 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
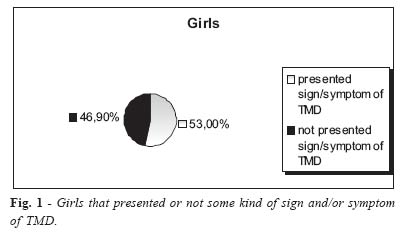
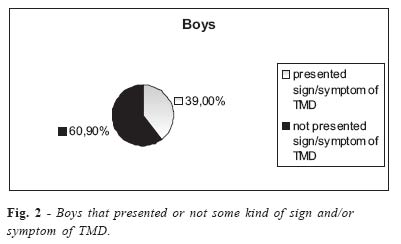
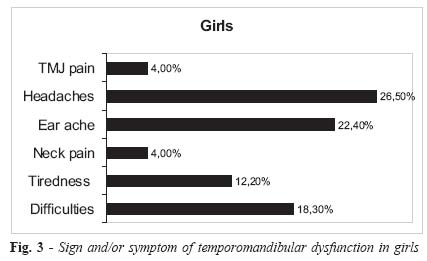
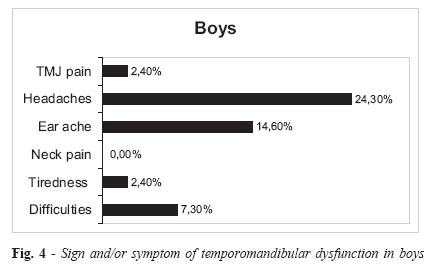
Brazilian Journal of Oral Sciences, Vol. 4, No. 14, July/Sept. 2005, pp. 787-790 Symptomatology of the temporomandibular dysfunction related to parafunctional habits in children Juliana P.Tosato1 Daniela Ap. Biasotto-Gonzalez2. 1Department of Anatomy, Faculdade de Odontologia de Piracicaba (FOP/UNICAMP) -Piracicaba; 2Department of Physical Therapy, University Center Nove de Julho - São Paulo, Brazil. Correspondence to:Juliana de Paiva Tosato Jacarandá st, 232 Condomínio Arujazinho IV 07400-000 Arujá –SP, Brazil Phone: 55 11 46541840 E-mail: julianadepaivatosato@ig.com.br Received for publication: February 01, 2005 Code Number: os05028 Abstract The study focused on verifying the prevalence of Temporomandibular Dysfunction in children, correlating it to their parafunctional habits. A questionnaire was utilized, which was answered by the mothers of 90 children aging three to seven years old (49 girls and 41 boys). The questionnaire inquired whether the child presented pain in the TMJ, head, ears, or in the neck region; tiredness or difficulty when chewing; if he/she used pacifier; habits like biting pens, chewing gum, teeth grinding or clenching, and biting the nails. Among the interviewed girls, 53% showed some sign or symptom of TMD, while among the boys, this prevalence was 39%. The most common complaint was headache. When considering the habits, they were more frequent among the children who presented pain or discomfort. So, parafunctions can be an important factor contributing to the etiology of the dysfunctions. Key Words: temporomandibular joint, children, parafunctions habits IntroductionAbnormal functioning of the temporomandibular joint (TMJ) appears with several motives, and the parafunctional habits can be one of these factors, among others1. The temporomandibular dysfunctions (TMD) are more frequent observed in female subjects2-3. Souza4 showed that 97,9% of all alterations occurred in women followed by the characteristic signs and symptoms. Santos et al.5 verified in a casuistics the articular cracking noise predominance in 51% of the TMD cases studied. Correia2 found bilateral pain as the most common complaint. Magnussos et al.6 noted the presence of muscular pain in these patients. Headaches and/ or ear ache were also frequent symptoms found7, just as tiredness or difficulty in chewing food. Problems located in this joint are usually found in the adult phase, however, they can start early in the infancy, and they can be related to the child’s habits8. Parafunctional activities of the masticatory system such as the bruxism, which includes teeth grinding or clenching, harms the joint by decreasing the intra-articular space. According to SHINKAI et al (1998) nocturnal eccentric bruxism is presented in 28,64% of children between two and eleven years old9. Another frequent habit among children is the thumb or pacifier sucking, which is more often seen in girls10. This can also trigger TMD, causing anterior open bite, mandibular retrusion, maxilar protrusion, excessive overbite, vestibule version of the superior incisors, posterior cross bite, ogival palate, and angular deformities11. Besides these habits, chewing gum, and biting on pens and nails can influence in the temporomandibular biomechanics, damaging it. Parafunctional activities in general, according to Almeida12, are present in 72,2% of children between four and seven years old. So, observing the harmful outcomes parafunctions may bring to the TMJ, the present study aim to verify the prevalence of signs and/or symptoms of temporomandibular disorders in children aging three to seven years old, correlating it to their daily habits. Material and MethodsVolunteers To accomplish this study, 102 mothers of three to seven year old children were interviewed. Was excluded 12 children, because six children was mouth respiration, and six questionnaires wasn’t be complete answered. Was included in the study 90 children being 49 girls and 41 boys. 13,33% was studying at the maternal II; 15,55% at Jardim I; 22,22% at Jardim II; 23,33% at Pré-school and 25,55% at first grade. To collect the data a questionnaire was applied on the mothers. This questionnaire was created to verify the symptomatology of TMD and the parafunctional habits in the children. In the literature wasn’t found a valid questionnaire that answers the necessity of this study. ConductsInitially, an authorization was asked for the board of directors of two different schools (one particular school and one public school). After the authorization was received, the questionnaires were sent to the mothers through the children, with a pamphlet explanation, and phone number if they have doubts. The questionnaire asked if the child presented pain in the TMJ, head, ear, or neck; tiredness or difficulty in chewing; knowledge of any postural change; if the child had already replaced the deciduous teeth; if the child was breast fed; used any pacifier or baby’s bottle; when did the child start to eat solid food; habits of biting the pen, chew gum, grinding or clenching the teeth, biting nails, and sucking the thumb. ResultsBy observing the collected data, a high level of prevalence was found regarding the symptomatology of dysfunction. Fifty-three percent of the interviewed girls presented some kind of sign and/or symptom of temporomandibular dysfunction, as showed in Figure 01; now, among the boys, thirty-nine percent presented some sort of sign and/or symptom of dysfunction (Figure 02). Among the interviewed girls, 4% presented TMJ pain, 26,5% presented headaches, 22,4% ear ache, and 4% presented neck pain. When considering discomfort in the temporomandibular joint area, 12,2% presented tiredness when chewing, and 18,3% had difficulties (Figure 03). Among the interviewed boys, 2,4% presented TMJ pain, 24,3% headaches, 14,6% ear ache, and no subject presented pain in the cervical region. Now, when considering discomfort in the temporomandibular joint area, 2,4% presented tiredness when chewing, and 7,3% had difficulties (Figure 04). It was observed a prevalence of common habits among the girls who presented any kind of TMD sign and/or symptom, differently from the ones who reported no pain or discomfort. The girls who presented some sort of alteration, 61,5% used pacifiers, 38,4% bite on pens, 30,7% chew gums, 26,9% grind the teeth, 11,5% clench the teeth, 42,3% bite on the nails. In the girls who did not present alterations, these habits were less frequent, 56,6% used pacifiers, 21,7% bite on pens, 17,3% chew gums, 13% grind the teeth, 4,3% clench the teeth, and 17,3% bite on the nails. Among the boys, parafunctions were also more frequent in those who presented signs and/or symptoms of dysfunction. 56,2% used pacifiers, 25% bite on pens, 12,5% chew gums, 31,2% grind the teeth, 25% clench the teeth, and 37,5% bite on the nails. Now, among the ones who did not present any alterations, 72% used pacifiers, 24% bite on pens, 28% chew gums, 24% grind the teeth, 20% clench the teeth, and 16% bite on the nails. The use of pacifier, along with the habit of chewing gums, were the most frequent habits among the children without pain or discomfort. DiscussionAfter analyzing the collected results through the answered questionnaires by the children’s mothers, as done in other studies7,9, a higher prevalence of signs and symptoms of temporomandibular dysfunction was found among the girls, which consents with the literature, showing the higher incidence of this dysfunction in the female gender2-4. It can be observed that the beginning of these signs and symptoms can occur during infancy. According to Hara et al.8, the TMD signs and/or symptoms are frequently recorded in earlier ages. Clinically, infant bruxism can be related to muscular and articular dyscomfort13-14. Thus, it is easily comprehended the high prevalence found in children with teeth grinding or clenching among those who presented any TMD signs and/ or symptoms. However, a number of children with bruxism were found with no pain or discomfort, but they may in the future present temporomandibular disorders because there is a significant correlation between bruxism and these type of alterations15, which can also be the main etiological factor for TMJ disorders16. Biting nails and biting the tip of the pen were the other frequent habits seen in the children with dysfunction, which was already found in other past studies. These two habits are usually performed in one side of the mouth, leading to a mandible laterality and to a unilateral overstrain, which will then lead to a type of unbalance. Therefore, parafunctions may be an important factor causing temporomandibular dysfunction, with common habits found in children with alterations, and a higher prevalence of parafunctions in those who presented any type of complaints. According to Almeida12, any factor capable of altering the perfect function of the stomatognathic system can provoke the onset of TMD signs and/or symptoms. Caution should be taken upon the children who do not present any problems, once parafunctions may bring future harm. It is believed that the percentile related to pain in the TMJ area may be much bigger than the percentile found until now, however, it is hard to obtain the exact location of the pain due to the young ages of the children. It is observed that the children who presented any kind of pain or discomfort had common habits, which could be important factor acting in the cause of any dysfunction. Besides, this symptomatology presented in children should be observed as to prevent any serious future dysfunction, avoiding pain and discomfort on these children when they reach the adult phase. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}