 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
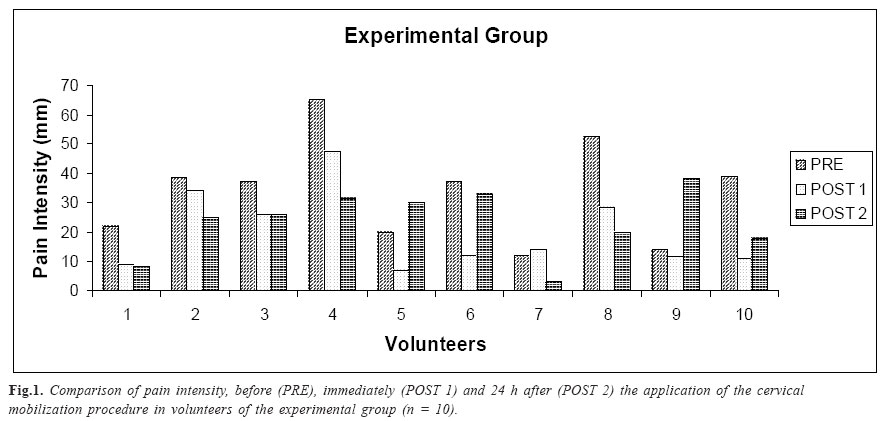
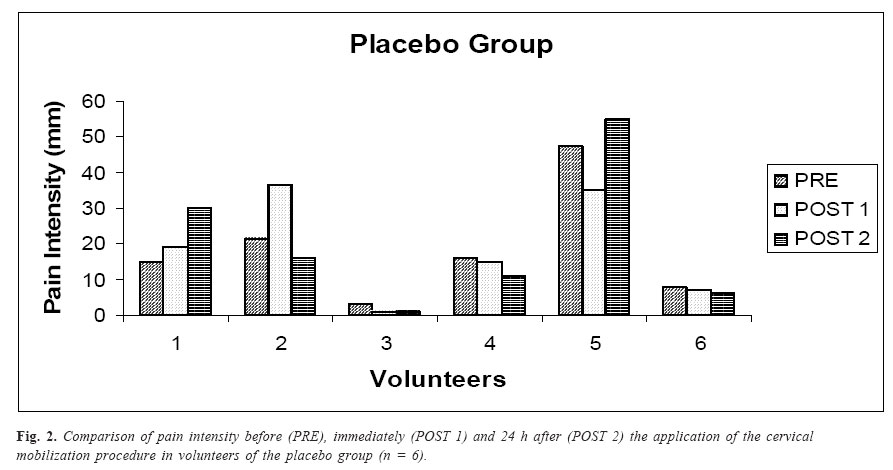
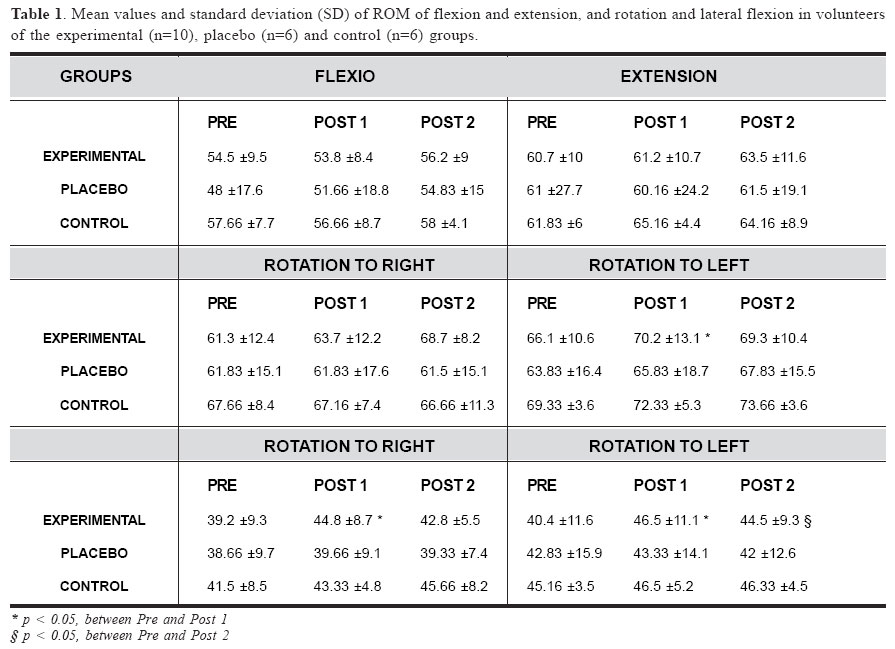
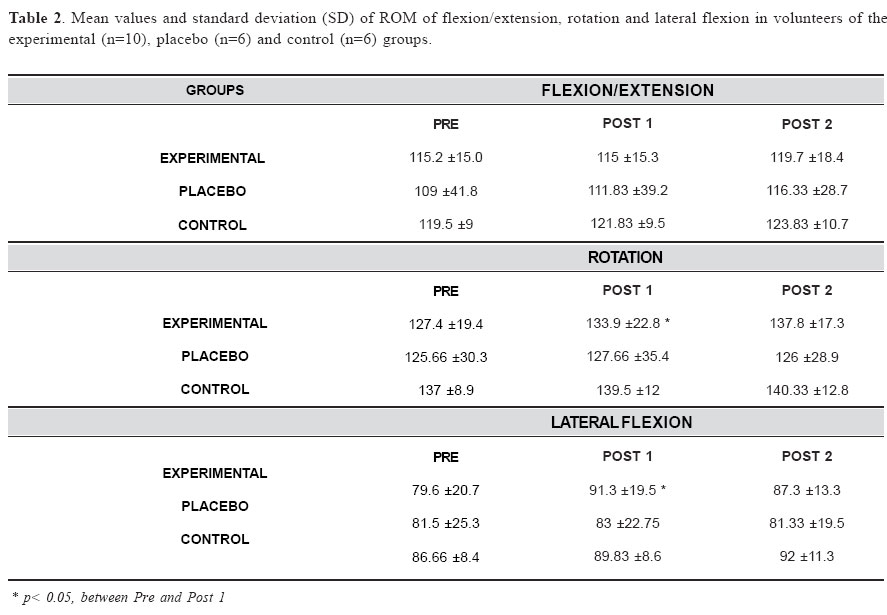
Brazilian Journal of Oral Sciences, Vol. 4, No. 15, Oct./Dec. 2005, pp. 911-918 Immediate effect of cervical mobilization in temporomandibular disorder patients Cristiane Rodrigues Pedroni 1 Anamaria Siriani de Oliveira 2 Fausto Bérzin 1 1Department of Morphology, University of Campinas – Piracicaba Dental School - Brazil 2Department of Biomechanics, Medicine and Rehabilitation of Locomotor Apparatus, Ribeirão Preto School of Medicine, University of São Paulo – USP Correspondence to: Cristiane Rodrigues Pedroni Faculdade de Odontologia de Piracicaba -Departamento de Morfologia Avenida Limeira, 901 - Bairro Areião CEP. 13414-903 – Piracicaba – SP Phone: (19) 3412-5336 E-mail: pedronicr@uol.com.br Received for publication: April 05, 2005 Code Number: os05039 Abstract The aim of this study was to assess the immediate effect of cervical mobilization on pain intensity and cervical range of motion in patients with temporomandibular dysfunction (TMD). Twenty-two volunteers, all females, participated in this study. The experimental and placebo groups were comprised of TMD patients with rotation at least one of the three first cervical vertebrae observed by radiographic examination, while the control group was comprised of TMD-free subjects without cervical vertebrae rotation. The results showed that there was a significant decrease in pain intensity and a significant increase in rotation and lateral flexion range of motion of volunteers of experimental group immediately after application of the cervical mobilization procedure. However, all these effects were of short duration. Key Words: mobilization, cervical spine, temporomandibular disorder, pain IntroductionMany studies related to temporomandibular dysfunction (TMD) point to an anatomical and functional interaction between the stomatognathic system and the cervical spine, confirming that pain symptoms of the stomatognathic system can also be related to the cervical spine disorders and vice versa1-2. The high prevalence of craniocervical disturbances in TMD patients, especially those with muscle involvement, is usually attributed to the neurophysiological interactions and biomechanical relations between the cervical segment and the stomatognathic system. Various authors have been showing evidences of a greater number of signs and symptoms of the cervical dysfunction in TMD patients than in volunteers without TMD, mainly in relation to tenderness of cervical muscles and functional limitation of the cervical spine1,3-9. Stomatognathic and cervical systems should be considered functionally as one. The abnormal function of the muscles and joints of the cervical region can be a probable cause for the greater frequency of pain in the orofacial region10, due to the functional relation between Temporomandibular Joint (TMJ) and the craniocervical regions, where movements of the atlanto-occipital joint and cervical vertebrae occur concomitantly with the activation of masticatory muscles and jaw movements. Therefore, injury or alterations of head posture could lead to the disruption of motor control of this region, compromising the normal mandibular function2. Although most of the authors considers cervical mobilization an important treatment form in patients with articular dysfunction, there have been few randomized and controlled studies evaluating the efficacy of these procedures11. Therefore, additional studies are needed to determine if cervical mobilization is an effective therapy, especially in relation to TMD patients. In general, articular mobilization techniques have been applied in the attempt of reducing the pain and to increase the joint cervical mobility. It has been published reports of studies utilizing cervical mobilization in the treatment of TMD. However, this technique has often been combined with other treatments such as massotherapy, thermotherapy and relaxation12-13, which would not influence specific effects observed with cervical mobilization. The aim of this study was to determine the effects of cervical mobilization in TMD patients from the data obtained in the measurement of the cervical range of motion and determination of pain intensity, before and after the procedure. Matherial and MethodsVolunteers This study involved 22 female volunteers, aged 18 to 40 years (x = 24.3 ±7.1), divided into 3 groups: an experimental group, comprised of 10 subjects, a placebo and a control group both comprised of 6 subjects. All subjects volunteering for this study signed an institutional review board approved consent form after the testing procedures were verbally described to them. The subjects of the experimental and placebo groups were presented with myogenic TMD, who had pain in the masticatory muscles during functional activities (speaking and eating), occlusal parafunction and/or in accordance with muscular fatigue. In addition, to be selected, all the volunteers had to show evidence of rotation of at least one of first three cervical vertebrae upon radiographic examination and report of pain at the moment of evaluation. The control group was comprised of subjects with no dysfunction and who have not rotation of any of the of the upper cervical spine vertebrae. None of the volunteers was using analgesic; there was not any evidence of contraindications for the application of cervical mobilization. X-ray ExaminationThe radiographic examinations were performed with the purpose of confirming a diagnosis of vertebral rotation of the cervical spine by the transoral approach. A GE 1000 X-ray equipament was set for an exposure of 21 impulses, 68 kvp and 10 mA, using an intensifying screen. The volunteer remained seated with the mouth opened fully and, the posterior region of the head was completely laying down in the chassis, which was attached to the wall by a support. For the X-ray examination, the head was extended 10º relative to the Frankfurt plane. The film-focus distance was 70cm and the central ray passing through the labial commissure. The X-ray examinations of the volunteers were analyzed considering the alignment between the spinous processes in relation to the midline of the center of the cranium14. The X-ray examination also permitted a Grostic radiographic analysis in relation to manipulation therapy of the cervical spine15-17. Rotation was visualized by the use of an upper angle, which is the acute angle formed by the intersection of the line of the atlas plane and central line of the cranium. In selecting the 16 volunteers with TMD, who fulfilled the criteria in relation to vertebral rotation, it was necessary to exclude from the sample 3 volunteers (18.75%) who did not show vertebral rotation. Only one of the volunteers (16.66%) classified previously as TMD-free showed rotation of the cervical vertebrae and was excluded from the sample. Although the number of subjects in the control group (n = 6) was smaller than the number of volunteers with TMD (n = 16), this observation suggests that the cervical vertebrae rotation is more frequent in patients with TMD than in those without the dysfunction. ProceduresAfter the X-ray examination, the selected volunteers were submitted to an evaluation of active mobility of the cervical spine and of the pain intensity. Cervical mobilization was then applied in volunteers of the experimental and control groups and a simulation of the technique was accomplished in the placebo group. A re-evaluation of the cervical spine range of motion and pain intensity was performed immediately after the application of the technique, with another re-evaluation 24 h after the experiment. The volunteers of the control group were not evaluated as the pain intensity, since they did not show any pain. Cervical spine range of motion was evaluated during the neck movements of flexion, extension and rotation and lateral flexion to right and left. A fleximeter from the Code Instutite of Research® was utilized for these measurements. Pain intensity was determined by means of a visual analog scale (VAS). So that the responses would not be induced, the volunteers did not have access to any of their previous responses. Cervical mobilizationVolunteers were divided into experimental and placebo groups by sorting were blinded to the nature of the procedure (simulation or real treatment). Cervical mobilization technique employed in this investigation was a longitudinal movement described by Corrigan and Maitland18. The application duration was one minute for twice and a 3 minutes interval between repetitions. The placebo group received a simulation of the cervical mobilization technique in which the volunteer and the operator remained in the same position, abiding by the same duration and interval as in the therapy utilized in the experimental group, although the combination of longitudinal and oscillatory movement was not employed. Statistical AnalysisThe paired, non-parametric Wilcoxon test was utilized, considering the level of significance at 5% (p<0.05), to compare the values for pain intensity and cervical range of motion amplitude at the three times of evaluation, that is before (PRE-evaluation), immediately after (POST 1-evaluation) and 24 h after (POST 2-evaluation) the cervical mobilization procedure in each group separately. ResultsPain intensity Pain intensity, obtained by the use of VAS, in the experimental group showed evidence of a statistically significant reduction of pain intensity when comparing measurements of PRE and POST 1 evaluations, while there were no significant changes for measurements between PRE and POST 2 evaluations, and between POST 1 and POST 2 evaluations (Fig. 1). In the placebo group there were no statistically significant difference for any of the periods of evaluations studied (Fig.2). Cervical mobility Regarding to cervical range of motion values for the experimental group, there was a statistically significant increase in ROM for rotation to left and lateral flexion to left and right, between PRE and POST 1 evaluations, and for lateral flexion to left between PRE and POST 2 evaluations. In the placebo and control groups, there was no statistically significant difference for any of the movements evaluated. Table 1 shows the mean values for cervical ROM observed in the three groups studied. When analyzing the total cervical range of motion for each movement studied, a significant increase in cervical range of motion for rotation and lateral flexion in the experimental group, between PRE and POST 1 evaluation was observed, as shown in Table 2. DiscussionA statistically significant increase in cervical range of motion values was observed only in the experimental group, for rotation to left and lateral flexion to left and right when examining unilateral movements, and a significant increase in rotation and lateral flexion when considering the complete range of motion in the three planes examined. These results are in concordance with the majority of studies about manual therapy19-21 and cervical mobilization in patients with articular TMD22-26, which confirm an increase in range of motion after application of the techniques. This increase in cervical range of motion can be explained physiologically by the action of the procedure on contractile and non contractile structures surrounding the vertebrae, resulting in a muscular relaxation reflex27 and consequently in a tendency toward equilibration of contractions, bilaterally, re-establishing or leading to a normal range of motion. Another effect of the cervical mobilization technique employed that could explain the increase cervical range of motion is the decrease in the internal pressure of articulations attained by longitudinal traction, which allows an influx of synovial fluid responsible for articular lubrication28. In addition, oscillatory manual techniques, such as that evaluated in the present study, could be utilized to guide tissue remodeling, interconnecting new collagen fibers and consequently improving the extensibility and lengthening of the tissue, as well as articular mobility21. Although, it can not be certain that this remodeling occurred with only a single session of treatment. It is very probable that the proposed treatment acts in the plastic phase of tissue deformation, that is, some time after the external force has been stopped and the distended tissue recovers its initial structural characteristics29. This could explain cervical range of motion gain immediately after the cervical mobilization procedure (POST 1) and the loss of this additional range observed in the second re-evaluation (POST 2). Another important aspect that should be considered is the capacity of the cervical mobilization to activate type I articular mechanoreceptors. These are low-threshold, slow adapting receptors, which responds to very small mechanical stresses and continues to send out nerve impulses for the duration of the mechanical stimulus. Their function includes the signaling of the direction, range and velocity of articular movements, produced actively or passively, and the regulation of changes in articular pressure. Significant contributions to kinetic and postural sensation and to facilitation of the central nervous system in regulating postural and muscular tonus during articular movement30. The stimulation of these mechanoreceptors caused by cervical mobilization should have therefore contributed to the gain in range of motion observed in this study. Some alternative explanations for the correlation between the restoration of articular movement and the reduction in the pain intensity has been described in the literature related to cervical vertebral mobilization. It is suggested that the stimulation of type I mechanoreceptors may inhibit the flow of nociceptive afferent activity that runs through the type IV articular receptor system. This receptor, found in the articular capsule, is an inactive nociceptor under normal conditions, becoming active only when articular tissues, which contain this type of nerve terminus, are submitted to extensive mechanical deformation or chemical irritation30. The inhibitory effect of type I articular receptors on type IV nociceptive receptors is one of the factors described in the literature as being responsible for the reduction of the pain intensity in patients treated with manipulation or articular mobilization in general30 and cervical mobilization31. In addition to the functions described, type I mechanoreceptors produces an inhibitory effect on the pain at the level of the spinal cord, in a manner similar to that described in the “Gate Control Theory”31. Pain impulses that reach the dorsal root ganglion, synapse in the dorsal horn with their fibers terminating predominantly in the gelatinous substance, which in the case of the C1 to C3 cervical segments is homologous to the caudal nucleus of the trigeminal nerve32-33. The gate is closed to the ascendance of pain impulses by action potentials originating from type I mechanoreceptors (fast, myelinated fibers), which are preferentially stimulated by manual vertebral therapy techniques34. Knutson and Jacob17 (1999) utilized manipulation of the cervical spine combined with other procedures to reduce the pain in patients with TMD. The beneficial and alleviating effects on symptoms were associated with observed changes in X-ray examination pre and post-treatment. The realignment of the cervical spine was accompanied by improvement regarding to symptoms, while a new rotational misalignment of the first cervical vertebra was seen after relapse of TMD. Results of pain intensity values obtained showed a statistically significant decrease only in the experimental group, just after the administration of the cervical mobilization technique. These results are in concordance with authors who support the analgesic effect of manual therapy in general11,19-21,35, as well as with those who attribute this effect specifically to cervical mobilization therapy of the spine vertebra11,36. Although, no significant reduction in the pain intensity was seen in the experimental group, 80% of the volunteers in that group at 24 h after treatment presented with a pain intensity less than reported before initial phase of the experimental procedure (pre cervical mobilization). The most volunteers in this group (60%) continued to report lower pain intensity at POST 2 than at POST 1 evaluations (60%) (Fig. 1), albeit with a tendency toward exceeding initial levels. It suggests that although there was an effect on the pain intensity, it be of short duration. The same behavior was observed for 50% of the volunteers of the placebo group (Fig. 2). Although it was not statistically significant in any of the situations studied, the pain intensity reduction for some of the volunteers of this group could be explained by spontaneous improvement as well as by the behavior of the volunteer with a tendency to be agreeable to the examiner. No reports were found in the literature dealing with a randomized and controlled study aimed at determining the effect of single treatment modality in patients with clinically homogeneous characteristics, which could be used for comparison of data. Besides, the most studies utilized cervical mobilization combined with other therapeutic modalities, difficulting the conclusions regard to the effectiveness of the technique alone. Further studies in TMD patients are needed to confirm these findings. It is likely that the experimental groups with a greater number of volunteers and a greater frequency and duration of treatment, reaffirm or point out other effects of he cervical mobilization technique cervical range of motion in TMD patients. In conclusions: 1. The cervical mobilization therapy used was able of producing an immediate pain reduction in TMD patients and with rotation of the cervical spine, and an immediate increase cervical mobility, shown by the neuroanatomical and biomechanical interaction between the cervical spine and craniocervical structures; 2. The effects on pain intensity and cervical mobility of the cervical spine were short lasting, since signs and symptoms returned upon examination 24 h after application of the technique. This indicates that cervical mobilization can be an alternative treatment to obtain rapid alleviation of the signs and symptoms of TMD, but that the frequency of treatment needs to be more than every 24 h; 3. Rotation of the cervical vertebrae may be a common alteration among TMD patients, showing the need for alleviation and treatment of the cervical spine alterations. AcknowledgementAcknowledgements to the Fundação de Amparo à Pesquisa do Estado de São Paulo - FAPESP for the financial support of this work (Process nº 01/04253-3 and 01/08505-7R) References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}