 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
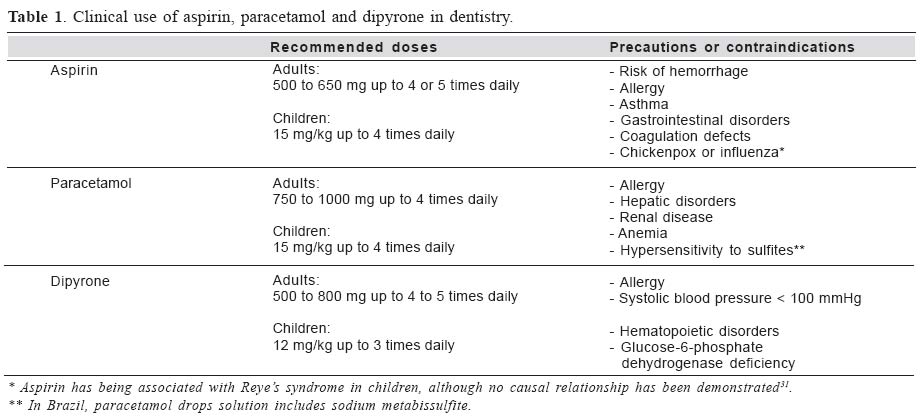
Brazilian Journal of Oral Sciences, Vol. 4, No. 14, July/Sept. 2005, pp. 762-765 Analgesic choice in dentistry.Part I: The mechanism of action Filipe Polese Branco 1* Marcos Luciano Pimenta Pinheiro 2** Maria Cristina Volpato 3* Eduardo Dias de Andrade3* 1DDS, MS 2PharmD, MS 3 DDS, PhD *Science Physiological Department, PiracicabaDental School, Campinas State University,Piracicaba-SP, Brazil.**Diamantina Dental School, Diamantina, Brazil. Correspondence to: Eduardo Dias de Andrade Department of Physiological Sciences Piracicaba Dental School Campinas State University Av. Limeira, 901 13414-903 Piracicaba-SP, Brazil E-mail: eandrade@fop.unicamp.br Received for publication: April 15, 2005 Code Number: os05023 Abstract Analgesics are frequently used in dentistry for the management of dental pain. Dental clinicians should choose the medicine based on its mechanism of action and toxicity, to promote a successful analgesic effect as well as comfort to the patient. The purpose of this first article is to describe the pharmacological mechanisms of action of the three analgesics considered for the management of mild to moderate acute dental pain. Key Words: analgesics, mechanism of action, dentistry IntroductionAnalgesics are commonly recommended for mild, moderate or acute pain. About 16 million of these drugs are annually prescribed by American dentists. In Brazil, analgesics are the most sold out class of medicine; dipyrone is the first in this list followed by acetaminophen (paracetamol) and aspirin, respectively. Although these drugs are safe, recent studies alert to intoxication risk and severe adverse effects, even at doses or concentrations nearly the same as those used to relieve pain, increasing the need for either pharmacological knowledge or patient guidance. The clinician should employ a variety of effective and safe analgesic regimens based on estimates of anticipated pain intensity, mechanism of action and toxicity1. The purpose of this first article was to describe the pharmacological mechanisms of action of three analgesics considered for the management of mild to moderate acute dental pain in dentistry as well as parameters to choose each of them. AspirinAspirin has been used in dentistry as an anti-inflammatory, analgesic and antipyretic drug prescribed for use within short periods2. The mechanism of action of aspirin, a nonsteroidal anti-inflammatory drug (NSAID), was established approximately 30 years ago3. Clinical trials have shown repeatedly that aspirin is effective in the management of dental pain4. Optimal use of this drug is based on the understanding of its action on the arachidonic acid metabolism pathways. Aspirin blocks the cyclooxygenase enzymes, which exist in at least two known isoforms: cyclooxygenase 1 (COX-1) and cyclooxygenase 2 (COX-2). COX-1 is responsible for the synthesis of several mediators, including the prostaglandins that protect the gastric mucosa and regule renal blood flow, and the thromboxanes, which initiate platelet aggregation5. Tissue damage resulting from pulpits, periodontitis, or oral surgery will induce the production of COX-2, which, in turn, leads to the synthesis of the prostaglandins that sensitize pain fibers and promote inflammation. Traditional NSAIDs, such as aspirin, act by blocking both cyclooxygenase enzymes (COX-1 and COX-2). This nonselective inhibition is responsible for many of the unwanted effects of this drug6. Aspirin, like all the other NSAIDs, induce inhibition of thromboxane synthesis resulting in a decrease in the platelet aggregation. For most NSAIDs this effect is reversible within 24 hours; however, aspirin is unique in that it irreversibly damages cyclooxygenase for the life of the platelet5. Although an increase in the time of coagulation can be accepted in normal patients, aspirin might promote post-operative hemorrhage, mainly if the clot is not totally formed. There are some reports of hemorrhage after aspirin ingestion in dentistry7-8. Use of aspirin in children during or immediately after a viral infection has been associated with the increase in the incidence of Reye’s syndrome9. This syndrome is a rare acute encephalopathy associated with fatty degeneration of the liver and its etiology remains uncertain. It is known to occur after viral infections such as chickenpox (varicella) and influenza10. Table 1 shows the clinical use of aspirin in dentistry. ParacetamolParacetamol has become increasingly popular as a safe and mild aspirin substitute, either alone or in associations, without decreasing in the platelet aggregation. It is currently found in more than 200 formulations, most of which are available over the counter. It is often categorized as a NSAID even though it provides little anti-inflammatory activity in clinical practice and in animal models11. The exact site and mechanism of action of paracetamol remain unclear. Flower et al.12 reported that paracetamol might produce analgesia by increasing pain threshold. Björkman et al.13 suggested that the potential mechanism of action might involve the inhibition of the nitric oxide pathway and is mediated by several neurotransmitters, including the Nmetil-D-aspartate and the P substance. Actually, this discussion focuses on the relation between paracetamol and the isoforms of COX. Flower and Vane14 showed that paracetamol inhibited COX activity in dog brain homogenates more than in homogenates from spleen, suggesting the existence of different isoforms of COX. The great step forward in our understanding of the NSAIDs came in the early 1990s whem the existence of two isoforms of COX was proved on a molecular basis, COX-1, constitutively expressed, and COX-2, inducible by pro-inflammatory stimuli15. However, not all questions were answered by the characterization of two COX enzymes originating from different genes. One such question is the effect of paracetamol, which, unlike NSAIDs, produce analgesia and antipyresis but has little effect on inflammation. The existence of additional COX enzymes was therefore postulated. Investigations of the relative sensitivity of the 2 enzymes to paracetamol found that although the drug was a weak inhibitor of both enzymes, COX-1 was marginally more sensitive than COX-216. In view of the low sensitivity to paracetamol of both COX-1 and COX-2, the existence of a new, so far unknown isoform of COX provisionally named COX-3 has been postulated11. Chandrasekharan et al.17 discovered the enzyme COX-3, an enzyme derived from the same COX-1 gene, observing its highest levels of message in the cerebral cortex and heart. Common analgesic/antipyretic drugs and NSAIDs were tested for their ability to inhibit of COX-1, -2, and -3 activities. At a higher concentration of substrate, only COX-3 was inhibited by paracetamol. These authors concluded that the inhibition of COX-3 in the brain might be the long sought-after mechanism of the action of paracetamol. But pain is a difficult process to unravel. Prostanoids produced at sites of inflammation can sensitize nerve endings and therefore promote the localized feelings of pain associated with inflammatory events and tissue injury18. These prostanoids can be produced by COX-2 induced by the local inflammatory processes. It remains unclear how paracetamol causes its analgesic effects, once it is not a peripheral anti-inflammatory drug. Therefore, paracetamol might act in an additional enzyme19. Simmons et al.20 have previously proposed the existence of an isoform of COX-2 (COX-2b) that is particularly sensitive to paracetamol. Then the presumable site of action of paracetamol might be both in the locally acting “COX-2b” and COX-3 in the centrally acting, but these points still need to be proved. The potential for adverse effects from paracetamol seems to be singularly confined to the situation in which there is an acute overdose, and herein lies its main therapeutic advantage over aspirin. The most serious manifestation of paracetamol overdose is hepatotoxicity. The degree of liver damage is directly related to the amount of drug ingested, and people with preexisting liver disease are most susceptible21. The clinical use of paracetamol in dentistry is shown in Table 1. DipyroneDipyrone, a drug of the pyrazolone group, exhibits analgesic and antipyretic activity and its action may be central as well as peripheral22. In dentistry, dipyrone, like aspirin and paracetamol, is indicated to produce low or moderate analgesia in adults and children6. An important point to understand the mechanism of inflammation and pain is to understand the hyperalgesia, which results from excitatory actions of endogenous mediators released by inflamed or damaged tissues23. The biochemical mechanism of up-regulation (hyperalgesia) is through the increase of cAMP and Ca2+. Prostaglandins and dopamine are the most potent stimulators of neuronal tissue adenylate cyclase and are the most active up-regulators of nociceptors. It has been shown that inhibitors of cAMP inactivation potentiate the up-regulation of the nociceptors24. When the nociceptor is up regulated, drugs that block the release of prostaglandin or sympathomimetic amines are not effective as analgesic agents. Ferreira et al.24 described that repeated administration of nociceptor up-regulatory stimuli induces a state of persistent hyperalgesia, which cannot be treated with standard COX inhibitors (NSAIDs). Dipyrone can be considered an analgesic that directly down-regulates the nociceptor, because it reduces the state of persistent hyperalgesia decreasing calcium and cAMP concentrations25. Unlike aspirin and other NSAIDs dipyrone has been suggested as a classic analgesic acting in the prevention and elimination of dental pain6. Recent research carried out at the Hospital das Clínicas de São Paulo showed that more than 50% of the patients reported dipyrone as the preferable analgesic26. In dentistry, dipyrone is the most effective analgesic used in elective surgery and demonstrates the same potency as do paracetamol and aspirin27. Dipyrone use has been discussed because of its absolute risk of mortality caused by agranulocytosis, aplastic anemia, anaphylaxis and upper gastrointestinal complications. Andrade28 reported that this risk appears to be similar to that caused by paracetamol and substantially lower than the risk associated with aspirin and diclofenac, drugs commonly used for short-term pain relief. These considerations are well explained in the Boston Study29 and in the Painel internacional de avaliação da segurança da dipirona30, showing the safety of this drug, as will be discussed in the next article of this series. The clinical use of dipyrone in dentistry is presented in Table 1. In conclusion, only dipyrone is a classic analgesic, acting effectively even after the hyperalgesia process sets out. It is commonly prescribed in Brazil and seems to have the same analgesic efficacy, as do paracetamol and aspirin. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}