 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
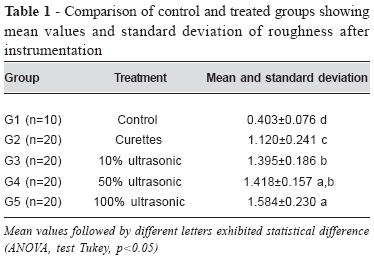
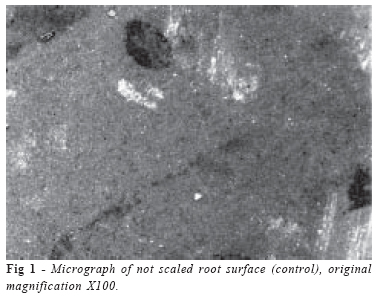
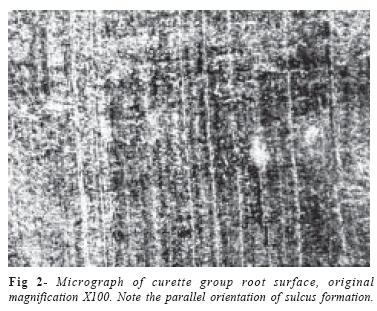
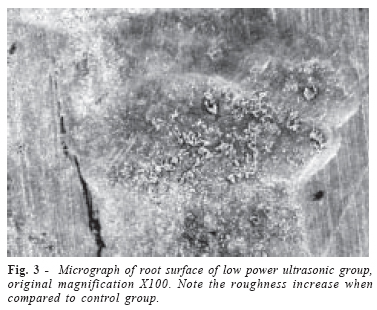
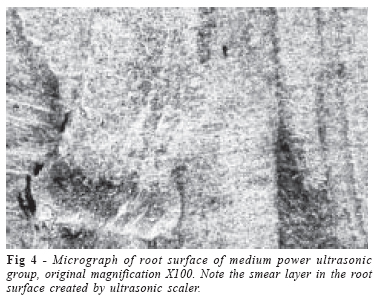
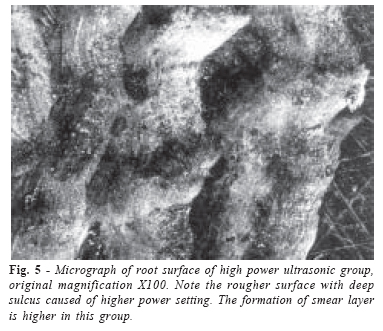
Brazilian Journal of Oral Sciences, Vol. 5, No. 17, Apr-June, 2006, pp. 996-1000 Assessment of ultrasonic root surface scaling with different power settings. roughness evaluation. Renato Corrêa Viana Casarin ,Fernando Rodrigues Pinto, Francisco Humberto Nociti Júnior, Enilson Antônio Sallum, Antônio Wilson Sallum, Márcio Zaffalon Casati Department. of Prosthodontics and Periodontics, Division of Periodontics, School of Dentistry at Piracicaba, UNICAMP Received for publication: March 14, 2006 Accepted: June 01, 2006 Code Number: os06013 Abstract Ultrasonic and curette instrumentation produces a rougher root surface which could be influenced by working parameters such as instrumentation time, pressure and tip angulations. Thus, the aim of this in vitro study was to evaluate root roughness after ultrasonic instrumentation with different power settings and compared it to curette instrumentation. Ninety extracted human teeth were assigned to one of five groups: control group (without instrumentation), curette instrumentation, ultrasonic instrumentation with low, medium, and high power. Before and after instrumentation, surface roughness was measured with a profilometer and the surfaces were examined under the SEM. The mean roughness values of the treated roots were higher than the non-treated roots (0.40+0.08mm). Roots treated by ultrasonic instrumentation had higher roughness means than roots treated by curettes (1.120+0.241mm). Among ultrasonic groups, the higher power setting produced the higher roughness mean (1.58+0.23mm), which was significantly higher than the roughness obtained with the low power setting (1.39+0.18mm). These findings show that ultrasonic instrumentation with a high power setting produced a rougher root surface than ultrasonic instrumentation with a lower power setting. In addition, manual instrumentation with curettes produced lower roughness than ultrasonic instrumentation independent of power setting. Key Words: ultrasonics, root scaling, root planing, potency Introduction The critical determinant of periodontal therapy is not the choice of treatment modality, but the detailed thoroughness of the root surface debridement and the patient’s standard of oral hygiene. In this respect, there is considerable evidence in support of scaling and root planing as an essential and effective component of therapy for inflammatory periodontal diseases1. Since the 1960s investigations concerning manual and powerdriven instrumentation of root surfaces have consistently produced varied and conflicting results2. Ultrasonic scalers appear to attain similar results to hand instruments for removing plaque3, calculus and endotoxin4-5. Due to the fine width of the instrument, furcations may be more accessible using ultrasonic scalers than manual scalers6-7. Based on this characteristic, sonics and ultrasonics may be the instruments of choice for scaling and root planing furcations2. In addition, several studies have shown that the debridement time spent per tooth may be reduced with ultrasonics as compared to manual scaling8-9. However, an ideal goal of periodontal instrumentation is to effectively remove plaque and calculus without causing root surface damage. Studies evaluating differences with regard to the magnitude of root surface alterations produced by hand, sonic, and ultrasonic instruments are inconclusive10-12. When sonic is compared to ultrasonic, some studies find sonic to be equivalent13 or inferior to ultrasonic with regard to root surface smoothness14-15. Several older studies report that curettes leave the root surface smoother than ultrasonics16-17. Studies also reveal that as instrument contact time, tip to tooth angle, and instrument pressure is increased, the likelihood of root surface damage is also increased. Lie and Leknes11 (1985) compared efficiency and possible iatrogenic effects of cleaning of three different air turbine scalers with an ultrasonic instrument at different power settings. A Subjective index (which was a combination of the Scanning Roughnes Index17 and Loss of Tooth Substance Index13) were used to measure the roughness after instrumentation and substance removal. Ultrasonic instrumentation at a medium power setting caused few lesions, but the surface roughness was noticeable, on the other hand, at the maximum power setting both roughness of the surface and removal of considerable amounts of tooth substance was observed. Therefore, the aim of this study was to evaluate the root roughness with the use of profilometer and SEM examination with ultrasonic instruments at different power settings and to compare these results with curette instrumentation in an in vitro study. Material and Methods This study was previously submitted and approved by the Ethics Committee of the Piracicaba Dental School under protocol number 02/2006. Collection of Experimental Sample: Ninety mandibular and maxillary premolars extracted for orthodontic reasons were selected for this study. All teeth were donated to the study and were rinsed in 10% formalin for 1 month. Selection Criteria: All teeth had to meet the following criteria: intact root surface, absence of caries, a negative history of periodontal involvement, absence of gross soft and hard debris. The final selection was made with a 4X stereomicroscope magnification and teeth with root concavities or convexities which impeded the planning of the root surface were excluded. Mounting Procedure: The crowns of the teeth were removed and each root was mounted in a 2cm high plastic tube filled with acrylic resin (Jet Classico, São Paulo – SP, Brazil) with the most plane surface between the buccal or lingual surface of them exposed. Before the instrumentation, roots were polished in crescent granulations of rotating sandpaper (300, 400, 600 and 1200) and felt disc, to reach a similar visual roughness for all samples. The mounted teeth were numbered from 1 to 90 and randomly assigned by a toss to one of the five groups of the study. To avoid reading localization errors a 3x3mm area at the polished face of each root was delimitated as the reading area. Pre-instrumentation roughness reading: Surface roughness was measured with a profilometer (Surf-Corder SE 1200 Kosaka Laboratory Ltd.) at 0.1mm/sec reading speed following the ANSI standard. Each root received 6 roughness readings (3 parallel and 3 perpendicular to the scaling) to determine a mean roughness for each tooth. Root Scaling: Five modalities of treatment listed below were performed by the same operator: Group 1 – control, without instrumentation; Group 2 – scaling with Gracey curettes 5-6 (Gracey; Hu-Friedy, Chicago, Ill); Group 3 – scaling with ultra-sonic scaler at low power (Dabi Profi III – Bios, Ribeirão Preto, SP, Brazil); Group 4 – scaling with ultra-sonic scaler at medium power; Group 5 – scaling with ultra-sonic scaling at high power. The group treated with curettes received 15 apical to coronal strokes with a new curette per tooth; ultrasonic groups received 15 apical to coronal strokes with zero degree inclination between tip and root18. Post-instrumentation roughness evaluations: A roughness reading was performed again on all treated roots to determine a mean roughness for each treated root surface. Four samples of each group were selected for scanning electron microscopy (SEM) using a JEOL JSM-T330A (Japan) with a magnification of 100X. The images acquired were used for descriptive analysis. Statistical Analyses: Differences in roughness means after instrumentation were evaluated by analysis of variance and by the Tukey test (α=0.05). Results Roughness: All treated groups showed a significant increase in roughness (p<0.05) compared to the control group (0.403 ±0.076mm). However, in comparing the direction of the roughness readings (parallel or perpendicular) there were no differences in all samples. The use of ultrasonic instrumentation at all different powers represented a significant increase in roughness (p<0.05) compared to the curette group. The ultrasonic scaling at maximum power showed the highest roughness (1.584±0.23mm); however, this difference was not significant when compared to group 4 (Table 1). Microscopy Descriptive Analysis: Differences in surface topography of the treated groups could be seen clearly. The treated surfaces showed an irregular aspect different from the negative control root surface (FIG 1). The curette group harbored a better finishing surface (FIG 2) presenting sulcus in the same direction as the scaling movements and showing less roughness when compared to ultrasonic groups. The ultrasonic groups showed the presence of deeper sulcus and rougher surfaces than the curette group (FIG 3,4 and 5). Among the ultrasonic groups, group 5 exhibited the highest surface roughness, as well as the deepest defects caused by scaling. The presence of a smear layer was common for the treated groups but the ultrasonic groups harbored a greater amount. Discussion In the present study, a positive correlation was observed for superficial roughness of root surfaces and the power setting of an ultrasonic device. Additionally, as previously demonstrated by other6,9,11,13, the present investigation showed that rougher root surfaces are produced by ultrasonic instrumentation than by curettes. Scanning electron microscopy showed that curettes created grooves, valleys and peaks that run in the direction of the tooth’s long axis. The use of ultrasonic instrumentation created surface alterations including scratches, gouges and nicks. The images of the scanning electron microscopy showed the presence of a smear layer in both kinds of instrumentation, but the ultrasonic group exhibited a greater amount of smear layer mostly when maximum power was used. The differences in methodologies used to determine the effects of these instruments over the root surface has made difficult and Kocher et al.19 demonstrated that the measurement of roughness is dependent on the area to be evaluated. The use of curettes results in a surface with a regular pattern of roughness and in a two dimensional measurement with the formation of sulcus in the same direction of scaling, like it was observed in this study. Due to this pattern of sulcus formation quite different results could be found dependent of the direction of reading (across or along). Since ultrasonic instruments produces an irregular pattern of roughness, the reading of roughness should be performed in both direction even for curette groups as for ultrasonic instruments to achieve a reliable evaluation of the two modalities, like it was performed in the present study. Schlageter et al.20 found statistical differences in roughness between instrumentation with curettes (1.9 ±0.84mm) and ultrasonic scalers (2.48 ±0.9mm). In the present study, a direct relation could be observed between the increase of ultrasonic power and the roughness produced which is in accordance with Flemming et al.18,21, who found in the respectively studies a relation between power, for ultrasonic instruments, and angulation of the tip to substance removal and depth of the defects formed with both sonic21 an ultrasonic18 scalers. Chapple et al.22 evaluated the effect of instrument power setting during instrument scaling upon treatment outcome in a split mouth study in 17 patients with chronic periodontitis, they compared periodontal healing during six month when ultrasonic scaler was operated at full and half power and the results showed that the use of half power setting was as effective as using the ultrasonic scaler at full power. Although differences in ultrasonic power devices seem not to influence clinical results of periodontal treatment22, the increase in roughness could directly influence the accumulation of dental biofilm over exposed root surfaces11. Since no differences are observed in clinical results, harboring similar benefits in pocket reduction and bleeding on probing, ultrasonic scalers have the advantage of reduction in time spent and operator stress. An interesting point to be considered is that after scaling and root planning a gingival retraction is expected due to the reduction in tissue inflammation and those areas previously considered subgingival, where an increased roughness should have no importance in clinical outcome, can turn to supragingival root surface, what could influence biofilm retention. Ideally, scaling and root planning should only remove staining, plaque, calculus and bacterial components adhered to root surface causing no or minimal damage and roughness. However the present study demonstrated that both curette and ultrasonic instruments cause root increased roughness which could facilitate biofilm accumulation and, thereby, compromise daily plaque control. Considering these aspects, it could desirable a supragingival root polishing to achieve a smother surface. By analyzing the images of the scanning electron microscopy, they demonstrated the differences among curette group and different power of ultrasonic scaling groups. While the surfaces of curettes group harbored a better surface finishing, the use of ultrasonic produced a rougher surface and deeper sulcus formation. The presence of smear layer was found on SEM examination (FIG. 2 and 5) in both kind of instrumentation, but the ultrasonic group seemed to exhibit a great amount of smear layer mostly when maximum power was used. Scanning electron microscopy not only allows investigating the instrumented root surface but also enables comparisons with profilometer measurements11, but these results are difficult to compare since standardization of operating conditions such as orientation of instrumentation, pressure applied and operating settings of the instruments may differ. An effectiveness scaling and root planning is a hard procedure to be achieved with manual or ultrasonic scalers, but it seems that ultrasonic instruments may increase operators efficiency compared to curettes9, besides that, time spent and operators demands to achieve a good scaling is lower using ultrasonic instruments. Subgingival roughness influence over the success of periodontal treatment is no conclusive, since some studies demonstrated that these changes over radicular topography do not interfere on the response to periodontal treatment12,22, others suggest a relation of the radicular roughness over plaque accumulation and inflammatory cells migration11. The significance of wound healing is still unclear since most human studies have not found clinically significant differences in wound healing following hand, sonic or ultrasonic instruments23. Considering the rougher surface produced by ultrasonic instruments, it could facilitate supragingival plaque accumulation, so a root polishing should be considered in these areas. In conclusion, ultrasonic instrumentation at high power settings produces rougher root surfaces than ultrasonic instrumentation at lower power. An addition, manual instrumentation with curettes produces lower roughness than ultrasonic instrumentation independently of power setting. Acknowledgments The authors would like to thank to FAPESP for the financial support to this study (02/0666-1), to Glaucia Bovi Ambrosano - Department of Social Dentistry, UNICAMP for the statistical analysis support and to Marcelo Giannini - Department of Restorative Dentistry, UNICAMP - who ceded the surface roughness measuring instrument for the execution of this study (Process 51234 –FAPESP). References
Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06013f5.jpg] [os06013t1.jpg] [os06013f2.jpg] [os06013f3.jpg] [os06013f1.jpg] [os06013f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}