 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 5, No. 16, Jan - March, 2006, pp. 941-943 Enamel hypoplasia or amelogenesisimperfecta - a restorative approach Rodrigo Borges Fonseca1 Lourenço Correr Sobrinho2 Alfredo Júlio Fernandes Neto3 Adérito Soares da Mota3 Carlos José Soares4
1DDS, MS, Graduate student at Piracicaba Dental School,
State University of Campinas São Paulo, Brazil.
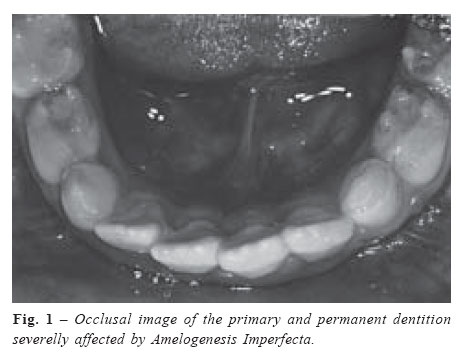
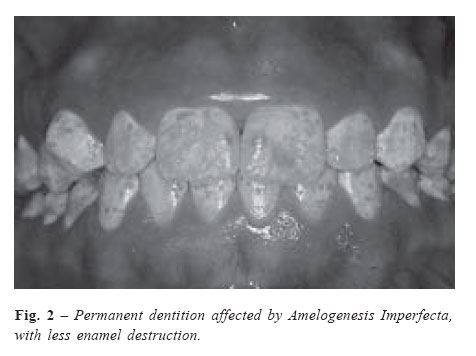
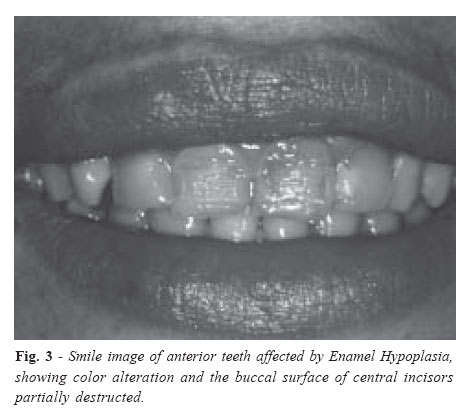
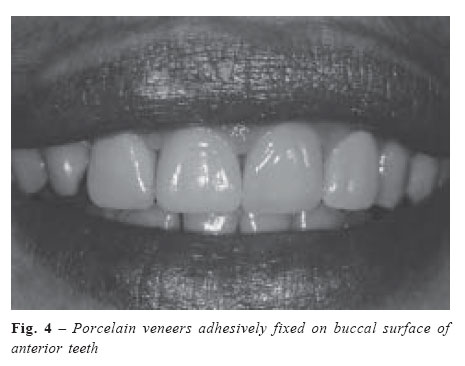
Received for publication: December 04, 2003 Code Number: os06002 Genetic or acquired disturbances may lead to the development of alterations on enamel structure, compromising tooth esthetics and function. This short communication aims to briefly discuss the possibility of employment of several treatment options either to – Enamel Hypoplasia or Amelogenesis Imperfecta in order to achieve optimally esthetic results. Key Words: amelogenesis imperfecta, enamel hypoplasia, treatment options Introduction In general practice many professionals do not know how to differentiate Enamel Hypoplasia from other enamel alterations, such as Amelogenesis Imperfecta. Enamel Hypoplasia or Amelogenesis Imperfecta can be considered an exclusive ectodermic disturbance which can cause white flecks, narrow horizontal bands, lines of pits, grooves, and discoloration of teeth varying from yellow to dark brown1-2. According to Alvares and Souza Freitas3, “this alteration is probably inhibitory in nature and causes atrophy and lack of function of ameloblastic cells, leaving as a result structural defects on enamel formation”. It is true that hypoplastic teeth are a characteristic of Amelogenesis Imperfecta, but the last is only related to genetic causes, autosomal dominant or recessive genes or X-linked, i.e. it is always hereditary, affecting all the teeth on both dentitions (Figures 1 and 2). Enamel Hypoplasia can be related either to hereditary causes, affecting all the teeth on both dentitions or acquired ones, involving one or more teeth (Figure 3). When Hypoplasia is related to a hereditary cause it can be also called Amelogenesis Imperfecta. According to the clinical findings amelogenesis imperfecta can be classified into four categories: type I, hypoplastic enamel (the most common one), type II, hypomaturated enamel, type III, hypocalcified enamel and type IV, hypomaturated-hypoplastic enamel with taurodontism4. Bonding to teeth with affected enamel has been done successfully5-9 but any esthetic restorative treatment should pay attention to the characteristics of each type of alteration. Type I is a result of a defect in the formation of the enamel matrix showing pits at the enamel surface or severely worn teeth with exposed discolored and sclerotic dentin. Type II is associated with the retention of 2-5% of the enamel matrix proteins compared to only 0.01-1% in normal enamel10, and clinically enamel tends to chip from the underlying dentin. Type III shows soft enamel due to a defect during mineralization and wear is common. Type IV is a combination of I and II. In less severe cases normal enamel can be found around the affected one; then adhesion procedures can be optimally performed5. The pretreatment with sodium hypoclorite can improve bond strength to hypocalcified enamel11 but if just affected enamel is present it is advisable to remove it and bonding should be tried in dentin, usually sclerotic. Reduced bonding efficacy has been documented in sclerotic dentin due to obliteration of dentinal tubules with sclerotic casts, the presence of an acid-resistant hypermineralised layer, and the presence of bacteria on the lesion surface12. In order to overcome these problems extending etching periods have been recommended for conventional adhesive systems13, while the application of acids is suggested prior to self-etching adhesives12. Tooth bleaching and microabrasion represent a first and minimally noninvasive step; after that, composite resin restorations can produce excellent esthetic results5, but in most severe cases, porcelain veneers appear to be the best option14. Enamel which is easily penetrated with an explorer is not a good candidate for microabrasion. Superficial brown and white discolorations on hypomaturated enamel can be easily removed by microabrasion7. As the treatment is headed to produce excellent esthetic results and stable clinical longevity, greater loss of tooth structure should be treated with more invasive procedures that are known to achieve best results5-6,8-9. As stated by Andrews et al.14, in most severe cases porcelain veneers appear to be the best option. This option is based on the fact that on most Enamel Hypoplasia cases the enamel loss exposes the dentin structure to the oral environment, resulting either on dentin loss or even in dentin pigmentation. Normally, this pigmentation is superficial and can be easily superposed by direct resin restoration. However, when pigmentation is more severe direct resin restorations may not conceal dentin discoloration. Also, when there is a greater loss of tooth structure, indirect restorations may provide better mechanical properties either to the tooth or to the restoration. The porcelain veneers cavity preparation to hypoplastic teeth is similar to non-hypoplastic teeth but usually crown lengthening by periodontal surgery is needed6. The professional should pay attention on the preparation design as it makes possible the manufacturation of a porcelain veneer with at least 1.5mm thickness. On this way, discolored dentin areas will be superposed by porcelain veneers, resulting on an esthetic and functional rehabilitation of the smile (Figure 4). There are a great number of alternatives for the treatment of hypoplastic teeth. This communication only states this possibility but helps the clinician to understand what can be used on each case. Analyzing the benefits and limitations of each technique the professional will be able to decide the best treatment plan. References
Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06002f3.jpg] [os06002f2.jpg] [os06002f4.jpg] [os06002f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}