 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
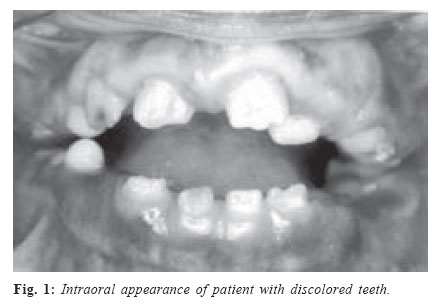
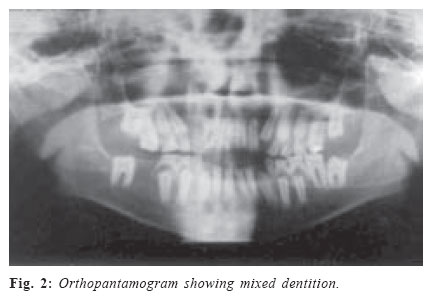
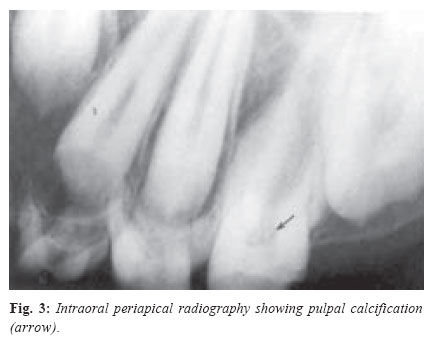
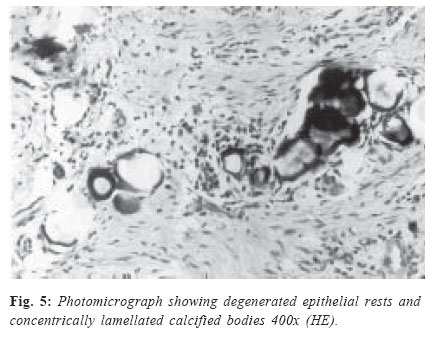
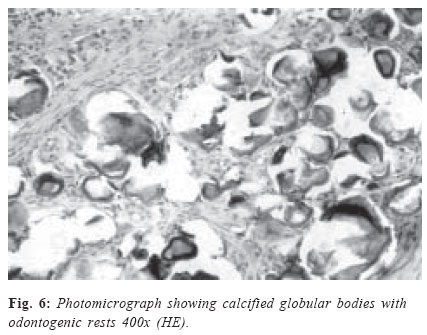
Brazilian Journal of Oral Sciences, Vol. 4, No. 15, Oct./Dec. 2005, pp. 932-935 Amelogenesis imperfecta with gingival calcification: a rare presentation Sunitha Carnelio1 Nirmala Rao1 1MDS -Department Of Oral And Maxillofacial Pathology - Manipal College Of Dental Sciences - Manipal, Karnataka, India. Received for publication: October 11, 2005 Code Number: os05043 Abstract The purpose of this article is to highlight the rare presence of gingival calcification with Amelogenesis Imperfecta. A case is presented of a 12-year-old girl with a defect of enamel in deciduous as well as permanent dentition with moderate amount of gingival hyperplasia with no positive family history of a similar condition. On the basis of history, clinical and radiographic features a diagnosis of autosomal recessive hypoplastic amelogenesis imperfecta of rough variant was made. Histopathological examination of hyperplastic gingival tissue revealed the presence of calcified bodies. An attempt is made to determine the nature of these calcified bodies by histochemical examination. The relevant literature is reviewed. Key Words: amelogenesis imperfecta, gingival, enamel, hyperplasia, calcification IntroductionAmelogenesis Imperfecta (AI) is a group of hereditary developmental defects of tooth enamel. It is mainly an autosomal dominant disease, but autosomal recessive, X-linked and sporadic cases also do occur. The possible abnormalities include hypoplasia, hypomaturation and hypocalcification of the tooth enamel or combination of these. Both primary and secondary dentitions are affected. A few reports on autosomal recessive nature of the rough variant hypoplastic type of AI are present in the literature1,2. The unique clinical feature of this patient was the presence of a few deciduous teeth, few partially erupted permanent teeth, showing features of AI with pulp stones and hyperplastic gingiva of moderate intensity. Histopathological examination of the hyperplastic tissue revealed the presence of calcified bodies in the connective tissue. The nature and the probable cause of these calcified bodies has been discussed. Clinical CaseA 12-year-old girl was seen for the chief complaint of discolored teeth. There was no history of any drug intake or systemic disease. No evidence of a similar condition could be elicited in the family history. The extraoral examination was unremarkable. On intraoral examination, the deciduous and permanent teeth that were present had a distinct yellow color with an irregular, but hard surface. The teeth were widely spaced with a moderate amount of gingival hyperplasia (Fig. 1). The teeth present were deciduous maxillary first and second molars, deciduous mandibular canines, first and second molars, partially erupted permanent maxillary central and lateral incisors, mandibular central and lateral incisors and permanent molars. The mandibular permanent right molars were missing. The deciduous as well as permanent molars were attrited. Radiographic examination revealed enamel hypoplasia of both affected primary and permanent teeth, together with delayed or arrested eruption of other permanent teeth. Lower right mandibular molar was missing. The crown and root of the teeth appeared to be developing normally in outline. It was difficult to differentiate enamel from dentin (Fig. 2). Pulpal calcifications were evident in the coronal portion of the teeth (Fig. 3). The hyperplastic gingival tissue was sent for histopathological examination, which showed small, round to ovoid basophilic masses with few odontogenic rests in a chronically inflamed connective tissue stroma, with dense proliferating fibroblasts. The epithelium was lined by parakeratinized stratified squamous epithelium, acanthotic at places (Figs. 4, 5 and 6). Further, various special stains like Periodic Acid Schiff (PAS), Van Gieson, von Kossa and Congo Red were performed, and was found to be positive for PAS, Van Gieson and von Kossa but negative for Congo Red. DiscussionAI may be isolated or associated with syndromes like otodental and Morquito syndrome, amelocerebrohypohi-drotic, ameloonychohypohidrotic, trichodentoosseous, dystrophic epidermolysis bullosa, oculodentoosseous dysplasia, pseudohypoparathyroidism, tuberous sclerosis and vitamin D – dependent rickets. None of these conditions is associated with extra dental anomalies3-4. The autosomal dominant hypocalcified type is the most common form of AI, followed by hypomaturation and hypoplastic types5. The enamel is of normal thickness, but opaque or yellowish white without luster on newly erupted teeth showing hypocalcification. It is so soft that is lost soon after eruption, resulting in a crown composed only of yellowish dentin. The enamel can easily be scraped from the tooth. The prevalence of this condition is said to be 1:4000. On the basis of clinical criteria, AI has been subdivided into hypoplastic and hypopcalcificated varieties6. Witkop7 coined the term ‘hypomaturation’, to describe less severe degrees of enamel hypocalcification. Witkop and Sauk8 described six types of hypoplastic AI based on the clinical, histological as well as the mode of inheritance. This case represented an unusual and rare form of rough hypoplastic type of AI with autosomal recessive inheritance, which could be compared with the reports of Catena and coworkers9, Frank and Bolender10, Witkop and Sauk8 and Chosack and colleagues11, although differing somewhat, represent other examples in this category. The parents of this patient, her siblings or relatives had no such similar condition (AI) and thus her parents could be accepted as heterozygous carriers of a recessive gene, which determines AI. Being a sporadic case with a new mutation is another possible alternative. Studies have also shown that recessive cases are more severe than the dominant ones2. Generalized gingival enlargement may be due to a variety of causes, including inflammation, leukemic infiltration and chemical induction, as seen with drugs like phenytoin, cyclosporine or nifedipine. These must be ruled out; however, the degree of enlargement is typically less and the texture soft than that of the gingiva observed in this case12. Also there was no positive history of any of these. A feature to be noted in this case was gingival hyperplasia with lack of complete eruption of permanent teeth, though radiographically, well-formed roots of permanent teeth were seen. Normally, the connective tissue covering the tooth crown atrophies when the tooth erupts toward the oral epithelium. It can be assumed that the presence of an epithelial covering of the crown is necessary to bring about this atrophy of the tissue. A lack of epithelial covering may even lead to proliferation of the connective tissue so that the moving tooth covered with mucosa, bulges into the oral cavity. This loss of protective epithelial covering brings the connective tissue into contact with the enamel and may produce hyperplastic gingiva6. Since this patient did not have any history of drug intake, or a manifestation of genetic disorder, this may be attributed to dental follicles unable to synthesize the factor that initiate eruption, or a lack of epithelial covering which brings the connective tissue in contact with the enamel producing hyperplastic gingiva. The most interesting finding in this case was the presence of gingival and pulpal calcification. Ectopic calcification has been reported in patients with disorders of calcium and phosphorous metabolism13. In addition, calcinosis of different tissues and organs have been presented with familial, neoplastic, idiopathic and other etiologies14. But in this patient, serum levels of calcium and phosphorous were within normal limits, with the absence of any of the above mentioned etiologies. These calcifications, previously referred as ‘enameloid conglomerates’, have been described in several types of AI and also in odontodysplasia2. These were previously considered to represent the mineralization of rests of odontogenic epithelium and areas of dystrophic calcification. Studies by various authors disagree with the interpretations made by the previous authors and they suggest that the presence of rests of odontogenic epithelium may indicate a mechanism of induction associated with these epithelial elements15-16. Paynter and Pudy17 have shown that afibrillar cementum stains yellow with Van Gieson, as in our case. Ultrastructural observations of Gardener and Sapp18 indicated that there are two different types of bodies in odontodysplasia, one representing an aberrant form of afibrillar cementum and another representing fibrillar cementum and these were compared with the histochemical findings, which were consistent with our findings. Also, ectopic calcifications with a matrix of fine, densely packed branching fibers, somewhat resembling filamentous actin has been described in the gingiva of patients with AI19. Pulpal calcifications were also present in this case in a few deciduous and permanent teeth. As these occurred in impacted as well as in erupted teeth, they appeared not to be related to external irritation. Electron microscopy needs to be performed to determine the nature of these calcifications, but could not be done due to its unavailability. References
Copyright 2005 - Piracicaba Dental School - UNICAMP São Paulo - Brazil |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}