 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
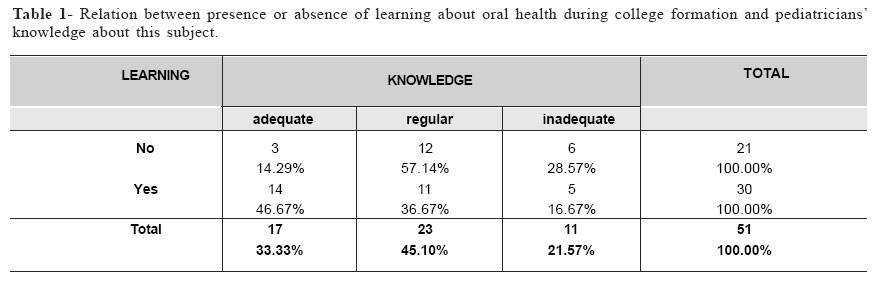
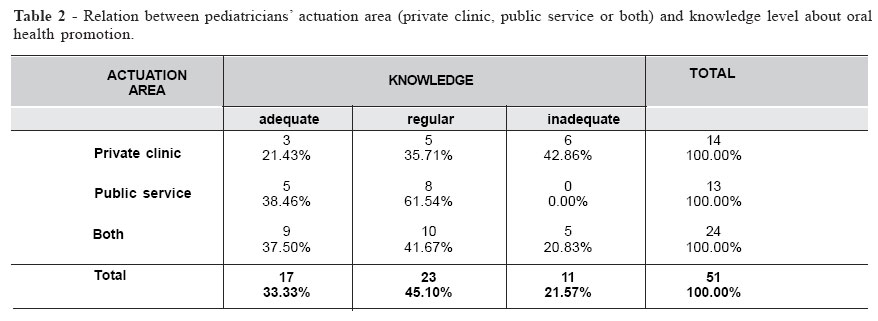
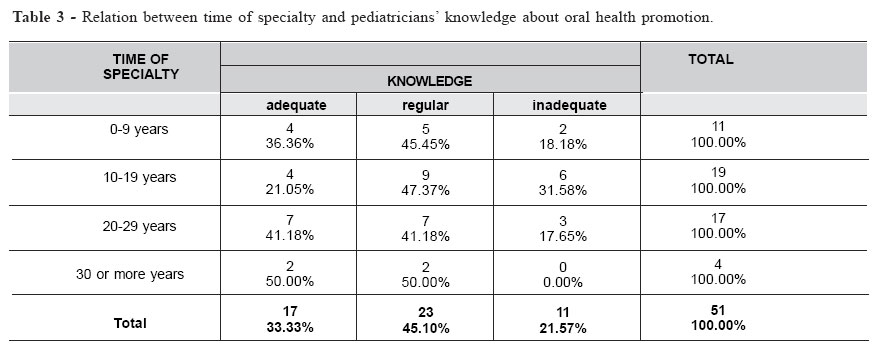
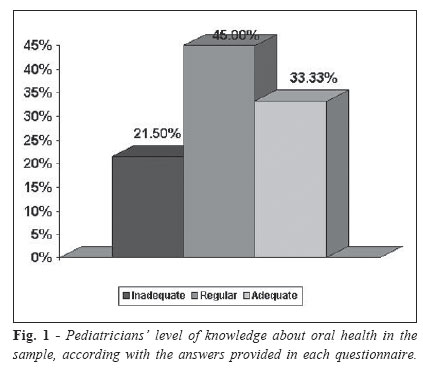
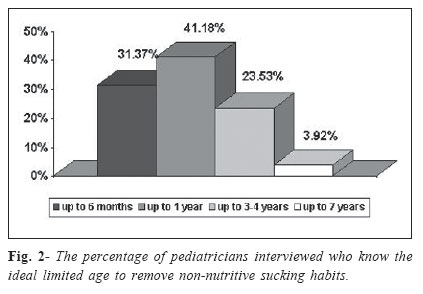
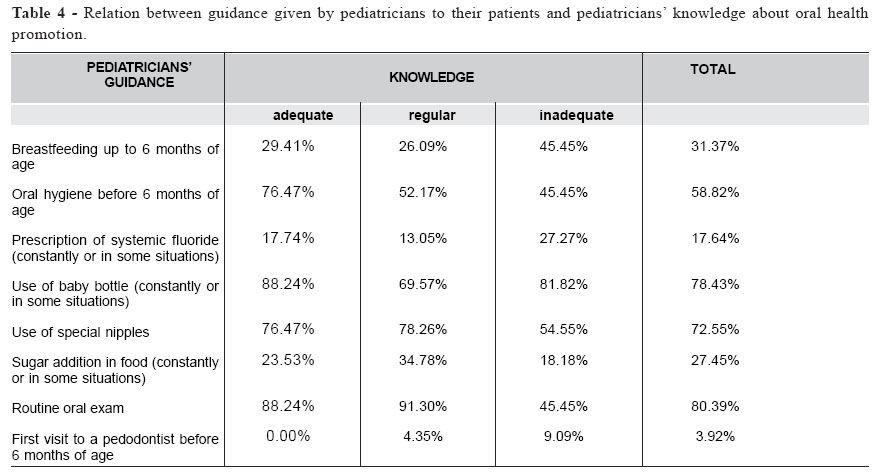
Brazilian Journal of Oral Sciences, Vol. 4, No. 15, Oct./Dec. 2005, pp. 904-910 The role of pediatrician in promoting oral health Karina Eiras Dela Coleta1 João Sarmento Pereira Neto2 Maria Beatriz Borges de Araújo Magnani2 Darcy Flávio Nouer3 1 DDS,MSD-Departament of Pediatric Clinic-Orthodontia- São Leopoldo Mandic Postgraduation Dental School, Brazil 2 Professor of the Pediatric Clinic, Departament of Pediatric Clinic, Piracicaba Dental School, Unicamp, Brazil 3 Chairman, Departament of Pediatric Clinic, Piracicaba Dental School, Unicamp, Brazil Correspondence to: Karina Eiras Dela Coleta R. Dr. Waldo Barbieri, 41 bloco5 apto.83 Jardim Paulistano CEP- 14810-273 Araraquara- S.P. Phone: (16) 3339-1602 / (16) 3336-6663 E-mail: nkpizzol@ig.com.br Received for publication: September 15, 2005 Code Number: os05038 Abstract Many problems in the oral cavity that are common in childhood can be prevented with pediatrician guidance. Due to the strict relationship between the pediatrician and child parents, the objective of this study was to evaluate pediatrician knowledge about promoting oral health, correlating this information with the professional profile. For this, issues about fluoride application, oral habits and their consequences, diet and its relation with oral health, teething development, caries control, oral hygiene and forwarding to dentist were covered. Fiftyone pediatricians that do clinical care in two different cities of São Paulo State were evaluated. In 78.3% of the cases, a regular (10 or 11 correct answers) to appropriate (12 or more correct answers) knowledge level on oral health was verified. Although the results are positive, most pediatricians do not have some important information such as breast milk cariogenicity, when teeth formation starts and the appropriate age to remove a non-nutritive sucking habit. Based on the resulting data, we conclude that pediatricians’ knowledge about oral health can and must be improved, provided that there is more integration with dentistry area, especially when doctors are still in Graduation or Post-graduation. Key Words: pediatrics, oral health/ prevention & control IntroductionBased on the principle that prevention and education are the best way of promoting oral health collectively, we can consider that health professionals such as pediatricians and pedodontists, by the contact that they establish with their patients since the first years of life, are responsible for preventing abnormalities and educating parents about their children oral health. Above all, the pediatrician as an educator has to understand, convince and motivate parents about the necessity of oral health since they are the professional that first interacts with the family, sometimes before the child’s birth1. It is evident that more prematurely preventive measures and interruption on disease evolution are established more effective will be the results. Once healthy habits are introduced, either of hygiene or dietary, they tend to extend for the whole life of the individual2. With base on caries statistics in first childhood, it can be observed that even if pediatricians have knowledge of oral diseases, most of them don’t have conditions to prevent caries disease acting alone. In general, zero-to-three-year-old Brazilian children are not taken to a dentist, unless serious problems on teething development occur2. As the first consultation to a dentist usually occurs when the child is over three years old, the pediatrician responsibility to promote and guide about oral health increases up to this period3. Thereby, for that pediatricians responsibility contributes for education and prevention is important that they are the link between the family and the dentist, guiding parents to take their child to a pedodontist prematurely, who will be able to diagnose the abnormalities in occlusal development from the beginning. Some studies on pediatricians’ level of knowledge in Preventive Dentistry, as the one realized by Tsamtsouris and Gravis4, through questionnaires sent to 1797 pediatricians from Massachusetts, receiving back 57% (1035) of them, showed that 78% of the professionals work in private clinic, 22% have academic activity, and 49% consider their knowledge in oral health area poor and unsatisfactory. The results still showed that only 32% of the pediatricians guide their patients to go to a dentist up to 12 months of age, as it is recommended by the American Pediatric Dentistry Academy. This data leads the authors to believe that, although the pediatrician can diagnose the alteration, they will not guide the child believing that they will not tolerate the treatment. Even though knowledge about oral health promotion is deficient in nearly half of the pediatricians evaluated, they have demonstrated great interest of updating their knowledge in oral health in the form of continued education, doctor-dentist meetings or deepening of the information obtained during Medical University. In this same research line, Schulte5 sent a questionnaire with 8 items to 1453 pediatricians from Chicago, receiving 21% back. From 298 of the questioned doctors, 95% reported that they exam their patients teeth before two years old, 70% consider that clinical experience was the main learning source, and 85% emphasized the importance of interaction between the pediatrician and the dentist to prevent and guide to oral health in children younger than three years old. Considering that oral health promotion is essential, it is evident that a multidisciplinary care and guidance involving pediatrician and dentist are indispensable in order that not only parents’ education is reached, but also especially a real change in their attitudes with relation to promotion and maintenance of their children oral health. Material and MethodsThe sample consisted of fifty-one pediatricians registered in the Regional Medicine Council and affiliated to the Pediatrics Society of São Paulo, and that regularly exercise their profession in Araraquara and São José do Rio Preto cities, São Paulo State, without any distinction on gender, age or where these professionals were graduated. Data was gathered from a questionnaire containing 33 questions, which was sent to pediatricians (anonymously) with an explanatory letter saying what they should do. Based on the questionnaire, the doctors were evaluated on professional formation, oral health knowledge degree and clinical application of this knowledge. The results were analyzed according to the answers provided in the questionnaire, containing questions related to oral health promotion performed by the pediatricians. At the beginning of the questionnaire some personal questions were done, which defined several characteristics of the pediatricians that are participating with the variables: gender, time after graduation and residence, learning about oral health promotion and how its knowledge was obtained, the concept that the pediatrician has on their knowledge (correct or not) and their actuation area (private clinic, public service or both). In the second part of the questionnaire (15 questions), aspects relative to pediatricians’ knowledge about caries and oral cavity exam, diet and breastfeeding, hygiene, fluoride, teething development, facial growth, deleterious habits and malocclusion development were covered. According to the answers, each pediatrician knowledge was considered inadequate, regular or adequate. The knowledge was considered inadequate when the professional hit 9 or less questions, regular if the correct answers were 10 or 11, and adequate if the pediatrician hit 12 or more questions. Those parameters were statistically established based on the interval of confidence of 95% for the mean (10.41) with a standard error of 2.65. The third part of the questionnaire refers to clinical conduct of the pediatricians involved in the sample. The study evaluated if pediatricians guide the parents about oral hygiene, the importance of breastfeeding, toothbrush and fluoride use, special nipples for baby bottle and pacifier, type of diet, and especially evaluate the interaction between the pediatrician and the pedodontist with relation to the first visit to a dentist and the reason to the recommendation. A table with the data was created in Excel (Windows 98) and the data was analyzed using the frequency of variable crossing to determine the correlation of each questionnaire with personal qualitative variables. Results and Discussion PART I - Characteristics of the pediatricians The pediatrician can be very important to children oral health, basically because of two aspects: first because the child usually visits the pediatrician before going to the pedodontist, and second because of the respect and force that the pediatricians exercise on parents6. A relevant fact is that the index of caries in first-age children is still high, demonstrating no interaction between the clinical conduct of the pediatrician in puericulture and the oral health promotion. Parents lack of guidance concerning diseases such as caries can be evidenced by the evaluation performed by Walter et al.7, that found high index, since caries lesions were diagnosed in 62.96% of the 24-36-months of age children. Pediatricians are not retransmitting the information about prevention and oral health because learning on this area is deficient in Medical courses and residence, since 21 (41.18%) of the pediatricians interviewed in our study did not receive any information about oral health during their professional formation (Table 1). The profile of the 51 pediatricians that were interviewed was predominantly male, with 46.6 years of age, and that 20 of them work in São José do Rio Preto and 31 in Araraquara. From the pediatricians evaluated, 13 work exclusively in public service, 14 only work in office or private clinic, 24 in both (Table 2). When questioned about their knowledge of oral health, 30 pediatricians (58.8%) said that they had received information about this subject, and in most cases (29,41%), during graduation. In relation to quality of learning, 20 pediatricians considered it enough (40%) or totally adequate (26,6%); and according to the qualitative evaluation, 14 of those 20 professionals showed an adequate knowledge about oral health. Although the numbers were representative, 9.8% of the pediatricians reported that they do not have any interest in acquiring information on oral health area, which is a disappointment. According to Toledo8, the pediatricians should have basic knowledge about diet and dental caries relationship as well as methods for controlling and preventing oral diseases. Comparatively, pediatricians that only work in public service presence better performance in the qualitative evaluation than those that only work in private clinics or offices, based on the number of questions correctly responded (Table 2). All pediatricians that only work in public service presented adequate or regular level of knowledge; and regarding time after residence, the current study revealed that pediatricians with 20 or more years of specialty, showed better level of knowledge about oral health (Table 3). PART II - Pediatricians’ knowledgeRegarding the second part of the questionnaire, the specific knowledge of the pediatricians about oral health was evaluated. The grades assigned to each questionnaire, showed that 33.3% of the doctors presented a knowledge level in oral health that is considered adequate (12 or more correct answers), 45% regular (10-11 correct answers), and the remaining 21.5% (9 or less correct answers) demonstrated insufficient or inadequate knowledge (Figure 1). It was observed that 13.72% do not consider caries infectious (9.8% did not know to answer), and 43.13% do not know that caries is transmissible, can occur before the child’s first year of age and has a large destructive capacity. Therefore, common attitudes such as taste the baby’s food using the same fork, knife and spoon or blow the food before the child eats continue to be used due to pediatrician lack of knowledge and parents lack of guidance. It was also observed that pediatricians consider breast milk the best source of nutrients, and that its use must be stimulated. However, a detail should be always taken into account: the breast milk cariogenicity. 70.58% of the pediatricians that were interviewed do not know that breast milk can cause caries, and so that its ingestion by children with erupting teeth should be followed by oral hygiene. The importance of breastfeeding is not only restricted to nutritional, emotional and immunological factors, as normally said. The movements that the baby does, most known as milking, are essential to good development of face and dental arch skeletal-muscle. The results shown that 72.55% of the pediatricians evaluated know the benefit of breastfeeding to obtain a correct occlusion development. In baby bottle sucking, muscle function is very distinct from that done in milking; and muscle hypo function, especially propulsive and retrusive mandibular muscles, will result in growth and development losses of the stomatognathic system. Then, due the inappropriated mechanical action set, and the temporomandibular joint will be easily affected. Breastfeeding provides the best stimulation conditions of the oral sensor-motor system. Lack of breastfeeding or its insufficiency, can stimulate non-nutritive sucking habits such as pacifier or finger that will have the function of supplying neural sucking debt. Children breastfed for at least six months do not develop sucking habits or, if so, it will be for a short period in comparison with children that were not breastfed9. It is ideal that the intervention of these non-nutritive sucking habits is premature (before four years of age), with the aim of preserving inherited anatomic shape, and thus works functional and emotional factors as well. However, part of these children has not reached neuromuscular maturity yet, so it is necessary to do this sucking work for a longer period. Just 23.53% of the pediatricians know that extending deleterious sucking habits is acceptable up to children age 3-4 years, before erupting the first permanent tooth. In this period alterations in arch and occlusion form usually are reversible, recovering adequate muscular functions and equilibrium (Figure 2). It is important to mention that 91.67% of the pediatricians that respond correctly this question, work in Araraquara. This discrepancy of results can be justified partially by the frequent lectures and courses about oral health given by dentists from Araraquara, which is a reference dentistry center in the region. Concerning dental development, just 27.45% of the pediatricians evaluated know that tooth development starts in the second month of pregnancy. However, 82.35% of the doctors reported that they are able to recognize a caries lesion, and 76.47% are able to recognize an open bite. Most pediatricians said that there is correlation among deleterious habits, including oral breath, which results in face and occlusion development alterations. PART III - Clinical conduct Regarding the third and last part of the questionnaire, where the clinical conduct of the doctors interviewed was evaluated, was observed that the guidance given by pediatricians to their patients depend on where they exercise their profession, in terms of socio-economical level. In public system, traditionally the school health programs in Brazil have been focusing on the elementary students that provide dentistry cares for those students since they are 7 years old. The government does not give much attention to zero-tosix-year-old children. Based on the results obtained from this third part, all pediatricians interviewed recommend mothers to breastfeed their children, data that is greater than the 70.2% found by Paiva et al.2. It is evident that most mothers breastfeed their children when they born, but sometimes the breastfeeding period is not enough to promote adequate growth of the jaws and, if they breastfeed within an adequate period, they make a mistake while associating a dietary complement using the baby bottle. Most health professionals recommend that the introduction of semi-solid food is delayed until swallowing reflex starts and the baby has independent movements of tongues, lips and mandible, and can remain sat. Generally, these development stages occur from 4-6 months of age10. With relation to sugar addition in food, 13.73% said that they indicate constantly, and the other 13.73% indicate in some situations (Table 4). Paiva et al.2 found values higher than ours, observing that 66.7% of the pediatricians recommend to put sugar in foods, and that 48% of them advice the use of common sugar. It is important to emphasize that ingesting a high quantity of sugar in the first years establishes a lifelong standard that is difficult to change11-12. It is known that sugar has energetic capacity of quick assimilation and is very much used in malnutrition cases. However, there is no justification to use it abusively in healthy children. With relation to teeth, the risk of baby bottle caries is always present when milk with sugar is not followed by good oral hygiene. Concerning baby bottle, 78.43% of the pediatricians recommend to use it constantly or infrequently, basically for dietary effort and/or if the mother cannot breastfeed (Table 4). 28.57% of the pediatricians recommend adding dietary complements to milk, but no one reported that they indicate the addition of sugar in baby bottle milk. In relation to nipples, 72.55% of the pediatricians recommend using special nipples, compatible to the child age and the kind of food to be swallowed, while 68.62% indicate orthodontic pacifier nipple. There is a narrow relationship between diet and caries, but the cariogenicity of the most common baby bottle contents, namely milk and milk formulas, remains unclear13. Bovine milk contains the disaccharide lactose at the concentration of about 4%, and human milk contains about 7% lactose. Although human breast milk contains more lactose than bovine milk, the difference is not significant in terms of cariogenicity14. Under extreme conditions or at very high concentrations of lactose, laboratory studies have shown that lactose can demineralize dental hard tissues14. However, in vitro studies have shown that while bovine milk supports bacteria growth, it has a greater buffering capacity than infant formulas, which may contribute to its anti-cariogenic properties15. In summary, there are different types of infant formulas available and some formulations may support the caries process13,16. It is in the childhood that good hygiene habits will be acquired, which will accomplish the individual for the whole life. And this disregard with oral hygiene is exactly one of the main liable for appearing rampant or baby bottle caries. Nevertheless, 26.31% of the pediatricians guide their patients to start oral hygiene just when the first tooth erupts or from the first year of life, showing us that they do not know the necessity of cleansing the gingival mats and the facility to deal with early age children as concern to use the toothbrush later. According to Paiva et al.2, from the 57 pediatricians interviewed, 18 (31.6%) prescribe calcium. This prescription is more common (33.3%) in the six months of age, and 22.8% of the pediatricians still prescribe systemic fluoride. In our work, 50.98% prescribe calcium constantly or in specific situations, and 17.64% prescribe fluoride use (Table 4). We must remember that fluoride dosages prescribed should be adjusted to fluoride content in supplying water, and that in the case of both cities involved in the research, fluoride content is enough and adequate, and do not need supplementation. Miller and Resenstein17 point that the main pediatrician activities when dealing with preventive dental health in children are: evaluation, instruction, fluoride prescription and guiding. The contents of these activities are related to caries, periodontal disease, malocclusion and dental trauma. When interviewing 250 pediatricians in Italy, Faletto et al.18 observed that 65.6% of the pediatricians consider dietary guidance helpful in caries prevention, 59.4% found dental floss usage relevant, 50% recommend fluoride supplements, and 42.2% found supplying water fluoridation important. However, just 34.4% believed in the benefits of fluoridated dentifrices and only 4.7% had knowledge of the fluoride over dosage risks. Most pediatricians (80.39%) perform routine exam on the child teeth (most commonly in the cases of caring in private clinic _ Table 4). 96% recommend the first visit to a pedodontist from six months or after teeth eruption, while just 3.92% recommended it before 6 months of age, most of the time to guide cleansing and maintenance of oral health. However, just 49% present a trustful pedodontist to refer their patients, and 84% of them work in private clinics or offices, evidencing how difficulty is to establish an interaction with public service and dentistry area professionals. Although our study revealed that the guidance given by pediatricians to their patients depend on where they exercise their profession (public service or private clinic), the results did not shown a positive correlation between knowledge level about oral health and clinical conduct. In conclusion, based on the results obtained, we can conclude that:1) Most evaluated pediatricians (78,3%) have presented an adequate or regular knowledge level about oral health; 2) Although the numbers of adequate knowledge level were representative, most of pediatricians did not know important aspects about oral health like: the breast milk cariogenicity, the transmissibility of caries and the appropriated age to remove a non-nutritive sucking habit; 3) Pediatricians that work in private clinic tend to have a better clinical conduct, although pediatricians who work exclusively in public service shown better knowledge about oral health promotion; 4) In general, there was not a positive correlation between knowledge level about oral health and clinical application of this knowledge; 5) Pediatricians’ knowledge about oral health can and must be improved, provided that there is more integration with dentistry area, especially when doctors are still in Graduation or Post-graduation. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}