 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 5, No. 16, Jan - March, 2006, pp. 985-990 Alternative esthetic and cost-effective therapy using a removable partialoverdenture for the treatment of a patientwith class III malocclusion Vinícius Carvalho Porto 1 Rodolfo Azevedo Branco Kazniakowski 2 Fernando Ribas Baggio 2 Paulo César Rodrigues Conti 1
1DDS, PhD - Professor, Department of Prosthodontics,
Faculty of Dentistry of Bauru, University of São Paulo, Brazil 2DDS
- Specialization students, Department of Prosthodontics, Faculty of Dentistry
of Bauru, University of São Paulo, Brazil
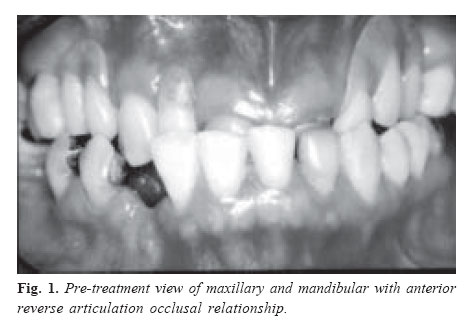
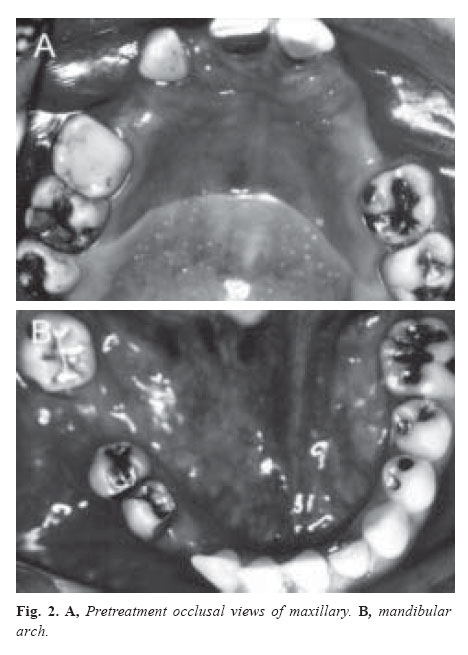
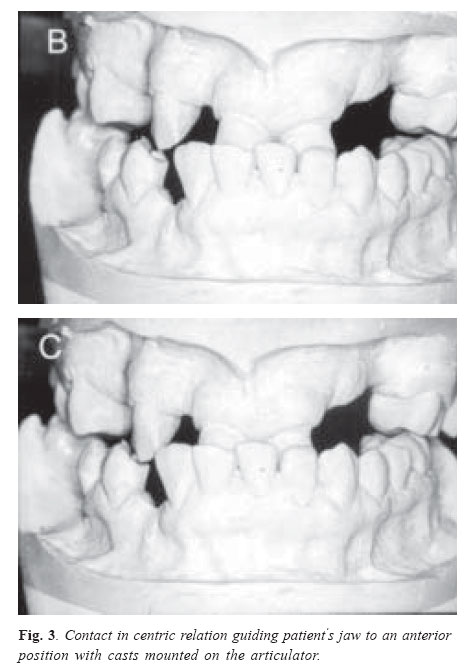
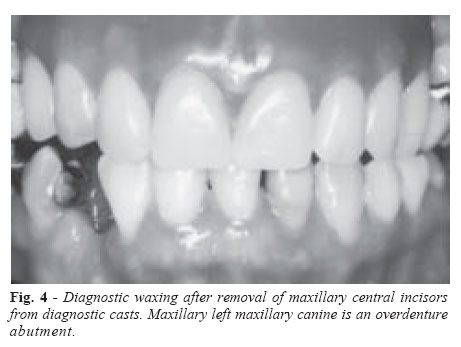
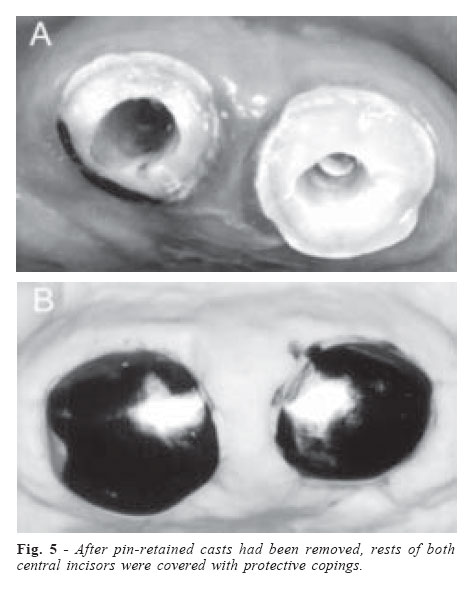
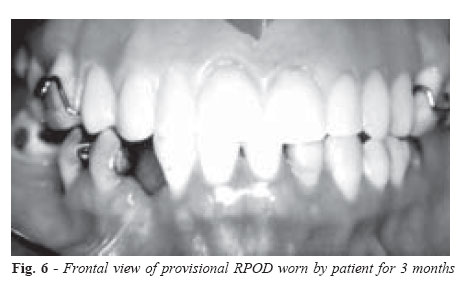
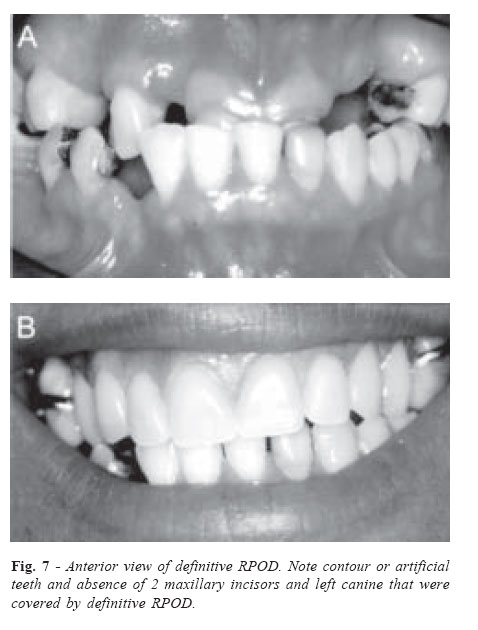
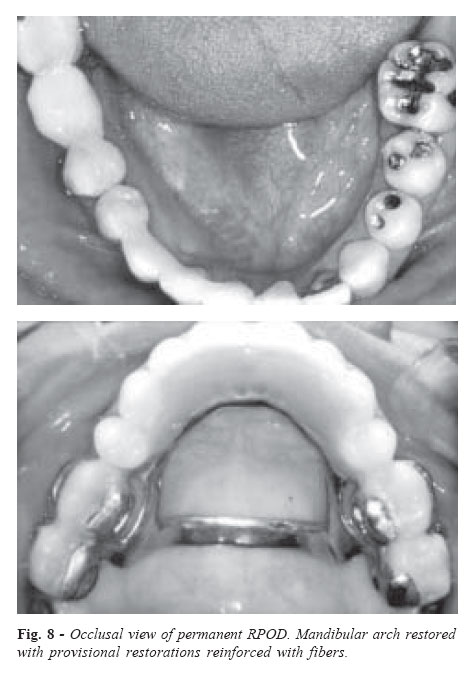
Received for publication: September 08, 2005 Code Number: os06011 Abstract This clinical case describes the treatment of a patient with an Angle class III malocclusion using an removable partial overdenture (RPOD). This treatment was selected as it was minimally invasive, had relatively low laboratory costs and was a simple technique. Clinical results were functionally and esthetically satisfactory. The treatment combined orthodontic and prosthodontic treatment, requiring few clinical appointments as compared to other therapies. Key Words: removable partial denture, overdenture, reverse articulation occlusal relationship, angle class III malocclusion, denture esthetic, denture base Introduction A reverse articulation occlusal relationship is classified as a Angle class III skeletal malocclusion1-2. For patients with class III malocclusion, maxillary archsize deficiency, maxillary retro-positioning, true mandibular excess, mandibular forward positioning, or any combination of these may be present3-8. Treatment including orthodontics and combined orthodontic/oral surgery may be indicated to correct this problem. Enacar et al.9 proposed face mask therapy with rigid anchorage for a patient with a class III skeletal relationship with maxillary hypoplasia and severe oligodontia. Gallagher et al.10 demonstrated that maxillary protrusion with a face mask produced a slight (<3 mm), but significant forward movement of the maxilla. Mcnamara5 and Turley11 showed that rapid maxillary expansion might also serve to disrupt the maxillary suture and enhance the protrusion effect of the face mask. For the patient with a class III relationship, a removable partial denture (RPD) offers advantages, including the possibility of preservation of remaining teeth, minimal gingival coverage, and enhanced labial support. The low cost of treatment compared to a fixed partial denture is another reason for considering a RPD. When the clinical examination reveals that anterior teeth are missing, there is a tendency towards the loss the labial support. However, regardless of the treatment of choice, good oral hygiene, maintenance of periodontal status and motivation are necessary. The maintenance of periodontal status of at least 1 tooth by residual root provides a passive stability without any retentive feature, and preserves the residual alveolar ridge and maintains the proprioception of the periodontium12-15. The extraction of a residual root, however, is necessary in some situations. As a result of the loss of many teeth, especially in the posterior area, there may be loss of occlusal stability and a decrease in the vertical dimension of occlusion (VDO). In many situations, even with few remaining teeth the VDO is preserved. More important than amount of remaining teeth is how they are distributed in the arch. Even when only one effective occlusal contact is present, there is, in some cases space available to restore a dental arch. In determining the VDO, the patient may demonstrate the following: (1) excessive wear with loss of VDO, (2) excessive wear without loss of VDO but with space available, or (3) excessive wear without loss of VDO but with limited space16. For all of these situations, treatment may be preceded by the use of a removable occlusal splint17. The use of occlusal splint avoids unnecessary tooth preparation, allowing a more accurate evaluation of comfort, stability, esthetics, and phonetics. Castillo et al.18 described successful use of a maxillary and mandibular overlay removable partial dentures (ORPD) to treat a skeletal class III and posterior open bite patient. The ORPD or RPOD is a RPD that gains support partially from tooth roots similar to complete overdenture support. Some advantages of overdentures are alveolar bone maintenance, maintenance of proprioception, increased masticatory ability, increased patient acceptance, additional support and retention, psychological aspects, and can be used as a transitional prosthesis. This clinical report describes an alternative treatment for a patient with anterior reverse articulation occlusal relationship, initially treated with a provisional RPOD and definitively with an RPOD in the maxillary arch. Clinical Case A 47-year-old woman was examined for prosthetic treatment at the Bauru School of Dentistry (University of Sao Paulo, Brazil). Her medical and dental histories were recorded and after an intraoral examination, irreversible hydrocolloid impressions (Jeltrate; Dentsply Ltd, Petrópolis, Brazil) were made for diagnostic casts. Periapical radiographs were also made. Intraoral examination revealed the absence of the left maxillary canine and right and left lateral incisors and premolars. The patient had a past history of generalized carious lesions. The mandibular right canine and first molar were also missing (Figure 1). Occlusal amalgam restorations in all molars were present, except the right first maxillary molar, which was restored with a resin composite. Veneer crowns in the maxillary central incisors and left lateral mandibular incisor were noted (Figure 2). The patient’s chief complaint was the wearing of a removable acrylic resin partial denture. Plaque and gingival inflammation were found on clinical examination. However, periodontal pockets were absent. A face bow transfer was made to mount the diagnostic maxillary cast in a semi-adjustable articulator (BIOART Dental Products, Sao Carlos, Brazil). An anterior deprogramming device was fabricated with acrylic resin (Duralay reliance Dental Mfg Co, Worth, Ill) and a centric relation record was made with a silicone material (Optosil; Heraeus Kulzer, Hanau, Germany) to mount the mandibular cast. The VDO was increased (approximately 5mm) to provide enough space for the restoration of the missing teeth. Afterwards the initial contact was found to be on the buccal edge of the maxillary central incisors without posterior contact (Figure 3). She had a deflective contact in a centric relation that resulted in positioning the mandible anteriorly. Thus, the patient had a skeletal and functional class III malocclusion. After the initial examination, alternative of treatment plans were considered, including orthognatic and orthodontic procedures. Orthognatic surgery would probably be the best treatment for the patient. However, this alternative is invasive and expensive. All the alternatives were presented, and the patient agreed that the RPOD was the most simple and lowcost choice. A provisional and a definitive maxillary RPOD were then suggested. This prosthesis used was based on Castillo et al.18 technique. A diagnostic waxing was made to determine the appropriate position of anterior teeth (Figure 4). The metal-ceramic crowns of maxillary central incisors were removed and then the root of these teeth were prepared as overdenture passive abutments to contribute to support and stability of the denture (Figure 5). Only few adjustments were necessary to insert the RPOD into the mouth. The patient wear the RPOD for 3 months and during this period, she reported acceptable comfort, esthetics and functionality (Figure 6). After the preparation of rest seats and guide planes, an impression with a condensation silicone (Optosil/Xantopren; Heraeus Kulzer, Hanau, Germany) was taken. Rest seats were prepared on mesial surfaces of the first and second maxillary superior of both sides. From the definitive impression, a master cast was made and a framework pattern for restoring plane of occlusion was designed. The master cast was duplicated in investment to be mounted in an articulator. Circumferential clasps were planned for all maxillary molars. Maxillary RPD was cast in chrome-cobalt alloy (Degussa, Legierung, Zur Anfertigung, Germany). The design of major connector was an anterior-posterior palatal bar. The major connector must be rigid in order to perform its functions with maximum efficiency. Clasps and rests were in passive contact with the tooth when framework was completely seated. The definitive RPOD was try-in intraorally. The denture teeth used was an anatomic tooth to simulate the natural tooth form (TRILUX,tooth form E4/ tooth shade 2B; Ruthibras, Pirassununga, Brazil) and then the denture was polymerized in an oven (Lucitone 550; Dentsply, Petrópolis, Brazil) (Figure 7). Based on financial problems, it was determined that the mandibular arch would be replaced with provisional restorations, reinforced with fibers (SPLINT-IT!; Jeneric Pentron, St Paul, Minn.). Reinforced provisional restorations are a practicable restoration technique19-23, prior to long-term treatment, if necessary. The definitive restoration and suitable adhesion were achieved by using photopolymerized resin (Z-250; 3M ESPE; St Paul, Minn). This RPOD has been in service about 6 months, with monthly follow-ups (Figure 8). Patient reported satisfaction after this provisional restoration was installed. There has also been a significant improvement in the patient’s appearance, psychological attitudes, and personal satisfaction. Discussion In the present clinical report the patient was highly cooperative and demonstrated good oral hygiene. Maintaining the two roots and the left maxillary canine will prevent the loss of residual alveolar ridge later in life. In case the patient had no control of a proper hygiene in this area, the tooth would have been removed and the RPOD relined. Thus, RPOD is a reversible and cost-effective procedure. RPOD is a type of overdenture. Overdenture not only transmit more detailed information through the sensory nuclei to the motor centers and muscles12,15, but also increase power during mastication14-15. Based on these studies, the effect of loading over the remaining roots present in the RPOD or overdenture will be very similar. The use of orthodontic therapy was also a treatment option. Chong, Ive, Arthun6 showed changes following the use of protrusion headgear for correcting class III malocclusion. Gallagner, Miranda, Buschang10 evaluated the treatment response and post-treatment follow-up of children with class III treated with palatal expansion and reverse-pull face mask to the maxilla and found that after treatment, the maxilla relapsed relatively backward in the anterior area and upward in the posterior area and that mandible resumed a normal growth direction. Rapid maxillary expansion is used in young patients and has been shown to produce effects that favor class III correction7-8. The method of treatment on this clinical report can be less expensive than other alternatives but surely the most important feature is that it is less invasive. Orthodontic or orthognatic treatments are very safe, but their high invasibility may be a problem for the patient. In this present situation, the reinforced provisional restorations were indicated especially because of their low cost and for being reversible. The placement of glass fibers in the mandibular arch increases the resistance to fracture of the interim fixed partial dentures in a long-term analysis19-23. However, a serious disadvantage with the acrylic resin provisional, reinforced or not, is the risk of recurrent decay and potential endodontic involvement. Then, a traditional treatment will be performed as soon as the patient gets as the financial support. The results hold important clinical implications. By treating the patient early, with a slight amount of overcorrection, a more normal growth pattern might be allowed to proceed thereafter in the maxilla and mandible. If the patient does relapse to a greater or lesser extent, the overcorrection in the orthodontic procedure might be enough to compensate. The situation described in this paper allows the indication of an RPOD. Although greater retention and stability could have been better achieved with other treatments, this technique provided the patient with adequate stability and function. References
Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06011f6.jpg] [os06011f5.jpg] [os06011f8.jpg] [os06011f3.jpg] [os06011f1.jpg] [os06011f4.jpg] [os06011f2.jpg] [os06011f7.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}