 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
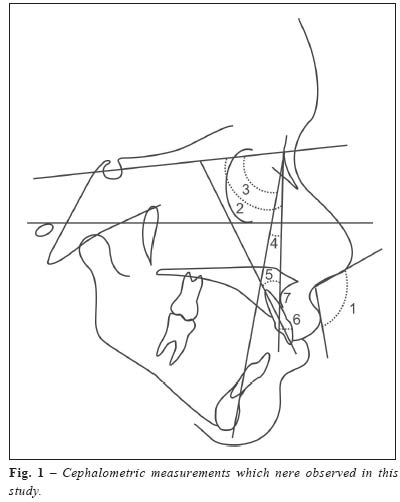
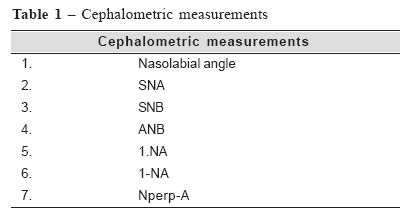
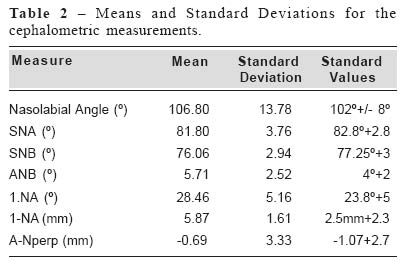
Brazilian Journal of Oral Sciences, Vol. 4, No. 14, July/Sept. 2005, pp. 798-800 Nasolabial angle in finger sucking patients Mayury Kuramae1 Ivana Uglik Garbui1 Maria Beatriz Borges de Araujo Magnani2 João Sarmento Pereira Neto2 Gláucia Maria Bovi Ambrosano3 1DDS, PhD Student, Piracicaba Dental School, Unicamp, Brazil 2Professor in Orthodontics, Piracicaba Dental School, Unicamp, Brazil 3Professor in Biostatistic, Piracicaba Dental School, Unicamp, Brazil Correspondence to: Mayury Kuramae Rua Major Campos, 792- Bairro Alto CEP: 18601-040 –Botucatu –SP Phone: (14)38823315 E-mail: mayury@bol.com.br Received for publication: March 08, 2004 Code Number: os05030 Abstract The purpose of this study is to analise the nasolabial angle and other cephalometric measurements that express the anteroposterior relationship of maxilla and mandibule in individuals with finger sucking habit. Thirty lateral cephalograms were selected from the patient files of the scientific documentation service, Orthodontic Graduation Course of the Piracicaba College of Dentistry, FOP/UNICAMP. The selection criteria was white Brazilian female subjects, 7 to 10 years old, in the phase of mixed dentition, and presenting finger sucking habit. The observed cephalometric measurements were: nasolabial angle, SNA, SNB, ANB, 1.NA, 1-NA and Nperp-A. The results were compared using Student’s ‘t’ test and, significance level of 5% (á = 0,05). The analysis showed no differences in the nasolabial angle in subjects presenting finger sucking habit; the maxilla and mandibule was well positioned, relative to the cranial base, and the upper incisors were well positioned. Key Words: facial profile, habits, cephalometrics, normal occlusion Introduction Sucking habits are known to have an inherent potential to provoke skeletal and dental disturbances1-2. Sucking habits might cause occlusal anomalies, such as anterior open bite and posterior crossbite3. Specifically, active sucking causes a reduced vertical growth of the alveolar process and the upper incisor were positioned more labial, and results in anterior open bite and more overbite4. Finger sucking is one of the main ethiological factors of anterior open bite5-6. The simple removal of the habit until the beginning of the mixed dentition may cause an spontaneous correction of the resulting occlusal anomalies3-4. This compensatory dentoalveolar mechanism is characterized by a relative growth of the dentoalveolar heigth of the maxilla and mandibule during mixed dentition, and by reducing posteriro dentoalveolar heigth in permanent dentition7. Skeletal changes persist even after the removal of the parafunctional habit3. The typical skeletal pattern of open bite also remains in subjects who showed and apparently spontaneous regression without any orthodontic treatment4,8. Improvement on facial esthetics hás become one of the main objectives of orthodontic treatment. However, current concepts on facial appearance are very controversial and are not clearly formulated. Evaluations of facial esthetics might be influenced only by the orthodontist’s individual concept. The nasolabial angle9 shows how the upper lip relates to the collumela line, irrespective of other soft tissue references far from the upper lip. Its clinical application was shown to be a trustworthy method for determining the sagittal position of the maxilla10-11. The values of the nasolabial angle observed in Brazilian suggest some tendency to labial protrusion, and the alterations of the nasolabial angle which are caused by the changes in upper incisors positioning during facial growth do not significantly affect this measure12. In search of a better understanding of facial changes that result from sucking habits, and knowing the difficulties of orthodontic treatment of anterior open bite, the purpose of this study is to observe the behavior of the nasolabial angle anteroposterior positioning of the maxilla and mandibule and the incisor position of subjects presenting the finger sucking habit. Material and MethodsThirty lateral cephalograms were selected from the patient files of the scientific documentation service, Orthodontic Graduation Course of the Piracicaba College of Dentistry, FOP/UNICAMP. The selection criteria was white Brazilian female subjects, 7 to 10 years old, in the phase of mixed dentition, and presenting finger sucking habit. This material was used occording to standards of the health ministry and the resolution number 196/96 of national health council. This study was approved by ethics in human research committee of the university, under the protocol number 139/2003. Cephalograms were drawn in a dark room by an only operator using a standard sized ultraphan paper (17.5cm x 17.5cm; 0.07mm thickness), a 0.3mm lead mechanical pencil, transparent ruler to the nearest 0.5mm, protactor to the nearest 0.1º, template, adhesive tape and illuminator; anatomical structures of skull and face were outlined, as well as lines and planes wich originate the cephalometric measurements that were used in this study (Figure 1, Table 1). In order to determine the cephalometric tracing error, the radiographs qere twice traced after at least 10 days from first drawing, and the mean was calculated13 for each measurement. The results were compared using Student’s ‘t’test and, significance level of 5% (á = 0,05). Results and Discussion The nasolabial angle describes the position of the maxilla, so that when it shows a greater value, it also reflects a maxillary retrusion; and, reversely, a maxillary protrusion. The mean value (Table 2) obtained in this study for the nasolabial angle was 106.80º (+ 13.78), that is, it ranges within normality standards, according to McNamara Jr9. The SNA angle (Table 2) indicates the maxillary anteroposterior positioning, and, in the present study, it was observed to range within normality standards since the calculated mean was 81.80º (+ 3.76), thus showing that, in this sample, subjects presented an adequately positioned maxilla, relative to the cranial base14. Another cephalometric measurement that relates the maxilla and the cranial base is Nperp-A9, which, during the mixed dentition, must show a point A coincident to N-perp line. In this study, the mean value for Nperp-A (Table 2) was –0.69mm (+ 3.33), showing no significant differences from standard values, according to Martins et al.15. The SNB angle indicates the anteroposterior positioning of the lower jaw, relating to the cranial base, and ANB indicates the anteroposterior discrepancy of the jaws, which showed (Table 2) a mean value of 5.71º (+2.52). For the present sample, SNB (Table 2) presented a mean value of 76.06º (+2.94), thus indicating normality standards, according to Martins et al.15. As for upper incisors positioning, the mean value for 1.NA (Table 2) was 28.46º (+ 5.16) and the mean value for 1-NA (table 2) was 5.87mm (+ 1,61), demonstrating normality standards, according to Martins et al.15. Although that the compressive forces exerted by the finger during sucking, since bone, though one of the hardest tissues of the body, is the one which best responds to external forces1-2,14 not results in anteroposterior and dentoalveolar discrepancies in this present sample. According to our proposal and by the results obtained from the studied sample, our conclusions are: no statistically significant differences in the nasolabial angle in subjects presenting finger sucking habit; the maxilla and mandibule was well positioned, relative to the cranial base, and the upper incisors were well positioned. References
|

{kind=link}
{kind=link}
{kind=link}