 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
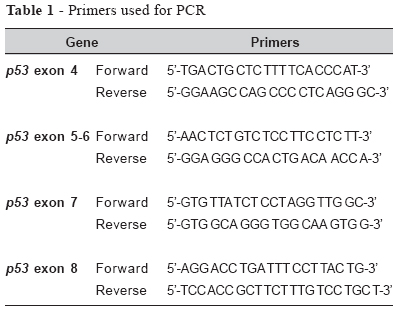
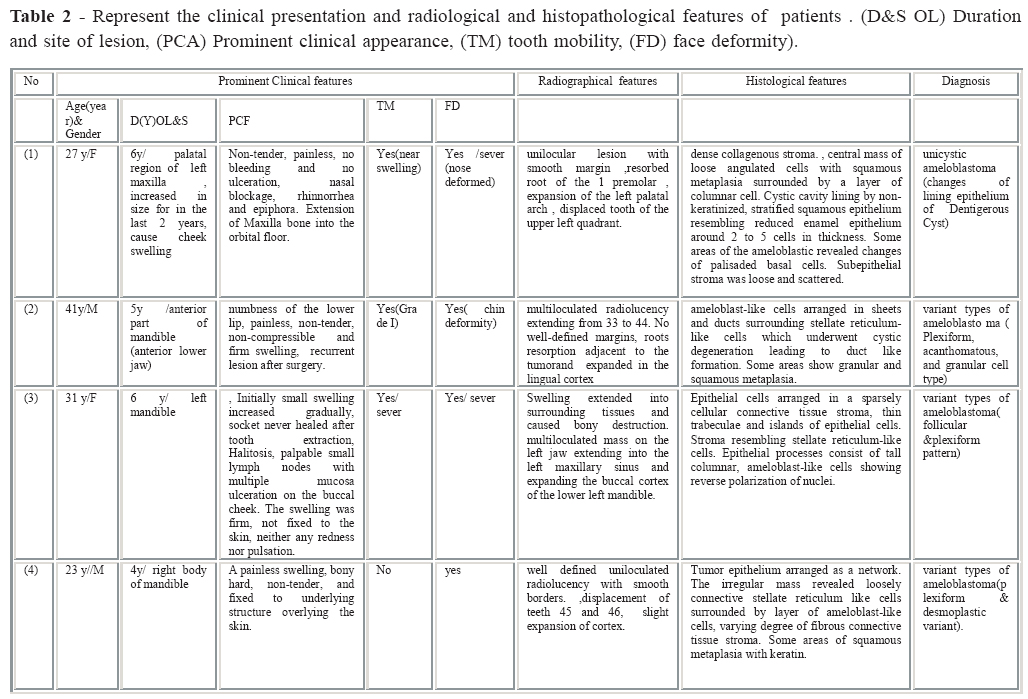
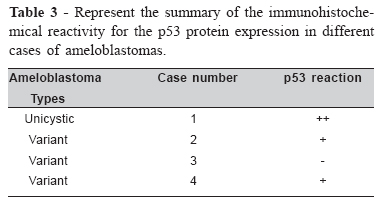
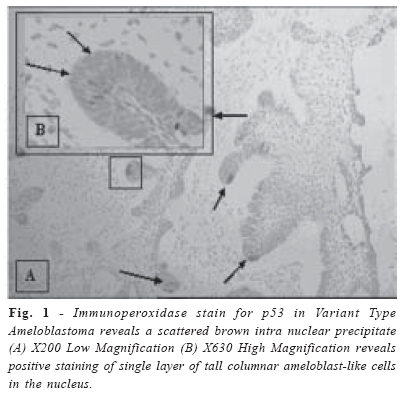
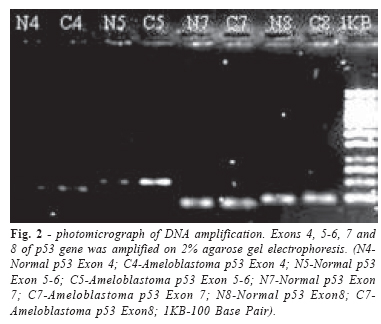
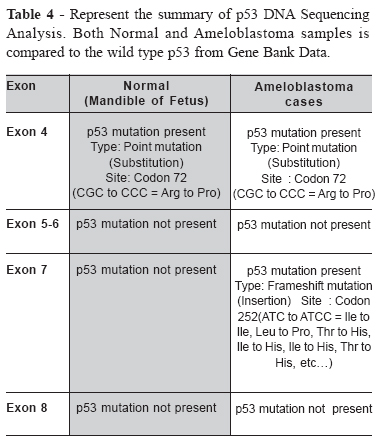
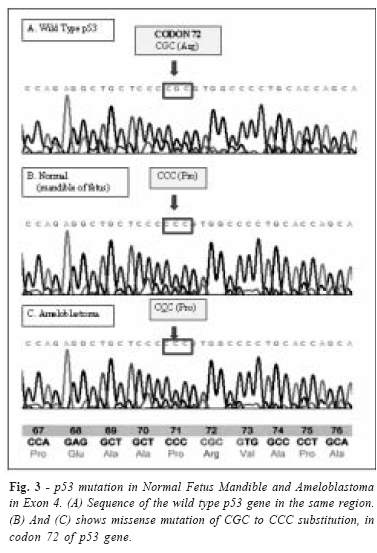
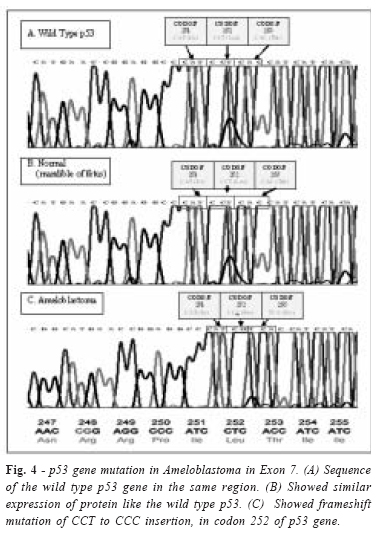
Brazilian Journal of Oral Sciences, Vol. 5, No. 17, Apr-June, 2006, pp. 1034-1040 P53 gene mutation and protein expression in ameloblastomas K. A. Al-Salihi1 Ling Yoke Li1 Azlina A.2 1School of Dental Sciences, Received for publication: January 30, 2006 Accepted: May 08, 2006 Code Number: os06020 Abstract P53 gene is commonly found to be mutated in human cancer. Currently, limited data exist on the occurrence of p53 gene mutation in ameloblastomas. This study designed to evaluate the expression of p53 proteins and their gene mutations in human ameloblastomas. Four cases of epithelial odontogenic tumors were used. Normal cells of a 7 months aborted fetus’s mandible were used as negative control. P53 Protein expression was detected immunohistochemically. DNA was extracted and amplified using PCR. Gene sequences analyzed to determine p53 mutation. p53 was overexpressed in one case of unicystic ameloblastoma and 2 cases of variant types of ameloblastoma. The Coding sequencing analyses demonstrated p53 gene alteration in cases of ameloblastoms in Exon 7 while, fetus epithelial mucosal cells showed the wild type DNA sequence in Exon 4. In conclusion p53 protein overexpression was detected by immunohistochemical staining as well as by DNA sequence analysis in cases of ameloblastomas. Key Words: ameloblastoma, p53, immunohistochemistry, mandible Introduction Ameloblastomas are an uncommon but most clinically significant benign odontogenic neoplasm of the oral region. Despite its relative rarity, it remains a subject of considerable interest, notably because of its locally invasive biological behavior, recurrence potential and the controversies regarding treatment modalities1, 2. Serial studies from Thailand 3, Singapore 4, and Japan 5 have identified the clinico-pathological characteristics of this neoplasm. In Malaysia, one main series on the distribution of this tumor in children 6 and isolated case studies have also been documented 7. The most common clinical finding is a non-tender slowly enlarging swelling 8, 9, 10,11,12,13 .It is now believed that neoplastic transformation, consisting of a multi-step accumulation of adverse genetic events, occurs in a wide variety of human tumors over a large region of the genome. Mutations in the p53 tumor suppressor gene are among the most common abnormalities in human cancer. The proto-oncogene product, p53, is a cellular protein expressed at low levels in non-transformed cells and acts as a negative regulator of cell division. Expression of p53 has been observed in normal epithelia, including the oral mucosa, and has also been detected in tissues of developing teeth 14, 15. In tumorderived and transformed cell lines the levels of p53 are often elevated and several investigators have suggested that inactivation of the p53 gene confers a selective advantage for the development of the tumorigenic phenotype with its subsequent impact on changing cellular activity 16. Few reports have dealt with the presence of p53 in ameloblastoma, while only few studies reported in the international literature consider ameloblastoma, as a tumor originating from p53 expressing odontogenic epithelium 14,15,16. This study focused on overexpression of p53 nuclear protein and gene mutation in ameloblastomas cases, to clarify the correlation between mutations within the specific regions of p53 gene, protein overexpression and clinical outcomes of patients. Materials and Methods Study Group The study comprised of 5 specimens of ameloblastomas which was case 1 (unicystic ameloblastoma (which was previously diagnosed as dentigerous cyst) and case 2, 3 and 4 of variant types. Four cases were retrieved from the archives of the Department of Oral Pathology, School of Dental Sciences, Universiti Sains Malaysia and 1 case was a fresh sample from the Operation Theatre 4, Hospital Universiti Sains Malaysia. Out of the 5 specimens, 2 were from the same patient (2) due to recurrence of the disease. Of the specimens, case 1 was from the maxilla (unicystic type) and 4 from the mandible (variant types). Radiological and histopathological features were re-evaluated for all cases. Control Group 1 normal mandible from a normal human fetus was obtained from the Department of Obstetrics and Gynaecology, Hospital Universiti Sains Malaysia. This has been approved by the Ethics and Research Committee, with reference USMKK/PPSP®/tindakan minit 149.6. Staining Procedures A 4mm thick serial sections were cut from the paraffin blocks; all tissues having been previously fixed in 10% neutral buffered formalin. Then, conventional haemotoxylin and eosin staining were done for the reevaluation and confirmation of the histological diagnosis. Immunohistochemical Study Immunohistochemical staining was performed using the IHC Select TM Immunoperoxidase Secondary Detection System (KIT, CHEMICON INTERNATIONAL Inc) uses biotin-avidin-HRP method. Briefly, 4mm thick serial sections were deparaffinized in xylene, hydrated and incubated with 0.5% (v/V) H2O2 in methanol for 20 min, to block the endogeneous peroxidase activity. Slides were then washed with Tris buffered saline (TBS, pH 7.4). The sections were placed on silanized glass slides for microwave antigen retrieval. The slides then immersed in 0.01 M citrate buffer (pH 6.0) and incubate for 5 min at 600W. Sections were then left to cool to room temperature and rinsed in TBS. Sections were stained according to instruction provided with the kit with a primary antibody: Mouse, Anti-Human p53 Protein (DO-7) (Dakocytomation, Cat# M7001). Sections were incubated overnight with primary antibody at dilution of . 1:300 in TBS at 40C. To observe a p53 –positive reaction, DAB substrate solution was used and counter-staining was performed with Meyer’s haemotoxylin. Primary antibody was omitted from negative control section for each experiment and replaced with non-human rabbit serum to shield against any false positive results which might develop from a non- specific reaction, Breast carcinoma sections were used as p53-positive control for each experiment. Immunohistochemical staining intensity was evaluated on a qualitative 2 point scale described previously 16. Dark, brownish, intranuclear precipitate reveals the positive overexpression of p53 protein while negative reaction reveals no staining. Polymerase Chain Reaction Analysis Specimens were collected for the DNA Analysis. The bone of the mandible of fetus was crushed and a slice of tissue from the other cases of ameloblastoma was taken. DNA extraction was performed using the QIAGEN® DNeasy Tissue Kit. Polymerase Chain Reaction (PCR) was then designed to amplify the p53 protein in genomic DNA using a MJ RESEARCH PTC-200 Peltier Thermal Cycler. The primers used in this study are included in TABLE.1. PCR was done in a total volume of 50 ìl containing 3 ìgl of genomic DNA. A PCR touch down technique was used. Touchdown PCR starts initially with an annealing temperature higher than the Tm of the primers and then during the early cycles of the PCR the annealing temperature is lowered gradually to below the Tm.. This ensures that only specific annealing of primers to their correct target sequence takes place before any nonspecific annealing events. For electrophoretical analysis, two per cent agarose gel was then prepared by diluting 1.0 g of MetaPhor® Agarose (BioWhittaker CAMBREX) in 50ml of Tris Boric EDTA (TBE) 1X by microwave for approximately 2 minutes at medium setting. An amount of 0.8ìl of SyBr green, a nucleic acid chelating agent, was then added and the mixture was swirled. The mixture was then poured onto a casket, the comb inserted, and cooled at room temperature for 15-30 minutes. When the gel has hardened, it is placed in the electrophoresis tank and covered with buffer TBE 1X 1-2 mm above its surface. Then 2 ìl of loading dye 6X was mixed with 1 ìl of each sample of PCR product and also the ladder/marker on parafilm. Loading dye was added to give color and weight to the DNA. Each sample was then loaded into the wells on the agarose gel and electrophoresis was done at 80V for 1hour. The gel was analyzed under UV light with the aid of the Alpha Innotech Corporation Image Analyzer. Results Clinical, radiological and histopathological findings Patients showed different types of ameloblastoma. Clinical presentation, radiological and histopathological features represent in table 2. Case 1 showed typical features of unicystic ameloblastoma. This case previously presented with lesion in the same area diagnosed as dentigerous cyst. The other 3 cases 2, 3, 4 were showed variant types of ameloblastoma. Which were Plexiform, Acanthomatous and Granular cell type in case 2, Follicular and Plexiform type in case 3 and Follicular and Plexiform type in case 4. Immunohistochemical reaction to p53 According to the classification used in this study, a positive staining would mean the presence of a dark, brownish, intranuclear precipitate. A negative reaction would not show any brownish staining. The results of immunohistochemical reactivity of p53 summarize in table 3. Immunohistochemical reactivity for p53 was detected in the nuclei of neoplastic odontogenic epithelial cells (Fig1 A&B ) The reaction was scattered in peripheral columnar or cuboidal cells in 3 of 4 samples (1,2,4). Only one sample (3) showed a negative reaction. Unicystic Ameloblastoma (case 1) showed a strong positive reaction of single layer of tall columnar ameloblast-like cells. The expression was more concentrated in the nuclei of these cells that were located at the opposite pole of the basement membrane. Cases 2, 4 showed a positive staining in the nucleus of the ameloblast-like cells. Sections of normal human fetus mandible did not show detectable p53 immunoreactivity. Negative control immunohistochemical staining of the mandible tissue which omitted the primary antibody showed no reaction. Mutation analysis of Tp53 gene DNA analyses of the 4 exons were carried out to find the mutation that probably occurs in the sequence. Exons 4, 5-6, 7 and 8 of p53 gene were amplified on 2% agarose gel electrophoresis (Figure 2). The sequencing analysis showed p53 gene mutant alleles in Exon 4 (both mandible of fetus and ameloblastoma) and Exon 7 (ameloblastoma only). There were no mutation present in Exon 5-6 and Exon 8 in both mandibles of fetus and ameloblastoma. Exon 7 in fetus of mandible did not reveal any mutation (table 4) .Exon 4 showed a homozygous mutation in which both the forward and reverse strands displayed a point mutation of substitution from CGC to CCC (base pair of G is substituted with C). This is found in Codon 72 where arginine (Arg) was replaced with proline (Pro) (Figure 3). There was a presence of heterozygous mutation in Exon 7 found in the reverse strand. The mutant p53 gene displayed the type frameshift mutation, where the C is inserted in Codon 251. The insertion causes the subsequent expression of amino acid to be changed (Figure 4). Discussion Odontogenic tumors comprise a complex group of oral pathologies, with diverse histopathological forms and clinical behaviors17, 18. These lesions contain epithelial and/or mesenchymal derived elements that may even be capable of recapitulating normal odontogenesis19, 13.Ameloblastomas are the most common human odontogenic neoplasia and although typically considered locally invasive and benign, they frequently recur subsequent to surgical resection (55–90%) and can even occasionally undergo malignant transformation. 20-23. The odontogenic origin of ameloblastomas is derived from many similarities in the histological appearance of the tumor and a developing tooth organ. 24 Possible origins of the neoplastic epithelium are discussed to be either disturbances of the developing enamel organ or the epithelial lining of odontogenic cysts, particularly the dentigerous cyst, and odontomas or cell rests of the enamel organ, namely either remnants of the dental lamina or remnants of Hertwig’s root sheath (epithelial cell rests of Malassez) or the basal layer of the oral surface epithelium (epithelium of the jaws). This distinctive semimalignant, unicentric, nonfunctional, persistent odontogenic neoplasm shows intermittent or slow growth. The proliferating tumor may infiltrate the cancellous marrow spaces without causing bone destruction. It tends to expand the bone rather than perforate it. Occasionally patients allow an ameloblastoma to persist for many years without treatment and though the expansion may become extremely disfiguring, the tumor does not break through the bone. But for reasons unknown some ameloblastomas manage to penetrate the bone and extend into the surrounding soft tissues. Local extension to the base of the skull is life-threatening. 25 Very rarely ameloblastomas develop distant metastases. Our patients were presented with different types of ameloblastoma. Only one presented with unicystic ameloblastoma, while the 3 other patients presented with variant types of ameloblastoma. The unicystic variety of ameloblastoma usually presents itself at a younger age group of 1st to 2nd decade of life and has a significant male preponderance where as our patient was a 27 year old female. Unicystic ameloblastoma typically contains a tooth and appears radiographically as a dentigerous cyst. These radiological and histological criteria’s however were presented in our patient. The variant type of ameloblastoma was presented in the other 3 patients. All these patients presented clinical and radiographical features typically as mentioned in previous published cases26, 27, 28. Due to invasiveness and a rare chance of metastases of ameloblastomas, the tumor has been subject to definition from a benign odontogenic epithelial tumor to a slow-growing malignant tumor 15. Pulmonary metastasis is probably a result of aspiration of tumor cells associated with surgery, particularly in cases having undergone multiple operations due to recurrences. This aspect is being discussed here as one of our patients showed recurrence. Other authors dispute to which extent the various histological patterns of a simple ameloblastoma accompany a distinctive variation in clinical behavior 29. Immunohistochemistry is widely used for diagnosis of cancers. In our patient immunohistochemical staining for p53 was positive in the unicystic ameloblastoma and 2 variant cases of ameloblastoma and only one case failed to reveal any immunoreactivity to p53 protein. Our results show that all cases of ameloblastoma might express p53 protein. However, laboratory procedures such as antigen retrieval technique may also interfere with the results and quality of immunohistochemistry. Our results indicate that p53 overexpression is not the only pathogenesis factor in odontogenic tumour; although it plays a major role in their pathogenesis. The odontogenic epithelial cells of control tissue (fetus) revealed negative p53 immunoreactivity, probably due to one fact that the wild type protein of p53 does not normally accumulated to amount detectable by immunohistochemical methods because of its short half –life (6-20 minutes). The result of our study is compatible with other few previous reports 16, 30. In our study the number of p53-reactive cases is compatible to results from the two other previous published studies of p53 expression in ameloblastoma16, 31. The p53 gene also known as TP53 codes for a protein that regulates the cell cycle and hence functions as a tumor suppressor. It is very important for cells in multicellular organisms to suppress cancer. P53 has been described as “the guardian of the genome”, referring to its role in conserving stability by preventing genome mutation. The only recent molecular biological studies analyzed molecular genetic alteration of p53, MDM2, and p14ARF in association with immunohistochemical findings on ameloblastomas suggested that elevated expression of p53, in benign and malignant ameloblastomas suggests that alteration of the p53- MDM2-p14ARF cascade is involved in oncogenesis and /of malignant transformation of odontogenic epithelium. P53 gene status implied that p53 mutation might play a minor role in neoplastic changes of odontogenic epithelium. Immunoreactivity for p53, MDM2, and p14ARF in ameloblastoma variants suggests that these factors might be associated with tissue structuring and cytodifferentiation of ameloblastomas32. According to our results, the mutations of the p53 gene were found in the sequencing analysis in Exon 4 in both mandible of fetus and ameloblastoma which is consider as a homozygous mutation in which both the forward and reverse strands displayed a point mutation of substitution from CGC to CCC (base pair of G is substituted with C). This is found in Codon 72 where arginine (Arg) was replaced with proline (Pro). There were no mutation present in Exon 5-6 and Exon 8. In Exon 7 the mutation found in the reverse strand in ameloblastomas cases only. The mutant p53 gene displayed the type frameshift mutation, where the C is inserted in Codon 251. The insertion causes the subsequent expression of amino acid to be changed. In exon 7 of the mutant p53 gene, a frameshift mutation has occurred. A frameshift mutation is a mutation that inserts or deletes a single nucleotide from a DNA sequence, for this instance, inserts a single nucleotide. This is found in Codon 251 where ATC to ATCC occurred. Due to the triplet nature of gene expression, the insertion has disrupted the grouping of the codons, resulting in a completely different translation from the original. From the DNA new sequence of the mutant p53 gene, RNA will be transcripted. RNA will then be translated to a protein that has no role in its original tumor suppressor function. The frameshift mutation in Exon 7 of mutant p53 gene totally resulted in a different translation of protein from the original. Hence, an abnormal non-functional tumour suppressor is expressed and is unable to arrest or suppress the proliferation of the disease.The observations found in our study is inconsistent with Kumamoto et al 2004. They found that mutional alteration was not detected in p53 gene exons 5-8, including hotspot codon 175, 245, 248, 249, 273, and 282 in any of the 11 cases31. Thus far, and according to comprehensive review of literature we couldn’t find any report about mutations in p53 gene in ameloblastoma. This study might be the first to report this new finding the mutations in p53 gene supported by immunohistochemical p53 protein overexpression in ameloblastoma. Having found these valuable findings in this study, p53 mutation analysis can be used as a potential therapeutic. Anti-p53 agent could be considered to reduce the size of large tumors and to treat unresectable tumors that are in close proximity to vital structures. Acknowledgments All people working in genome center Universiti Sains Malaysia are gratefully acknowledged. References
Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06020t3.jpg] [os06020t1.jpg] [os06020t2.jpg] [os06020t4.jpg] [os06020f3.jpg] [os06020f2.jpg] [os06020f1.jpg] [os06020f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}