 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
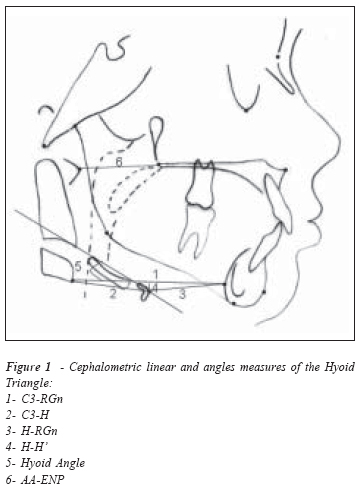
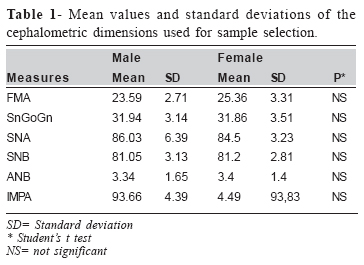
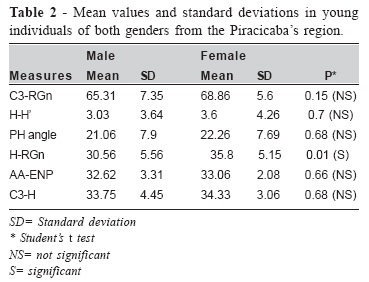
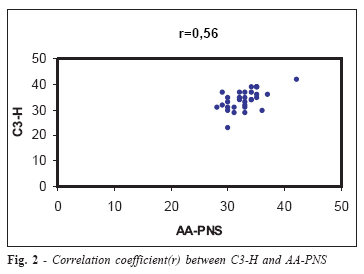
Brazilian Journal of Oral Sciences, Vol. 5, No. 17, Apr-June, 2006, pp. 1001-1006 Cephalometric appraisal of the hyoid triangle in brazilian people of Piracicaba’s region Maria Julia Pereira Coelho Ferraz1 Darcy Flávio Nouer2 Fausto Bérzin3 Meire Alves de Sousa4 Fábio Romano4 1Master in Orthodontics, Piracicaba Dental School, / UNICAMP, Brazil PhD student, Piracicaba Dental School, / UNICAMP, Brazil Member of CEBAPE Received for publication: October 14, 2005 Accepted: May 16, 2006 Code Number: os06014 Abstract The Triangle Hyoid was measured by cephalometric measures in Brazilian individuals from Piracicaba’s region by establishing comparisons with the values existing in the literature objectiving to establish values of normality for the position of the hyoid bone. The sample consisted of 31 cephalometric radiographs of Brazilian individuals with Angle’s Class I malocclusion, mix dentition,16 boys and 15 girls with ages raging from 8 to 15 years. The gotten data had submitted it test “t” of Student that showed the occurrence of sexual dimorfism for the ântero-posterior position of the hyoid bone(H) to the retrognation (RGn). The antero-posterior hyoid position (H) in relation to the third cervical vertebra (C3) was constant, with values of 34.03 mm and standard deviation of 3.85. The distances between antero-posterior position of C3 and symphysis (RGn) were similar to those found in the literature. The vertical position of the hyoid bone was higher and less inclined. The correlation coefficient between the atlas vertebrae to posterior nasal espine (AA-PNS) and C3-H was significant (0.56), which is suggesting that the hyoid bone represents the previous limit of the upper airspace in a level more inferior than the PNS in accordance with the literature. It concluded itself that there is a related sexual differences and face standard with the position of the hyoid bone indicates the necessity of a refined evaluation of this bone, therefore represents an important element for the orthodontic and functional orthopedic and speech therapist and physitherapist. Key Words: hyoid triangle, orthodontic diagnosis, class I malocclusion. Introduction Because of the complexity involving the stomatognatic system, a specific knowledge of anatomy, physiology and craniofacial growth theories are both necessary and indispensable for understanding such a complexity individually. As the possibility of relapse exists as the result of oral habits such as atypical deglutition and mouth breathing, the relationship between respiratory pattern and craniofacial growth has been producing controversy among the practitioners from Dentistry, Medicine, Phonoaudiology and Physiotherapy1-2. According to Meredith3, a great increase in growth occurs in the first days of life. At birth, the craniofacial skeletal of a Caucasian correspond to 60% of the cephalic size in adults, 80% at six months of life, 90% at three years, and 95% at nine years. Therefore, most of the facial growth has already occurred at 12 years old, when many orthodontists begin the treatment. As a result, it is important to follow a preventive approach before the final phase of the craniofacial growth. As the lingual functions and mandibular muscles are thought to affect the craniofacial growth and development, the morphological analysis of the hyoid bone would be considered for evaluating how shape is affected by function, since the hyoid bone is supported by muscles only, with no osseous connection with skull and mandible. Therefore, the hyoid bone position depends on the balance involving the surrounding soft tissues4. As the stomatognatic system plays an important role in positioning the hyoid bone both anatomically and functionally, we propose the establishment of cephalometric measurements of the hyoid triangle according to Bibby and Preston5 in Brazilian people living in Piracicaba’s region that the results compared with those found in the literature, too. Brodie6 and Durzo and Brodie7 have studied the morphology and the function regarding the hyoid bone, and other authors2,4-5,8-16 have investigated the hyoid bone position in relation to the skull and the vertebral column by using cephalometric techniques. Sicher and Dubrul17 have reported that the hyoid bone represents the “tongue’s skeletal”, i. e., a U-shaped bone consisting of one body, two larger horns and other two smaller horns. The hyoid bone is located between the tongue (above) and the larynx (below), and it has a characteristic aspect of being externally subcutaneous and internally submucous. The hyoid bone is partially suspended by ligaments which extend from the tips of the styloid processes to the hyoid smaller horns. The muscles fix the hyoid bone to tongue, mandible and skull above and to thyroid cartilage, sternum bone and scapula below. The muscular movement of mastication, deglutition and phonation is based upon the great mobility of the hyoid bone. Stepovich11 pointed out that orthodontists often finish the treatment with relatively successful outcomes, but relapse may occur due to atypical lingual pressure. As the studies of deglutition was suggesting that hyoid bone might have a different position in those patients with such an atypical lingual pressure, the author developed a technique to measure the hyoid bone vertically, horizontally and angularly. He also described the hyoid plane. In order to establish the hyoid angle, it was traced a line over the long axis of the hyoid bone and another line perpendicular to the S point (sella) over the SN line (Sella-Nasio). The vertical position was determined by measuring the distance between S point and the intersection formed by the two lines cited above. The horizontal position was determined by measuring the intersection formed by these two lines with point H (Hyoid). The study consisted of lateral teleradiographs of 28 male individuals aged between 13 and 35 years, and they were divided into four groups. Groups A and B consisted of eight radiographs of each individual taken in different days. Group C consisted of four consecutive radiographs of each individual. Group D consisted of three radiographs taken in three days consecutively, and the subjects had a metallic ring placed around their tongue’s tip in order to stabilise it. All the individuals had Angle’s Class I malocclusion and normal deglutition, but no open-bite. The results showed no significant correlation between the FMA angle and the occlusal plane in relation to the hyoid plane, with the hyoid plane crossing the third cervical vertebra. The same study has also demonstrated that the hyoid bone had different positions in each radiograph taken from the same individual, although precautions to avoid the movement of the hyoid bone had to be taken. Kuroda et al.4 studied the relationship between hyoid bone, skull and mandible by using lateral teleradiographs in order to elucidate the functions of both tongue and supra-hyoid muscles. The sample consisted of 20 Japanese adults presenting normal occlusion, 20 having Class II division 1 malocclusion, and 20 having Class III malocclusion. Regarding the angular measure SNA, the results showed no statistically significant difference between the groups. Regarding the other angular measure SNB, the mandible was found to be slightly backwards in Class II individuals and forwards in Class III ones. The relationship between the hyoid bone and the anterior cranial base (NS) showed significant difference in the hyoid bone position in all groups studied. The body of the hyoid bone was located slightly backwards in Class II individuals and slightly forwards in Class III individuals in comparison with the control group. However, the relationship with the mandible, which was determined by the mandible measure (genian tubercle or point G) and the cranial base measure (Bolton´s point), showed that the hyoid bone position was constant in the three groups. In order to confirm the relative stability of the hyoid bone in relation to the mandible, two cases had been presented with severe craniofacial alterations: ankylose of the temporomandibular articulation as well as inferior protrusion with severe distortion of the cervical vertebra. The position of the hyoid bone in relation to the mandible was virtually stable in both cases. Regarding the cranial base, such a relation showed changes depending on the antero-posterior position of the mandible in relation to the skull. Bibby and Preston5 advocated that the position of the hyoid bone might be easily determined in three directions by using the relationship between cervical vertebra and mandible instead of using the planes of cranial reference. As the level of the mandibular symphysis is more comparable to the head rotation axis than the skull, the effect of the head movement might be minimised and as a result the position of the hyoid bone could be more correctly determined. Consequently, they developed an analysis of the hyoid bone position known as Hyoid Triangle, which is formed by the following points: Retrognation – RGn (the most posterior-inferior point of the mandibular symphysis), Hyoid point – H (the most anteriorsuperior point of the body of the hyoid bone), and C3 (the most anterior-inferior point of the third cervical vertebra). The antero-posterior position of the hyoid bone was determined by H-RGn and H-C3 both anteriorly and posteriorly. The vertical position of the hyoid bone was determined by the plane C3-RGn in relation to the Hyoid point (H-H’) perpendicularly. The angular position of the hyoid bone incorporating the larger horn was determined by the angle formed by the hyoid axis and C3-RGn plane. The sample consisted of 54 individuals of both genders with Class I malocclusion without any significant vertical discrepancy. The mean ages for male and female individuals was 12.5 and 13 years, respectively. The anterior-posterior position of the hyoid bone in relation to the cervical vertebra remained constant with a mean value of 31.76 mm + 2.9, and a positive linear correlation between angular and vertical measures (Hyoid plane angle, H-H’, respectively) was found. The anterior-posterior dimension regarding the measure AA-ENP was also constant with a mean value of 32.91 mm + 3.66. A positive and significant correlation coefficient was established between AA-ENP (the most anterior point of the Atlas vertebra in relation to the posterior nasal spine) and C3-H, thus suggesting that the hyoid bone would represent the lower osseous limit of the pharynx more inferiorly than the ENP. There was found no sexual dimorphism regarding the hyoid position for the sample studied. Adamidis and Spyropoulos14 reported a statistically significant difference in both position and inclination of the hyoid bone between the Class I and Class III malocclusions. Individuals with Class III malocclusions, particularly the boys, showed a more anterior position of the hyoid bone as well as a decreased inclination, which was almost reverted in relation to the hyoid angulation with the mandibular plane, involving either centric occlusion or wide open bite. This might influence the function of the supra-hyoid and infrahyoid muscles and consequently the mandibular growth. Tallgren and Solow13 have suggested that the position of the hyoid bone might be influenced by two postural systems: change in the mandibular position and changes in the cervical inclination as well as in the craniocervical angulation. Vertical changes in the position of the hyoid bone in relation to the upper face followed the pattern of increase or decrease of the mandibular inclination, whereas the horizontal changes followed mainly the changes in both cervical inclination and craniocervical angulation. Such findings were obtained by lateral teleradiographs of 24 female adults who were using both superior and inferior prosthesis during a period of 15 years. They emphasised that such changes in the hyoid position should not involve the mandibular inclination only, but also head and cervical posture. Haralabakis et al.15 have used cephalometry to investigate the position of hyoid bone in adult individuals with open bite. The open-bite group was compared with a Class I group (control) in order to aid both diagnosis and aetiology of the malocclusions before beginning the orthodontic treatment. The sample consisted of 39 individuals of both genders, 16 males and 23 females aged between 15 years and two months to 26 years and three months, all presenting long face syndrome and open bite not less than 2 mm. The control group consisted of 43 individuals of both genders, 25 males and 18 females aged between 20 years and four months to 27 years and three months, all presenting Class I occlusion. The results showed that the majority of the horizontal measures had no statistical difference regarding the position of the hyoid bone in both groups. On the other hand, the vertical measures had only a significantly increased distance between hyoid bone and palatine plane in male individuals with open bite caused by the development of such a dentalskeletal malocclusion. The angles formed by the hyoid axis with either the nasio-nasio plane or the palatine plane were significantly high in the open-bite group, however no statistical difference was found regarding the mandibular plane. Consequently, the authors have hypothesised that the movement of the hyoid bone occurs in association with pharynx, cervical vertebra and mandibular plane in those patients with different skeletal patterns. Kollias and Krogstad16 have longitudinally investigated the craniofacial morphology and the hyoid position by using lateral teleradiographs of 26 men and 24 women who were divided into three different age groups with 10-year interval. The authors concluded that the craniofacial growth continues even after the third decade of life. The most significant changes occurring either in males or females after a period of 20 years showed decrease in the mandibular prognathism as well as an increase in the mandibular plane angle in females. The hyoid bone showed a more inferior position in relation to the craniofacial structures, and its horizontal position was stable. The inferior movement of the hyoid bone was significantly greater in men than in women, and the postural change of the head was similar in both genders. Coelho-Ferraz2 has evaluated the position of the hyoid bone in relation to the predominant respiratory pattern. The sample consisted of 53 young females with mean age of 10 years old, where 28 had predominantly mouth breathing and 25 had nasal breathing. All the subjects had Angle’s Class I malocclusion with no significant vertical discrepancies. The results showed that the hyoid position was stable in both groups. Material and Methods The present study was carried out only after being approved by the Faculty of Dentistry of Piracicaba’s Human Research Ethic Committee according to documentation required by the Ministry of Health’s Commission on Ethics (process: 059/2003). One hundred eighty clinical records from the Faculty of Dentistry of Piracicaba, State University of Campinas (UNICAMP), were initially evaluated, and 31 lateral teleradiographs of Brazilian individuals from the Piracicaba’s region were selected for study. The samples consisted of 16 male individuals with mean age of 11.8 years (standard deviation of 1.84) and 15 female individuals with mean age of 11.52 years (standard deviation of 2.13). All the subjects presented, mix dentition, Angle’s Class I malocclusion with no significant vertical discrepancies according to the following standard cephalometric measures: SNA, SNB, ANB, GOGn, and FMA. The radiographs followed the norms established by the Faculty of Dentistry of Piracicaba and were in accordance with the technique developed by Broadbent & Hofrat in 1931. The teleradiographs were obtained by using a Siemens X-ray device “SK-150”, with the subjects upright and the Frankfurt plane parallel to the floor. The selected cephalograms were traced by a single researcher using a negatoscope inside a dark room. The cephalometric tracings were performed by using “ultraphan” paper with the standard size of 17.5 x 17.5 cm and 0.07 mm of thickness, 0.3 mm pencil case, transparent ruler with 0.5 mm subdivisions, protractor with an approach of 0.1 degree, template, adhesive tape and negatoscope. Skull, face, cervical vertebra and hyoid bone were the anatomical structures delineated by the lines and planes traced according to Bibby and Preston5 .The cephalometric tracings were repeated 7 days after and supervised by a mentor. The error limit was established in 0.5 mm and 0.5°. The Hyoid Triangle is formed by the union of the following points: Retrognation point (the most posterior-inferior point of the mandibular symphysis), hyoid point (the most anteriorsuperior point of the body of the hyoid bone), and C3 (the most anterior-inferior point of the third cervical vertebral body). The anterior-posterior position of the hyoid bone was determined by the linear measures H-RGn and H-C3 both anteriorly and posteriorly. The vertical position of the hyoid bone was determined by the plane C3-RGn in relation to hyoid point (H-H’) perpendicularly. The angular position of the hyoid bone incorporating the larger horn was determined by the angle formed by the hyoid axis and C3-RGn plane. The osseous limit of the pharynx is indicated by the points AA, which is the most anterior point of the Atlas vertebra, and ENP, which is the posterior nasal spine (Figure 1). In order to evaluate the reliability of the cephalometric measures, the tracings were performed twice by a single researcher at 1-week interval under the same conditions of investigation. The average of the values found in the two tracings was used for assessment. Thirty days after the tracings ten lateral radiographs were randomly chosen for examining the error made between the two periods of tracing by using the error calculation proposed by Dalberg18 and advocated by Houston19. Descriptive analysis (average and standard deviation) was initially performed for analysing the data obtained. It was also used both test F and Student’s t test with significance level of 5%. According to Stepovich11, the correlation between the variables was analysed by using the Pearson’s correlation coefficient20 with a = 0.05. Results The tracings and measurements were found to be reliable since no statistically significant difference was observed between the two periods evaluated. The cephalometric measures demonstrating the skeletal characteristics of the subjects and the lack of sexual dimorphism are shown in Table 1, that showing the mandibular morphology feature, without big bone and dental discrepancies. The cephalometric measures for the Hyoid Triangle in the Brazilian individuals from the Piracicaba’s region are shown in Table 2. The sexual dimorphism observed in the sample was tested and no statistically significant difference was found, except one regarding the measure H-RGn(p< 0,05). It studied, too, the correlation between the variables that measure the hyoid position using the Pearson Correlation, The significant correlation between the variables measuring the distance between AA-ENP and C3-H (r = 0.56) was also studied ( Figure 2) DiscussionThe sample consisted of both male and female individuals presenting significant differences for the measure H-RGn, thus demonstrating the importance of considering the sexual dimorphism in the skeletal morphology. The basic difference regarding this measure occurs following the puberty, when the boys grow faster and for a longer period than the girls21, particularly with respect to the growth of the cervical vertebra8,11 . The skeletal characteristics presented a homogenous behaviour in this study, i. e., with no significant vertical discrepancy. In terms of quality, however, it was observed a biprotrusion trend involving predominantly the basal maxillary component in male individuals. The high frequency by which the craniofacial changes justifies the functional orthodontic and/or orthopaedic treatment of the maxilla was considered for the age group of 11 years. According to Meredith1, 95% of the craniofacial growth is complete at 9 years old. For this reason, it is important to consider the preventive aspect during the diagnostic process3. Because one of the etiologic agent of the malocclusion is the inadequate buccal habits, i.e. atypic deglutition, buccal breathing, and others, the hyoid positon will be to the important instrumet of diagnosis22. The anterior-posterior position of the hyoid bone in relation to the cervical vertebra (C3-H) was relatively constant, with a mean value of 34.75 mm + 4,45 for male and 34,33mm+3,06 for female , which might suggest the role of “security belt” provided by such an osseous structure23. These findings are in accordance with those found by Bibby & Preston5, Bibby22 and Kolias and Krogstad16, thus indicating that the horizontal distance of the hyoid bone is not influenced by the age. Additionally, this stability may depend on the anatomical and functional association between the hyoid bone and the laryngeal cartilage13. According to Bibby and Preston5 and Haralabakis et al.15, the stability of the hyoid position depends on the functional reflexive activity. The mean values regarding the Hyoid plane angle and H-H’ had high standard deviations, which is in accordance with Billy and Preston5, who recognised that both vertical and angular measures have greater variations than the linear ones. The measure regarding the anterior-posterior distance between the upper pharynx (AA-ENP) was relatively constant, with a mean value of 32.62 mm + 3,31 for male and 33,06 + 2,08 for female, thus corroborating the findings by Bibby and Preston5 and Coelho-Ferraz2. Additionally, such a measure is thought to be determined during the first stages of life8. The anterior-posterior distance between AA-ENP and C3-H had a significant correlation coefficient of 0.56 in compariosn to 0.98 and 0.40 found by Bibby and Preston5 and Coelho-Ferraz2, respectively. The vertical behaviour presented by the hyoid bone was shown to be irregular, which is in accordance with Bibby and Preston5, Bibby22 and Coelho-Ferraz2. Such an irregularity also corroborates the findings by Bench10, that is, the position of the hyoid bone revealed to be unstable during the stages of mix dentition, thus suggesting a loss of lingual support as well as a possible increase in the lip tension during the late stages of growth. It considering the features of the used sample, the used methodology and the carefeul analysis of the presented dates, it was possible to conclude: 1- Correlation There was the correlation between cephalometric measures and upper pharynx and lower pharynx, which is in accordance with Bibby & Preston5 and Coelho-Ferraz2. 2- The standard values regarding the Triangle Hyoid may be used for Brazilian young living in the Piracicaba’s region. References
Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06014f2.jpg] [os06014f1.jpg] [os06014t2.jpg] [os06014t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}