 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 5, No. 16, Jan - March, 2006, pp. 982-984 An unusual cause of recurrent cheek abscess: a clinical case Ashwani Sethi1* Anup Sabherwal2* Sudeepta. K. Basu3* Deepika Sareen4* 1Senior resident 2Senior resident 3Junior resident 4Junior resident
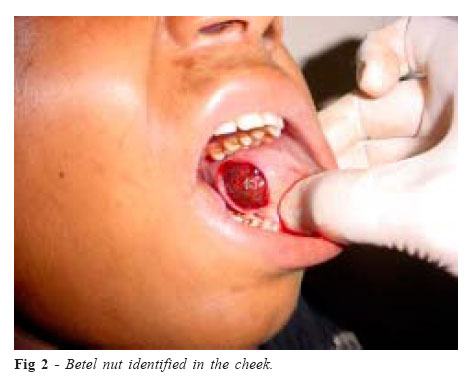
Received for publication: July 29, 2005 Code Number: os06010 Abstract We report the case of a 16-year-old female who presented to us with a recurrent cheek abscess following a blow to the cheek. On drainage of the abscess, a piece of betel nut was retrieved from the cheek. The patient recalled having a betel nut in her mouth at the time of the blow. Key Words: cheek, abscess, foreign body, betel nut Introduction Impaction of foreign bodies in the oral and paraoral region is not uncommon1. Most of the impacted foreign bodies are inorganic in nature with amalgam tattoo as the most common1-2. Most of the impacted foreign bodies are small in size and relatively inert in nature, thus, eliciting a very limited or no inflammatory response3. Impaction of a vegetative foreign body in the oral and paraoral tissues is rare and we encountered only one case4 of an impacted vegetative foreign body in the cheek with a resultant cheek abscess in the review of literature. The purpose of this report is to highlight the significance of a thorough history taking and keeping a high index of clinical suspicion for a probable foreign body when dealing with unusual abscesses in the head and neck. Clinical Case A 16-year-old female child presented to us with left-sided cheek swelling of 2 days duration. The patient gave history of having sustained a blow on left cheek around 2 weeks back from her father. It was followed by development of a similar swelling for which an intraoral incision was given with drainage of abscess by a practitioner in her village. She was apparently well for 10 days following that, when she developed a swelling again for which she had presented to us. On examination, the swelling was ill-defined, soft and tender situated submucosally in the left cheek anterior to the masseter muscle with a diffuse reactionary swelling involving the left half of the face (Figure 1). On aspiration, it was confirmed to be an abscess. The oral mucosa was apparently healthy. Routine blood and urine investigations were within normal limits. Pus culture revealed Staphylococcus Aureus. The patient was put on parenteral antibiotics in the form of ampicillin (50mg/kg/day) and gentamicin (4mg/kg/day) based on culture sensitivity report. The abscess was drained under local anaesthesia through an intraoral incision. At the time of incision and drainage, a piece of betel nut measuring 5mm.x5 mm. was retrieved from the left cheek (Figures 2 and 3). The patient later recalled of having a betel nut in the mouth at the time of sustaining the blow. The patient showed a complete response to the treatment and followed up for 8 weeks following the incision and drainage with no evidence of any recurrence of infection. Discussion The report presents an interesting and unusual case of recurrent cheek abscess as a result of impaction betel nut following a blunt trauma. Although, it is not uncommon for foreign bodies to be impacted in the oral and paraoral soft tissues1, most of the cases are asymptomatic because of the inert nature of the impacted foreign body3,5. Foreign bodies of vegetative nature may get lodged at various sites including ear, nose, bronchus etc., but, impaction in the oral soft tissues is rare with a very few cases reported in the literature4,6-8. Vegetative foreign bodies may induce an intense inflammatory reaction in the surrounding tissues and may get secondarily infected4 and the patient may also present with recurrent non-healing sinus in the oro-facial region7. Our patient sustained a blow to her cheek followed by the development of a recurrent cheek abscess. The presence of an impacted foreign body was not suspected, as there was no tooth loss as evidenced by history and examination. No specific questions pertaining to the possibility of an impacted foreign body were asked from the patient. It was indeed fortunate on our part to have retrieved the foreign body during the drainage of the abscess as we never suspected, and thus, never explored for a foreign body. On the other hand, in a case reported previously in literature, the patient underwent repeated incisions and drainage for recurrent cheek abscess5. Finally, an X-ray was done which revealed a foreign body in the cheek, which was removed and was found to be a pea with its shell. Both conventional and unconventional radiological techniques have been used in the localization of oro-facial foreign bodies5,8. In our patient no radiological investigation was sought as we did not suspect any foreign body impaction initially. Through this report, we attempt to alert the clinicians to consider an impacted foreign body as a cause of an abscess following trauma, especially if the abscess is recurrent. Learning points: References
Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06010f3.jpg] [os06010f1.jpg] [os06010f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}