 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
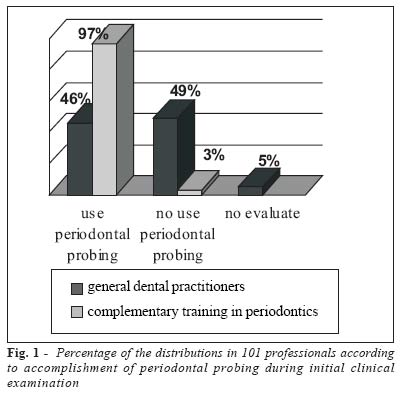
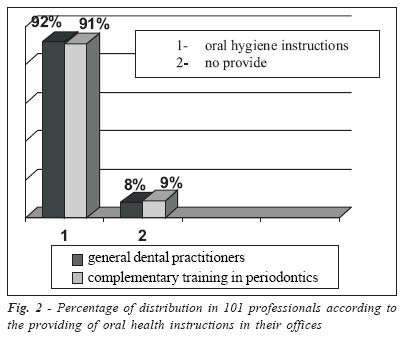
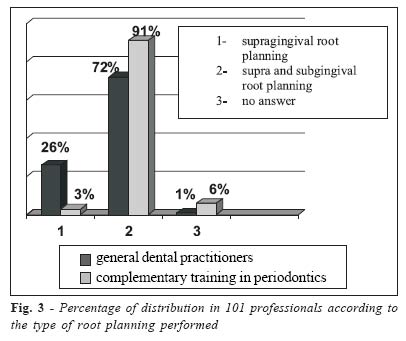
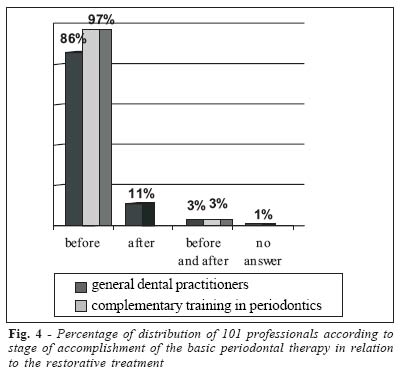
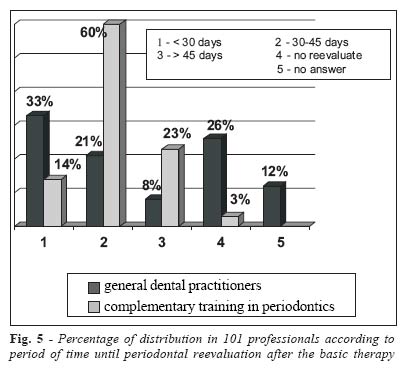
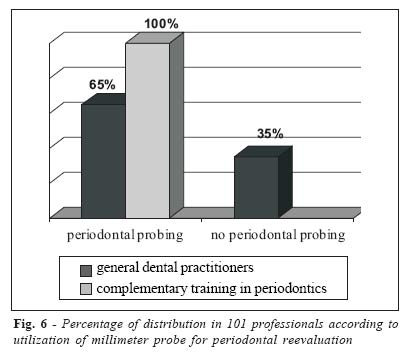
Brazilian Journal of Oral Sciences, Vol. 4, No. 14, July/Sept. 2005, pp. 773-777 Assessment of periodontal non-surgical treatment performed by general dentists and specialists in periodontics Luciana de Rezende Pinto1 Joni Augusto Cirelli2 1DDS ,Graduate student Department of Prosthodontics - Bauru Scholl of Dentistry - University of São Paulo USP Bauru, São Paulo, Brazil 2DDS, PhD, Assistant Professor Department of Diagnosis and Surgery School of Dentistry at Araraquara – São Paulo State University - UNESP Araraquara, São Paulo, Brazil Correspondence to: Luciana de Rezende Pinto Rua José Ferreira Marques, 10-41, apto.710 Vila Cidade Universitária CEP: 17011-570 Bauru – SP Tel: (14) 3227-3279 E-mail: lucianaderezende@yahoo.com.br Received for publication: November 29, 2004 Code Number: os05025 Abstract The aim of this study was to evaluate the behavior of general dental practitioners (GP) and dentists with complementary training in Periodontics (CTP) as to the need of accomplishment of this procedure. A questionnaire was applied to 130 professionals, 29 were returned not completed and then, eliminated of the sample. The results demonstrated that 97% of the CTP professionals performed probing during periodontal evaluation and 49% of the GP do not employ it. Most professionals of both groups provide oral hygiene instructions (92% GP and 91% CTP) and supra and subgingival root planning (72% GP and 91% CTP). The basic periodontal therapy is performed before the restorative treatment by 86% of the GP and 97% of the CTP. As to the period on which periodontal reevaluation was achieved after treatment, 33% of the GP performed this procedure in less than 30 days, from which 65% employed a periodontal probe. In the CTP group, 60% reevaluated the patient after 30 to 45 days and 100% used periodontal probe in this procedure. It is concluded that even though the basic periodontal therapy is properly performed by most professionals, the utilization of a periodontal probe as a diagnostic mean for periodontal diseases is neglected. Key Words: dental scaling, oral diagnosis, periodontal disease IntroductionOral hygiene methods have been recommended as a preventive measure against dental and periodontal diseases. However, the meaning of dental deposits in the development of periodontal diseases was not scientifically based until the middle of last century, when well-conducted epidemiological investigations were developed1-5. As a consequence of such studies, it is currently established that the presence of the dental biofilm is paramount for the establishment and development of periodontal disease. Additional evidence of the role played by bacteria in the dental biofilm on the development of periodontal disease was provided by studies, on which its evolution was significantly delayed by the introduction of proper oral hygiene measures and, in motivated individuals, the basic periodontal therapy may almost hinder the evolution of periodontal disease6-7. The basic periodontal therapy aims at controlling or eliminating gingivitis and impeding progression of the destruction of periodontal tissues by means of removal or control of the microbial deposits. Therefore, it is directed for preservation of natural dentition, maintenance and enhancement of periodontal health, comfort, esthetics and function8. To achieve such objectives, the basic periodontal therapy comprises patient’s modes to combat the disease, providing instructions on proper oral hygiene techniques; accomplishment of root planning and scaling, with the removal of microbial deposits present on the tooth surface, and the removal of additional biofilm retention factors such as defective margins of restorations and poorly fitted crowns, providing the patient for better conditions of controlling biofilm9-10. Considering the role played by basic periodontal therapy on the control of periodontal diseases and maintenance of the health of these tissues, the dental professionals, especially general practitioners, should be informed on the proper accomplishment of these therapeutic procedures, from diagnosis to treatment plan up to reevaluation of the results achieved and referral of the patient to a specialist if required. The aim of this study was to evaluate the behavior of dental professionals as to the diagnosis of periodontal diseases and therapeutic procedures accomplished. Material and MethodsThe study population comprised 130 dentists, both general practitioners (GP) and professionals with complementary training in Periodontics (CTP) from the city of Sao Jose do Rio Preto -SP. This group included general practitioners who had attended a training course in Periodontics with at least 80 hours and specialists in Periodontics. The instrument for analysis was a questionnaire containing multiple-choice questions, related to the methods for diagnosis of periodontal diseases, basic periodontal procedures accomplished in the dental office, including type of treatment, stage on which it is performed within the overall treatment plan of the patient, reevaluation of the results achieved and referral of the patient to the specialist (the latter just for the group of general practitioners). The questionnaires were left on the professionals’ offices and collected after one week, with avoidance of the investigator’s presence during completion of the questionnaires. Data were entered in a Microsoft Excel 97 worksheet and submitted to descriptive statistics. ResultsA hundred thirty questionnaires were distributioned, but only 101 professionals answered it. The sample was composed by 76 general dental practitioners (GP) and 35 dentists with complementary training in Periodontics (CTP). The CTP group included 23 specialists in Periodontics and 12 general practitioners who had attended a training course in Periodontics with at least 80 hours The results are represented in graphs (graph 1-6) and each one corresponds to a specific question from the questionnaire applied. DiscussionAccording to the guidelines for Periodontal Therapy of the American Academy of Periodontics, all patients should be submitted to a complete and systematic periodontal examination, including the patient’s medical and dental history, clinical examination of the periodontal structures, presence or not of inflammation, caries, prosthesis or implants, tooth mobility, furcation lesions, malocclusions, occlusal pathologies, besides probing of all teeth and periapical and bitewing radiographic examination11. The authors referred unanimously state that the manual periodontal probe is the most important tool for clinical diagnosis and it is the only method to control the progression or regression of periodontal disease, by means of the longitudinal control of the changes in the values achieved by probing for measurement of the attachment level, recorded from a fixed reference point12,. Moreover, the utilization of the probe is fundamental for detection of inflammatory exudates and bleeding associated to the pocket depth, which is an important indicator of active periodontal disease13. Figure 1 displays percentage of distributions in 101 professionals according to accomplishment of periodontal probing during initial clinical examination. It may be observed that most professionals with complementary training in Periodontics (97%) accomplish probing, whereas 49% of the PG does not perform it, therefore neglecting the periodontal examination and affecting the treatment success. Figure 2 indicates percentage of distribution in 101 professionals according to the providing of oral health instructions in their offices. The results demonstrated that most professionals in both groups (92% of the GP and 91% of the CTP) provide oral hygiene instructions for their patients. This procedure is fundamental for any dental professional. Oral hygiene instructions encourage and motivate the patient; moreover, the success of any dental treatment depends on the proper control of biofilm. According to the guidelines of the American Academy of Periodontics, patient education on oral hygiene and awareness of the need to control risk factors such as smoking, stress and diet are part of the periodontal treatment and should be applied to all patients11. The success of failure of the attempt to avoid inflammation and attachment loss for extended periods of time, basically, depends on the oral hygiene level, and also on other measures adopted for reduction of the supra and subgingival biofilm14. As regards the accomplishment of periodontal therapy (figure 3), 72% of the 76 interviewees of the GP group answered that they performed supra and subgingival root planning, even though most general practitioners investigated do not employ the probe for periodontal evaluation. This indicates that these professionals plan and conduct the basic periodontal therapy without a precise diagnosis of the subgingival calculus. Thin layers of calculus may not be noticed on visual examination, thus utilization of probe and manual scaling instruments is required for detection of subgingival calculus. Such procedures are fundamentally important, since partial removal of contaminated calculus does not eliminate the local etiologic factor, contributing to the advancement of periodontal disease12,15. However, most of the group including professionals with complementary training in Periodontics employs the probe for diagnosis of periodontal diseases and performs supra and subgingival root planning (91%). Most dental professionals in both study groups performed the basic periodontal therapy before the restorative treatment, as demonstrated in figure 4. In addition, 3% of both groups stated to employ this treatment before and after the restorative treatment, depending on the oral hygiene conditions of each patient. Another fundamental step for the success of periodontal therapy are the periodic reevaluations that determine whether there is progression of the periodontal disease, both for the patients submitted to surgical treatment and for the nonsurgical treatments, and the utilization of the probe as a tool for measurement of the pocket probing depth and attachment level gain is paramount16-17. During the periodical reevaluations, in those cases with no progression of periodontal disease, healing of the periodontal pocket is observed after removal of the local irritant, when the signs of inflammation disappear and the junctional epithelium recovers its attachment level. This healing occurs at about 45 days and may be observed by the utilization of the periodontal probe, since there will be a decrease in probing depth14. Figure 5 demonstrates percentage of distribution in 101 professionals according to period of time until periodontal reevaluation after the basic therapy. Thirty three percent of the general practitioners carry out reevaluation before 30 days and 26% do not evaluate the periodontal status of their patients after completion of the basic periodontal therapy. Moreover, among the professionals in this group who perform reevaluation, 35% do it improperly, without using the periodontal probe (figure 6). In these conditions, observation of the treatment success and elimination of periodontal disease are affected, impairing the correct detection of the cases requiring periodontal re-treatment. On the other hand, the majority of the group constituted by dentists with complementary training in Periodontics (60%) reevaluates the patients after 30 or 45 days after completion of the basic periodontal therapy, and 100% do it with probing. According to the results obtained in this study, we can conclude that: a) Most general practitioners included in this study accomplish periodontal examination in their patient in an incomplete manner and without the utilization of the periodontal probe. On the other hand, professionals with complementary training in Periodontics perform the examination properly; b) Most dental professionals investigated carry out basic periodontal procedures in a complete manner, comprising supra and subgingival root planning; c) A larger failure was observed on treatment reevaluation, which is not performed or is improperly accomplished by most general practitioners. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}