 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
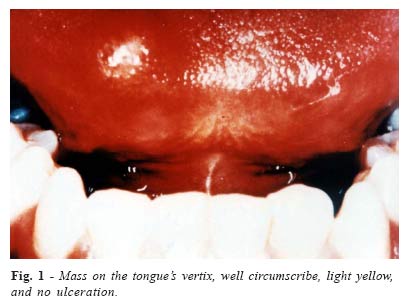
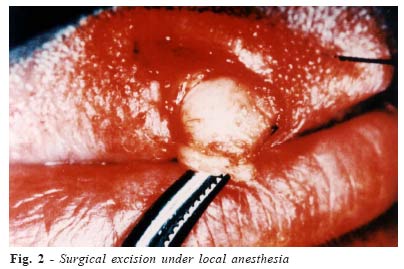
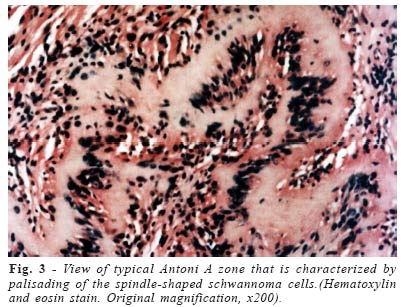
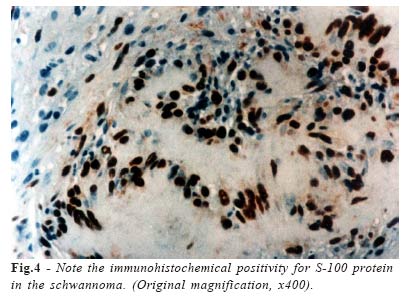
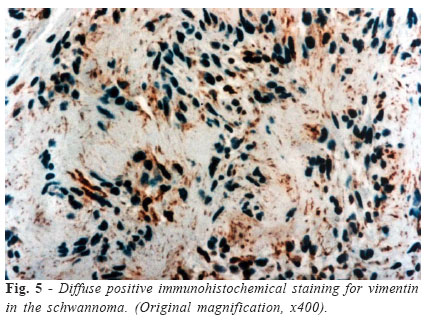
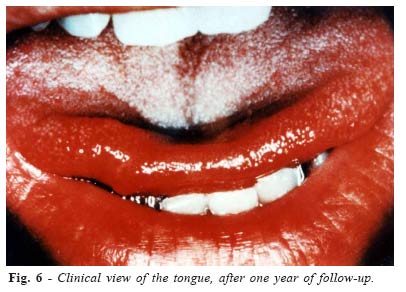
Brazilian Journal of Oral Sciences, Vol. 4, No. 14, July/Sept. 2005, pp. 806-809 Schwannoma of the oral cavity.Histological and immunohistochemical features Sandra De Cássia Santana Sardinha1* Aleysson Olímpio Paza2* Pablo Agustin Vargas3* Roger William Fernandes Moreira4* Márcio de Moraes5*1Resident Oral Maxillofacial Surgery 2 Resident Oral Maxillofacial Surgery 3Professor Oral Pathology 4Professor Oral Maxillofacial Surgery 5Professor Oral Maxillofacial Surgery * Piracicaba Dental School - UNICAMP Correspondence to:Márcio de Moraes Faculdade de Odontologia de Piracicaba –UNICAMP Avenida Limeira, 901, Areião CEP: 13.414-903 Caixa Postal: 52 Piracicaba-SP, Brasil Phone: +55-19-3412-5326 E-mail: mmoraes@fop.unicamp.br Received for publication: March 08, 2004 Code Number: os05032 Abstract Schwannoma is a relatively uncommon, slowly growing lesion that is most commonly encountered in the nerve sheath. The mobile portion of the tongue is the most common site, followed by the palate, floor of mouth, buccal mucosa, lips, and jaws. The present case report refere a 13-year-old boy with a tongue mass that did not interfere with the speech. The histopathology and immunohistochemistry study of the excised lesion showed a Schwannoma of the tongue. Key Words: neurilemoma, schwannoma, oral cavity, tongue , immunohistochemistry Introduction Schwannoma has been defined as a benign, encapsulated neoplasm that arises in the nerve fiber. This neoplasm is composed primarily of Schwann cells in a poorly collagenized stroma1. The etiology is unknown, but it is postulated that the lesion arises by the proliferation of Schwann cells at one point inside the perineurium. The growth of this lesion will cause the displacement and compression of the surrounding normal nerve tissue. The tumor may arise at any age. Some series have reported that the schwannoma is more common in adults, in contrast to the neurofibroma which tends to be more frequent in young children2. Most reports suggest that the majority of tumors are present between the ages of 10 and 40 years3-4. Some series report a higher incidence of Schwannoma in the female population3, while others show a slight male predominance4. Clinically, the tumor appears as a smooth-surfaced, usually painless, soft-tissue swelling with intact overlying epithelium. There have been approximately 146 schwannomas reported from the oral soft tissues3-5. The schwannoma is usually a solitary lesion. When multiple, however, they be associated with neurofibromatosis1. The differentiation between schwannoma from neurofibroma is essential, because an apparently “solitary”neurofibroma may be a manifestation of neurofibromatosis. Fifteen to sixteen percent of pacients with neurofibromatosis will present malignant transformation in one or more lesions, contrary to schwannoma1. Histologically, the schwannoma is encapsulated and consists of varying quantities of two types of tissues-Antoni A and Antoni B. The treatment for schwannoma is surgical excision. Recurrence after excision of schwannoma is rare. Malignant change has been reported, however this is an extremely rare phenomenon. Clinical CaseA 13-year-old boy was admitted to the Maxillofacial Surgery Service of the Campinas State University, São Paulo, Brazil, for treatment of a swelling on the tongue. The patient’s mother stated the presence of painless, slow growing lesion for the past few years. No problems with speeching or swollowing were reported. The lesion was founded during a routine dental examination. Oral examination revealed a yellowish, well circunscribed mass on the vertix of the tongue, approximately 1.4cm x 0.6cm x 0.6cm in size. The was no tender to palpation and there was no evidence of paresthesia or ulceration (Figure 1). Macroscopically, the lesion was grossly similar to a lipoma. The patient was otherwise healthy without significant past medical history. The mass was excised under local anesthesia without complication (Figure 2). Microscopically, the schwannoma was uncapsulated and consisted of typical Antoni A zones admixed with Antoni B zones. Antoni A tissue was predominant in the present case (Figure 3). Immunohistochemical studies were positive for S-100 protein (policlonal; 1:2000 dilution; none antigen retrieval; Dako; Denmark) mainly in Antoni A areas (Figure 4). The viment antibody (V9; 1:6000 dilution; heat induced epitope retrieval; Dako; Denmark) was diffusely positive (Figure 5), and the anti-CD57(LEU-7; Dako; Denmark) was found to be negative. After 12 months of follow-up, no recurrence has been detected (Figure 6). Discussion Schwannoma is a benign tumor, apparently derived from the Schwann cells, which may arise from any myelinated nerve fiber6-7.The tumor is composed primarily of schwann cells in a poorly collagenized stroma1. This lesion is not commom in the oral cavity. The schwannoma is usually a solitary lesion, but can be multiple lesions when associated with neurofibromatosis1. Wright and Jackson1, reported 146 cases of schwannoma of the oral cavity soft tissue. Of those, 52% occurred in the tongue, 19.86% in the buccal or vestibular mucosa, 8.9% in the soft palate, and the remainder 19,24% were in the gingivae and lip. Schwannomas of the hypoglossal nerve are rare tumors. These tumors are seldomly found in the sublingual space. when present, usually involves the most peripheral segment of the hipoglossal nerve6. Histologically, schwannomas are descried as Antoni A type or Antoni B. Antoni type A present a parallel arragement of fibrocyte-like cells, and Verocay bodies. Antoni B, is less cellular and shows microvacuolation of the intercellular substance. Flickinger et al.8, reported that in most tumors both cell types are present as reported in the present case. Chrysomali et al.3, reported that schwannomas consistently showed positive staining for S-100 protein in most of the tumor cells. The staining intensity was greater in cells in the Antoni A tissue compared with that seen in the Antoni B tissue similarly to our case. On the other hand the immunorectivity for CD57 antibody was negative in our report. Chrysomoli et al.9, showed CD57-positive cells 0,1% to 10% in schwannomas and neurofibromas. Ancient schwannoma, a variant of schwannoma, was first described in the thorax by Ackerman and Taylor, in 19511. This lesion contain both Antoni A and Antoni B pattern, with pleomophic nuclei, some of which may be hyperchromatic. Area of hemorrhage hemossiderin accumulation as well as mitotic figures may be seen1. Redman et al.10, reported a case of cellular schwannoma of the mandible. This tumor differs from classic schwannoma, by its increased cellularity, nuclear pleomorphism and hyperchromatism, lack of Verocay bodies, and frequently higher mitotic activity10. Lipomas, hemangiomas, eosinophilic granuloma, epidermoid and dermoid cysts, epithelial hyperplasia, granular cell tumor, leyomioma, lymphangioma, are some of the lesions included in the differential diagnosis of schwannoma1. López and Ballestin11, reported that the histological pattern of schwannoma is easily recognizable. The management of schwannoma requeres complet surgical excision of the lesion. Schwannoma rarely recidive and not respond to radiation therapy1,12. The conclusion is that the benign Schwannoma represent a pathology which are often not taken into account during clinical pratice. Differencial diagnosis must be made in relation to numerous benign neoformations basead on epitelial and connective tissue and, malignant tumors. Immunohistochemical features can be useful in determing neural differentiation. Anti-S-100 protein is probably the single best antibody for this case. Treatment of the Schwannoma is complete surgical excision. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}