 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 4, No. 13, April./June. 2005, pp. 749-752 Histopathology and ultrastructuralfeatures in mucous extravasation phenomenon: Report of a case Shareef, B. T. Al- Salihi, K. A. Samsudin, A. R. Pohchi, A Universiti Sains Malaysia School of Dental sciences Kubang Kerian, Kelantan Malaysia Correspondence to: Al- Salihi Universiti Sains Malaysia School of Dental sciences Kubang Kerian, Kelantan Malaysia E-mail: elsalihi@yahoo.com Received for publication: February 14, 2005 Code Number: os05019 Abstract Histopathological and ultrastructural features of a case of pseudocyst extravastation mucocele lesion located in the lower lip of an 18 yearold Malaysian female is presented. Complete surgical excision of the lesion with associated minor salivary glands was done. The specimen was processed for routine histopathology and transmission electron microscopy (TEM) for ultrastructral studies. The lesion revealed pooling of mucin infiltrated with inflammatory cells and walled by a rim of granulation tissue. The underlying salivary lobules showed varying degrees of chronic sclerosing sialadenitis. Ultrastructural features revealed multiple membrane bound electron lucent mucus granules with varying diameter, duct cells with few microvilli. Desmosomes, tonofilaments and myoepithelial cells were prominent. There were also dilatation of the rough endoplasmic reticulum (RER) and presence of multiple electron dense granules Key Words: extravasation mucocele, mucin, TEM, ultrastructural, contractile filaments Introduction Mucocele and ranula are clinical terms for a pseudocyst that is associated with mucus extravasation into the surrounding soft tissues. These lesions occur as the result of trauma to the salivary gland excretory duct, although obstruction of salivary flow is implicated in some instances1-2. A mucocele may persist for as long as a year without rupturing, but many patients present within a few weeks of onset for evaluation3. Recent research studies have revealed increased levels of matrix metalloproteins, tumor necrosis factor-alpha, type IV collagenase, and plasminogen activators in mucoceles compared with that of whole saliva. These factors are further hypothesized to enhance the accumulation of proteolytic enzymes that are responsible for the invasive character of extravasated mucus4. Mucoceles occur commonly in the oral cavity, typically on the lower lip but may present anywhere the minor salivary glands are found, including the floor of the mouth, tongue and palate, while the term mucocele has been applied only infrequently to lesions of the upper lip5-6. Almost two third of mucoceles appear to be more common in the first three decades of life; both sex are equally affected. Clinically, superficial mucoceles appear as thin-walled, bluish lesions that rupture easily; deeper lesions are well-circumscribed swellings covered by normal appearing mucosa. There are two types of mucoceles which are mucus-extrvasation and mucus- retention. The former type is more common and caused by laceration of a minor salivary gland duct by trauma, resulting in transaction of the duct and leakage of saliva into submucosal tissue with subsequent inflammation and formation of granulation tissue7-9. Chronic sclerosing sialadenitis is chronic inflammatory response of salivary gland tissue; it may occur as result of obstruction or severance of minor salivary gland ducts in addition to other factors. Microscopically the ductal elements are often seen to remain whereas the acini are completely degenerated8,10. In a review of the medical literature, the mucus-extravasations and mucus- retention are more common cases, the histological findings have been well described however,no published article have been found regarding the ultrastructural features of mucocele. Therefore, this paper presented the histopathological and ultrastructural features of a case of extravasation mucocele associated with chronic sclerosing sialadenititis located in the lower lip of an 18 year-old Malaysian female. Case Report
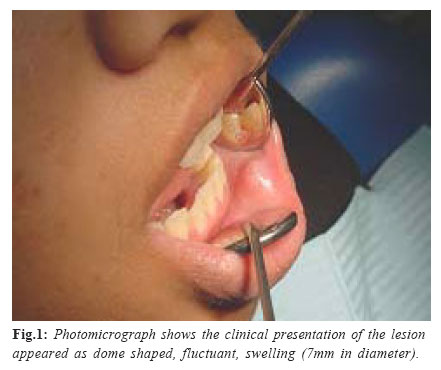
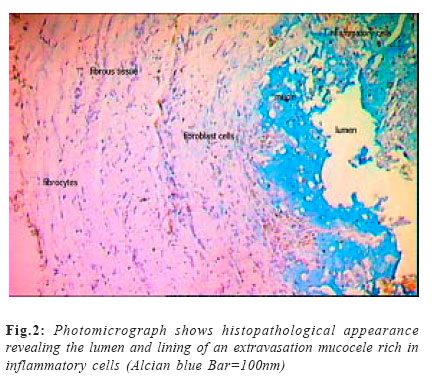
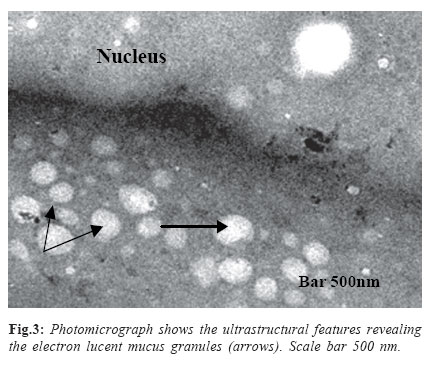
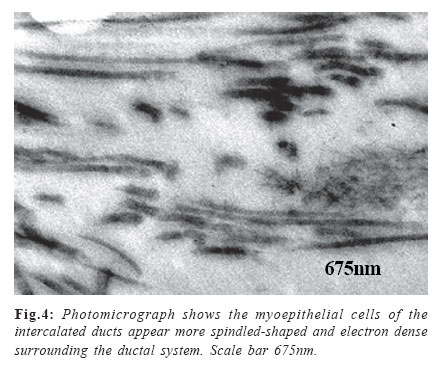
An 18 year-old Malaysian female presented to USM out-patient dental clinic complaining of uncomfortable painless swelling in the inner side of the left lower lip. The lesion showed dome shaped, fluctuant, swelling (7mm in diameter) (Fig.1). Excisional biopsy with associated minor salivary glands was performed, and the wound was closed with 4-0 sutures (gut for deep closure and silk super-facially). A mucocele was suspected. The biopsy sample was cut into two parts first part, immediately fixed in 10% neutral buffered formalin for routine histological evaluation and stained with haematoxylin & eosin while other sections were stained with special Alcian blue stain a useful in identifying mucin that is free in the tissue or in the foamy macrophages. The second part was preserved in cacodylate-buffered glutaraldehyde 2.5 % and cut into 1mm3 blocks for ultra structural study. The specimen was first pre-fixed in glutaraldehyde at 4 oC for 12 hours. Post-fixed for 2 hours in osmium tetroxide, and then dehydrate and embedded in Epon. Ultrathin sections were cut and stained with uranyl acetate followed by lead citrate. The specimen was examined with TEM (LEO 9122 AB, Germany ). The histological sections revealed distended surface epithelium due to pooling of mucin. The mucin appeared as blue color pool walled by a rim of granulation tissue and collagen. Infiltrations of inflammatory cells were appeared in the mucin pool as well as in the granulation tissue wall (Fig.2). The underlying salivary lobules were showed varying degrees of chronic sclerosing sialadenititis which was characterized by extensive acinar degeneration with fibrosis and infiltration of inflammatory cells with widening of ductal system. The definitive diagnosis was mucocele of the left lower lip. No recurrence was observed at 1-month and 4-month follow-up examinations. Ultra structural features revealed multiple membrane bound electron lucent mucus granules with varying diameter (Fig.3) and duct cells with few microvilli. Collagen fibril was appeared as spiral shaped, electron dense surrounding the ductal system . There were also dilatation of the rough endoplasmic reticulum (RER) and presence of multiple electron dense granules. The desmosomes, tonofilaments, myoepithelial cells and secretory cells were prominent and aggregated to form dark bodies. Myofilaments cell process was proliferate and contained many contractile filaments and densities (Fig.4). The myoepithelial cells of the intercalated ducts are more compressed and spindled-shaped with fewer processes. Discussion The mucocele arises most frequently on the labial mucosa of the lower lip although such a lesion can occur any where in the oral mucosa3,5-6. This lesion has also been called a mucus extravasation phenomenon while mucus- retention cyst is usually found on palate or floor of the mouth9,11. Traumatic severance of the salivary gland duct, such as that observed by biting the lip or buccal mucosa, precedes the development of the mucocele. Mucocele are usually formed secondary to rupture of an excretory duct of a salivary gland, which leads to an outpouring of saliva into the surrounding tissues11. The resulting pool of glandular secretion is first surrounded by inflammatory cells and later by reactive granulation tissue consisting of fibroblasts. This granulation tissue reflects an immune response (i.e., to wall off the mucin). Although there is no epithelial lining surrounding the mucin, it becomes well encapsulated by this granulation tissue and is therefore categorized as a false cyst or pseudocyst. The clinical presentation and histopathological features of a lesion in the case reported here was diagnosed as a mucocele of the left lower lip and typically compatible with the other extravasation mucocele cases described by other researcher2-3,9. Others histopathological features were the extensive acinar degeneration with fibrosis and infiltration of inflammatory cells with widening of ductal system. This lesions was resulted from salivary obstruction evolves and as glandular secretions accumulate within the ductal lumen, backpressure changes evolve leading to acinar atrophic degeneration. As acinar cells progressively degenerate subsequent to obstruction, apoptosis and necrosis ensue. Once acine are no longer evident, the parenchyma undergoes a progressive fibrosis (sclerosis), a process common to all reactive lesions. In the salivary glands it is referred to as chronic sclerosing sialadentis8. The ultrastructural features of mucocele were described for the first time in this paper. For the author’s knowledge and from the medical journal review, mucocele ultrastructural haven’t been described previously. The ultrastructural features support the histopathological features of mucocele, and can contribute in understanding the pathogenesis of mucocele. There were prominent desmosomes, tonofilaments, myoepithelial cells, secretory cells and myofilaments, which were aggregated to form dark bodies. The functions of myoepithelial cells are to support secretory cells and contract and widen the diameter of the intercalated ducts12. In the ultrastuctural level the increasing number of the contractile myoepithelial cell of the intercalated ducts in this mucocele case, which appeared more compressed and spindled-shaped with fewer processes and contained many dense contractile filaments may aid in the rupture of acinar cells of epithelial origin and leads to escape of secretion into the surrounding tissue. The treatment of choice for lips mucocele is local excision with extirpation of the underlying lobules of minor salivary gland tissue. Failure to remove the glandular tissue may contribute to recurrence. Cohen and others, 196513 observed that, of 63 mucoceles, 82% were found on the lower lip, 8% on the buccal mucosa, 3% on the retromolar area, and 1% on the palate. The Armed Forces Institute of Pathology collected data on 2,339 cases of mucocele and found that 33.0% Occurred on the lower lip, 7.7% on the buccal mucosa, 6.3% on the floor of the mouth, 6.1% on the tongue and only 0.4% on the upper lip14. It is of interest that the mucocele is restricted almost exclusively to the labial mucosa of the lower lip15 and is seldom, if ever, observed involving the upper lip3 . Conversely, salivary gland neoplasms are for the most part confined to the upper lip and only rarely occur on the lower lip. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}