 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 5, No. 17, Apr-June, 2006, pp. 1007-1011 Correlation between Candida spp.and DMFT index in a rural population Sheila Cavalca Cortelli1 Juliana Campos Junqueira2 Ivan da Silva Faria3 Cristiane Yumi Koga Ito4 José Roberto Cortelli5 1Assistant Professor of Periodontics, Department of
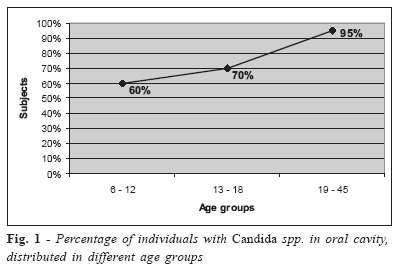
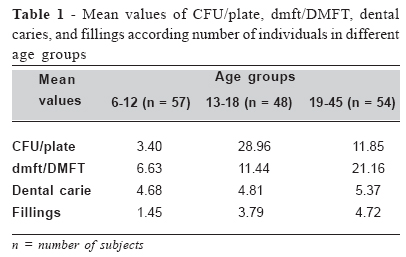
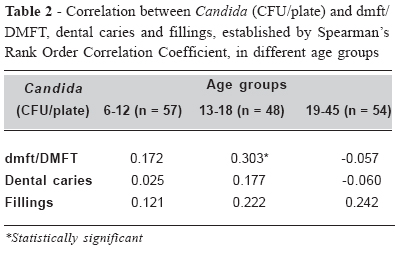
Dentistry, University of Taubaté, SP, Brazil Received for publication: August 19, 2005 Accepted: May 19, 2006 Code Number: os06015 Abstract Oral presence of Candida spp. was correlated with caries experience (dmft/DMFT index) in a rural population. dmft/DMFT index were evaluated in individuals between 6-12 years of age (n=57), 13-18 years of age (n=48) and 19-45 years of age (n=54). For the isolation of Candida spp., saliva samples were collected and spread on Sabouraud dextrose agar plates. The number of colony- forming units per plate (CFU/plate) was calculated and the isolates were identified. Data were analyzed by Chi-square and Spearman’s correlation coefficient (p<0.05). The mean value obtained for dmft/DMFT index were 6.63 (6-12 years of age), 11.44 (13-18 years of age), and 21.16 (19-45 years of age). Candida spp. were isolated from 60% of the individuals between 6-12 years of age, 70% of the individuals between 13-18 years of age and 95% of the individuals between 19-45 years of age. In the 13-18 years of age group a positive correlation between Candida and DMFT was observed. No correlation was observed among Candida and DMFT index in the others age groups. In conclusion, the presence of Candida spp. in the oral cavity seem to be related with past caries experience in young adults from 13 to 18 years of age. Key Words: caries, Candida, age groups Introduction The identification of high caries risk individuals and groups is a matter of great interest in public health programmes. It is widely accepted that caries prevention and treatment would be more cost-effective and efficient if the subjects or groups of subjects under greatest risk could be identified. With this aim, methods for predicting caries risk are being investigated. Several indicators including clinical, microbiologic, salivary and socioeconomic factors have been analyzed and discussed in relation to dental caries. So far, none of the indicators alone is able to make correct predictions1. Combined information of several predictors showed to have good ability to distinguish subjects in relation to high or low caries increment2-4. Past caries experience, plaque index and microbiological factors are easy to determine and show a reasonably good association with caries risk5-6. However, in case of three or more factors the interrelations may cause difficulty in the analysis of data2. Many microbiological studies have shown an association between high levels of mutans streptococci or lactobacilli and caries prevalence or incidence7-9. According to Moalic et al.10, the role of the saprophytic fungal microbiota as a risk factor for dental caries has, to date, not been clearly established. However, other studies11-14 found associations between Candida and caries prevalence. Indeed, Coulter et al.5 reported that the level of salivary Candida could be more useful as an indicator of microbial risk factors in caries than the lactobacilli count. Positive correlations between salivary parameters, caries experience and caries increment were established specially in children2,12-14 and adolescents1,15. However, the data on adult population are still scarce. The oral yeast tends to increase as a result of an increment in the number of retentive sites such as prostheses, orthodontic appliances and pacifiers16. Moreover, other factors such as the socieconomic conditions seem to interfere in the colonization by Candida12,14. Koga-Ito et al.17 reported an increased isolation of Candida spp. in mouthbreather children in relation to control ones, indicating the environmental influence in the candidal colonization. The aim of this study was correlate Candida spp. with caries experience in different age groups of a rural population. Material and Methods The study population included subjects from a rural village of Itamonte, Minas Gerais, southeastern of Brazil. The total population of this village is comprised of 309 individuals, from 1 month to 83 years old. One hundred fifty-nine individuals who agreeded in participating of the study were included. They were divided in 3 age groups: 6-12 years of age (n=57), 13-18 years of age (n=48) and 19-45 years of age (n=54). In case of children, prior consent was obtained from their parents. The protocol for this study was approved by UNITAU Committee on Human Research Ethics (Protocol number 0033/01). The criteria of exclusion were the presence of fixed or mobile orthodontic appliances or prosthesis, the treatment with systemic antibiotics or other drugs capable of altering the salivary flow or the ecological constitution of the oral microbiota, interfering, therefore, with the research. The socioeconomic status of the study population, as assessed by familial income, was determined by means of a questionnaire completed by the responsible of each family. The factors investigated at the interview were: age, gender, smoking habits, dental hygiene (frequency of brushing, flossing, and the use of toothpaste or mouthwash use), and eating habits. Caries experience was assessed by the number of decayed, missing, filled teeth (dmft/DMFT), based on World Health Organization18. Diagnostic intra-examiner consistency was evaluated by a double scoring of 20 children. Intra-examiner Kappa values for dmft and DMFT were 0.92 and 0.90, respectively. Observations were called out to a second person who recorded the data on a standard chart. Both dental arches were examined in their entirety. Following the examination and microbial sampling, oral hygiene instruction, a toothbrush, toothpaste and dental floss were given to all the individuals. Saliva samples for Candida counts were taken from unstimulated saliva sublingually, from cheek and dorsum of the tongue with sterile cotton swabs. After gently rubbing, the samples were immediately inoculated onto Sabouraud dextrose agar (Difco, Detroit, USA) added with 0.1 mg/mL of chloramphenycol (Carlo Erba, Rio de Janeiro, Brazil). The samples were incubated at 37oC for 2 days and at room temperature for 5 days. The counting of CFU/plate was carried out after the growth of characteristics yeast colonies. The morphological characteristics of Candida colonies and those of colonies with different aspects were confirmed in a stereoscopic microscope. Gram staining was utilized in order to recognize other types of cells. The colonies that presented grampositive budding cells of yeasts were sub-cultured and identified19. The statistical analysis was performed using Minitab, version 13.1, 2000 and the difference was considered to be significant when p < 0.05. The presence or absence of Candida spp. was compared with gender and caries prevalence by Chi-Square test. The correlation between Candida level (CFU/ plate) and caries experience was performed by the Spearman’s Rank Order correlation coefficient. Results Among the 159 subjects studied, 83 were females and 76 males. According to Brazilian per capita income, this population was considered of low socioeconomic status. 100% At the village of Campo Redondo there are no markets. By this way, no sweets candies are available. The sugar is sold directly to the families once a month. Consumption of sugar reaches 216 grams/ person/ day. Twenty-two percent of individuals reported to brush their teeth with an average of three times a week, 67% reported brushing once a day, and only 11% brushing their teeth twice a day. The individuals reported to brush their teeth with fluoride toothpaste. Just three of all individuals examined reported the use of dental floss once a day. None of the individuals examined related the use of mouthwashes. Among the individuals studied only five were smokers. Out of the 159 oral samples collected, 50 (31.44%) did not present any fungal growth and 109 (68.55%) presented fungal microbiota consisting of Candida and Rhodotorula with an average of 20.4 CFU/plate. The Candida genus was isolated from all the 109 sample. Four different species of Candida were identified and C. albicans was always the most frequently isolated species, representing 84.88% of all the fungi isolated. Additionally, 8 (7.33%) C. tropicalis, 2 (1.83%) C. krusei, 1 (0.91%) C. glabrata and 6 (5.5%) other Candida spp. were isolated. Rhodotorula genus was isolated from three samples. Twenty-two (13.8%) subjects were caries free and 137 (86.2%) subjects presented caries with a mean number of 5.13 and a range from 1 to 18 active lesions. Fifty eight (36.47) subjects were fillings free and 101 (63.52%) subjects presented fillings with a mean number of 5.14 and a range from 1 to 23 fillings. The mean dmft/DMFT value was 13.01 and the mean PASS index was 66.44%. According to the different age groups, the percentage of individuals with Candida spp. in oral cavity was presented in Figure 1 and the mean number of CFU/plate, DMFT/dmft, dental caries, and fillings were presented in Table 1. In the 6-12 years group, Candida spp. were isolated from 17 females and 16 males. Nineteen females and 5 males had not presented Candida spp. in their oral cavities. In this age group, gender was associated with Candida spp. (χ2 = 4.56; p = 0.03). In the 13-18 years group, Candida spp. were associated with caries prevalence (χ2=5.44; p=0.02) and significant positive correlation was found between Candida (CFU/plate) and DMFT/dmft (Table 2). However, in the 6-12 years old group and 19-45 years groups no correlation between Candida and DMFT/dmft, dental caries and fillings were observed (Table 2). Discussion Candida species constitute part of the oral microbiota. The prevalence of yeasts was higher in the studied population (68.55%) than in previous reports that related values between 30-38%20-21 and 40-60%10,22-23 in healthy individuals. The results on Candida species isolation are in accordance with the literature10,23 considering that C. albicans was the most prevalent species in all the studied groups. In the present study C. albicans represented 84.88% of Candida species. This data is in accordance to Jorge et al.24, Darwazeh et al.23 and Moalic et al.10 who found C. albicans as 73.75%, 80.8% and 93.7% of the isolated species, respectively. The studied population presented other species of Candida such as C. tropicalis (7.33%), C. krusei (1.83%), C. glabrata (0.91%), and Candida spp. (5.5%). Similar findings were reported by Jorge et al.24 who isolated 6.66% of C. tropicalis in saliva samples of Brazilian subjects, and according to Darwazeh et al.23 who isolated 2% of C. glabrata and 3% of C. krusei from Saudi healthy dentate subjects. Previous studies demonstrated that infection by Candida can be associated with some predisposing factors including high carbohydrate containing diet and poor oral hygiene25. In our study, a high sugar intake was observed for all the age groups. This could partially explain the high percentage of yeasts isolation in this population, considering that Vargas et al.26 found that dietary glucose intake is a determinant key for C. albicans growth in the gastrointestinal tract. Considering the group of ages between 6 and 12 years, DMFT/dmft value (6.63) can be considered high according to the mean DMFT, lower than 1, proposed by World Health Organization for the age of 12 in the year 201018. In our study, 33.57% of the individual between 6-12 years of age were positive for Candida in the oral cavity. This number was higher than the observed in previous studies. Souza et al.27 observed 17% of individuals positive for Candida in a population between 7 and 14 years of age. For this group, the positive correlation observed was between Candida presence and gender. Higher prevalence was observed among the females. Although salivary flow along can not be considered a key factor in fungi colonization10, reduced salivary flow has been related in the literature28 as a predisposing factor. In a previous study, Söderling et al.29 studying a population from 10 to 15 yearsold, reported that girls tended to have lower salivary secretion than boys. This could partially explain our findings on higher prevalence of Candida in girls. Considering the individuals between 13 and 18 years, a positive correlation between Candida and gender was not observed. This result is in agreement with Reynaud et al.30 that did not find any association between Candida and gender in subjects ³16 years of age. In the 13-18 years group Candida showed an association with caries prevalence. These data are in accordance with previous studies that also reported this correlation12,14,31. In fact, some authors suggested the use of Candida counts as a caries risk indicator2,5. In this age group, the presence of retentive surfaces, represented by decayed teeth and dental fillings, could be considered predisposing factors to Candida colonization. However it is important to emphasize that other predisposing colonization factor such as salivary flow rate, salivary pH, and salivary glucose contends were not evaluated. The mean value of Candida CFU/plate was higher in the group of 13-18 years, in relation to the other age groups. These results are not in accordance with the study of Parvinen and Larmas32 who reported higher prevalence of fungal colonization among adults in relation to younger groups. On the other hand, Williamson33 reported that children with less than 15 years of age presented higher fungal colonization in relation to adults and young adults. Our findings reinforce the multifactorial nature of the fungal colonization. Poor oral hygiene, low socioeconimic status and high levels of sugar intake could be contributed to the high prevalence of yeasts. The presence of Candida spp. in the oral cavity seem to be related and with past caries experience in young adults from 13 to 18 years of age. References
Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06015t2.jpg] [os06015f1.jpg] [os06015t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}