soft tissue neck radiograms of the patient revealed an extensive head and neck abscess with gas pockets. Prompt surgical intervention with antibiotic coverage and control of diabetes led to recovery of the patient. The absence in the literature of any previous report of a laryngeal gasforming abscess resulting from a primary dental infection prompted us to report this case. Key Words: parapharyngeal space; retropharyngeal space; paraglottic space; preepiglottic space; gas-forming infection; odontogenic. Introduction Extensive head and neck infections caused by gas-forming organisms are rare with a very few cases reported in the past1-2. Most of these infections arise as a result of mixed aerobic and anaerobic organisms3. Involvement of the paraglottic space with an infectious process is rare and may result as an extension of a supraglottic infection4. In our search of medical literature, we have not identified any case of a paraglottic space infection of odontogenic origin caused by gas-forming organisms. Case ReportA 46-year-old diabetic male presented to us with a rapidly progressive, diffuse, painful neck swelling originating below the jaw, difficulty in swallowing and labored breathing of three days duration. The patient also had pain in the right lower molar teeth for the past one week. There was no history of trauma. On examination, the patient was febrile, had tachycardia and was dyspnoeic with intermittent stridor. Neck examination revealed cellulitis involving the submental, left submandibular and bilateral paralaryngeal and paratracheal regions. There was no cervical lymphadenopathy. Per oral examination revealed poor orodental hygiene with halitosis, and caries involving the right lower first and second molars. There was no obvious parapharyngeal or retropharyngeal bulge, however, the floor of mouth was found to be raised. Indirect laryngoscopic assessment revealed pooling of secretions in bilateral pyriform sinuses with restricted mobility of both the true vocal cords. The routine biochemical and hematological investigations were within normal limits except for raised blood glucose levels. ELISA for HIV was non-reactive. Urine analysis was within normal limits. A soft tissue radiogram of the neck was done, which showed an increase in the soft tissue opacity of the retropharyngeal space with air shadows anterior to the laryngeal framework and within the retropharyngeal space (Figure 1). The chest X-ray of the patient was normal with no evidence of mediastinitis. A contrast enhanced CT-scan from the base of skull to the clavicle was done, which revealed an abscess involving the retropharyngeal space, pre-epiglottic and bilateral paraglottic spaces (Figure 2), and the left parapharyngeal space extending from the level of the nasopharynx above till the level of superior mediastinum below (Figures 3 and 4). Multiple air shadows could be seen in the anterior neck, parapharyngeal and paraglottic spaces (Figures 2, 3 and 4). The patient was tracheostomized and the left parapharyngeal, retropharyngeal and anterior neck spaces were drained through a transverse neck incision along the superior border of hyoid bone. Around 60-70 ml of extremely foul smelling pus was drained and sent for aerobic and anaerobic cultures. The patient was put on intravenous antibiotics in the form of crystalline penicillin, gentamycin and metronidazole. The pus culture revealed Staphylococcus aureus, Klebsiella pneumoniae and anaerobic Streptococci. Later, injection levofloxacin was added to the antibiotic regime on the basis of the culture sensitivity. The diabetic status was managed with injection insulin in consultation with the endocrinologists. The patient recovered completely and was discharged after three weeks of his admission. The patient was referred to the dental department for management of caries. Six months following the follow up, the patient is asymptomatic for the disease. DiscussionThe present case is an extremely interesting one as almost all the possible deep neck compartments along with laryngeal spaces were involved by a gas-forming infection. The primary focus of infection in this patient appears to be the lower first and second molars on the right side, which were found to be infected on examination. Infact, dental infections, along with tonsillar infections, are the most common primary foci for deep neck space infections5. The teeth most commonly involved are the second and third molars, although, canines have also been reported as the primary infective foci6. Like most of the other infections, the immunocompromised individuals such as diabetic patients are more susceptible to deep neck space infections with a more severe clinical course, increased risk of life-threatening infections and a poorer prognosis7. Our patient was also diabetic. Our patient presented with a diffuse neck swelling originating in the submental region. The history is suggestive of the development of a Ludwig’s angina with spread into the parapharyngel, retropharyngeal, pre-epiglottic and paraglottic spaces. Since Ludwig’s angina is an infection of the midline neck spaces (i.e. submaxillary and sublingual spaces), the infectious process may extend into the submandibular triangles on either side of the neck from these spaces. In the present case, the infectious process apparently extended onto the left submandibular region in the form of an abscess even though the primary focus of infection i.e. the carried teeth were in the right lower jaw. The extension of the submandibular space infections into the parapharyngeal and retropharyngeal spaces is a known entity8. Since, no case of pre-epiglottic and paraglottic space infection in association with deep neck spaces has been reported in the past, the precise mechanism of involvement of these, essentially laryngeal spaces, in conjunction with deep neck spaces has not been discussed in the past. We propose two possible mechanisms of involvement of these laryngeal spaces. The anterior neck cellulitis in the patient may spread through the thyrohyoid membrane to involve the pre-epiglottic space with consequent involvement of the paraglottic spaces. The other proposed mechanism is a direct extension into the paraglottic space of the infective process lying lateral to the pyriform sinus. The involvement of the paraglottic space was indicated by a restriction of the vocal cord mobility on the indirect laryngoscopic assessment, although, the definitive diagnosis was established only after the CT-scan. Prompt surgical intervention with drainage of the abscess was the most essential part of the management and we consider it to be a life-saving step in the present case. Frequently, patients with such an extensive neck infection may present with airway compromise. In such patients, the management of airway takes priority as regards the management. Fortunately, our patient never had any airway compromise during the coarse of management. The pus culture in the present case revealed a mixed aerobic and anaerobic flora with gas-forming organisms (i.e. Klebsiella, anaerobic streptococci). The other gas-forming organisms isolated from the head and neck infections reported in the past are Clostridium6, Bacteroides, Fusobacterium9, etc. Through this report, we attempt to highlight an extremely unusual presentation of a patient with extensive infection of the deep spaces of the neck and larynx caused by gas-forming organisms. We intend to reemphasize early recognition and treatment of dental infections with prompt surgical intervention for life-threatening head and neck infections. Learning points:(1). Dental infections may extend rapidly to involve deep neck and laryngeal spaces producing life-threatening situations.
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}