 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
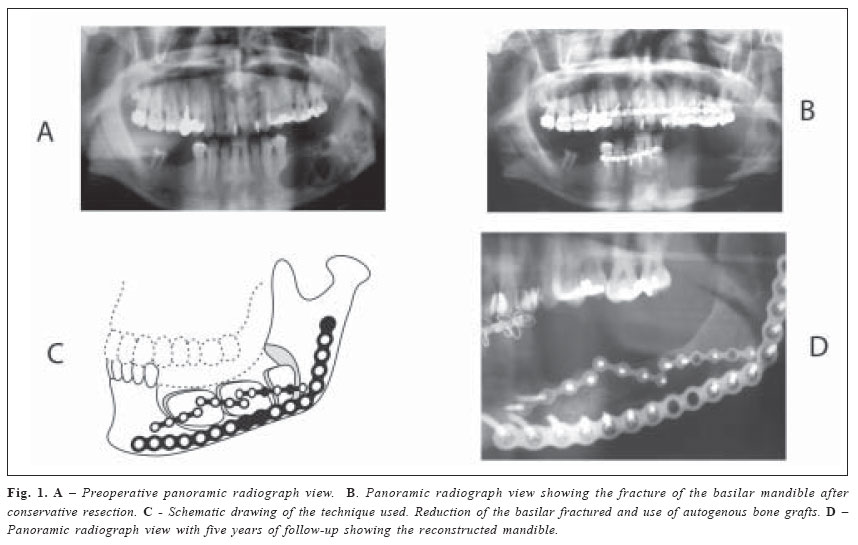
Brazilian Journal of Oral Sciences, Vol. 4, No. 15, Oct./Dec. 2005, pp. 929-931 Management of mandibular basilarfracture as a complication of tumor surgery Sergio Monteiro Lima Junior1 Bruno Ramos Chrcanovic1 Leonardo Gomes1 Leandro Napier Souza 2 Ricardo Santiago Gomez 3 Belini Freire-Maia 4 1DDS,Oral and maxillofacial surgery resident. 2DDS, MS, Oral and maxillofacial surgeon; Professor, Universitary Center Newton Paiva, Belo Horizonte, Minas Gerais, Brazil. 3DDS, MS, PhD, Professor, Clinic, Pathology and Surgery Department , Federal University of Minas Gerais, Belo Horizonte, Brazil. 4DDS, MS, Oral and maxillofacial surgeon of FHEMIG; Professor, Catholic University of Minas Gerais, Belo Horizonte, Brazil. Correspondence to: Belini Freire Maia Av. contorno 4747, conjunto 1011, Bairro Serra. CEP: 30110-090 Belo Horizonte – MG - Brazil Phone: 00 55 31 99843817 Fax: 00 55 31 3281-3817 E-mail: belini@lifecenter.com.br Received for publication: September 30, 2005 Code Number: os05042 Abstract Fracture of the mandible basilar bone after a conservative resection of an ameloblastoma is an unusual postoperative complication and poorly cited in literature, since the radical resection is the most common treatment used for this condition. We present a case dealing with this complication, showing a technique for mandibular reconstruction that creates good results in five years of follow-up. Key Words: mandibular, fracture, tumor surgery Introduction Many techniques have been developed for reconstruction of mandibular defects created by tumor surgery, trauma or infection. These include autogenous bone graft, pedicle bone grafts, homologous bone grafts1, and more recently platelet rich plasma to improve bone healing2. Vascularized bone grafts have become the preferred method of mandibular reconstruction, but this technique is considered to increase both the operating time and blood loss, which might be associated with an increased morbidity and mortality3. Although many approaches were developed during the last fifty years, the use of autogenous bone graft for mandibular reconstruction is still a standard technique4. The following report describes a technique using autogenous bone for bridging a mandibular defect after fracture in the remaining basilar bone submitted to a conservative resection to treat an ameloblastoma. The complication occurred one month after tumor resection and the mandible was divided into two pieces with poor contact. After reduction and fixation, a bone graft was performed. To achieve primary intraoperative anatomic alignment and stable fixation of the graft, after the removal of the iliac bone, it was divided in small blocks. This complication and its management are poorly cited in literature, even the conservative resection for this case could be questioned because the treatment employed to this condition is usually a radical resection. Clinical CaseOne month after a conservative resection for an ameloblastoma (Fig. 1A), the mandible basilar remaining bone has fractured (Fig. 1B), although the patient was under maxillomandibular fixation since surgery. In a second time surgery, the basilar bone was reduced using a 2.7 mm plate, to achieve facial harmony and function. The cortical and cancellous cellular bone were harvested from the iliac crest and stored in a saline solution. The cortical graft is divided in three blocks using a reciprocating saw and continuous saline irrigation. The cortical bone is contoured to adapt to the recipient site and grafting was performed (Fig. 1C). Rigid fixation with mini-plates 2.0 and screws were used to maintain the blocks on the previous position. The spaces between the blocks are filled with cancellous cellular bone, reshaping mandibular body and alveolar ridge. After five years of follow up, no tumor recurrence was seen. Radiographic controls showed no graft resorption and the bone volume was maintained since reconstructive surgery (Fig 1D). DiscussionDespite the option for treatment this case of ameloblastoma with a conservative resection indeed a radical resection, some authors discussed this postoperative complication in their texts5-6 and a few attention is given to the management of this type of mandibular fracture. Curi et al5 treated this complication with intermaxillary fixation, but neither intermaxillary fixation nor open reduction and functionally stable fixation would not improve the patient health, because the area of contact at the fracture site was minimal and a spontaneous bone fracture and displacement occurred. Some authors recommended ameloblastoma resection and immediate reconstruction7, but the use of plates to maintenance of anatomic area for future reconstruction is an option due to possibility of recurrence8. The great challenge of this case was to favour basilar bone healing and correct alignment and improve bone volume, all in a second time surgery. The division of cortical iliac bone in smaller blocks obviously increases the contact surface, and so more cancellous bone could be inserted in the recipient site. An advantage of this technique is that graft rotation or malposition was avoided and cancellous cellular grafts allow appropriate reconstruction of the mandible4. Successful criteria defined by August et al9 were achieved in five years of follow up: closed wound, freedom of infection, bony continuity, stability and maintenance of osseous bulk. The relative amount of displacement of the fractured segment is obviously a determining factor since conservative management is a realistic option. A grossly displaced edentulous mandible fracture is not treatable with conservative treatment and an open reduction and internal fixation followed by reconstruction is required. The open technique offered the advantage of autogenous bone grafting with minimal increased morbidity and produced an excellent result in five years of follow-up. No recurrence was observed on this follow-up period and a rehabilitation treatment is under consideration using prostheses or osseointegrated implants. AcknowledgementsSupported by grants of FHEMIG (Fundação Hospitalar do Estado de Minas Gerais) References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}