 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
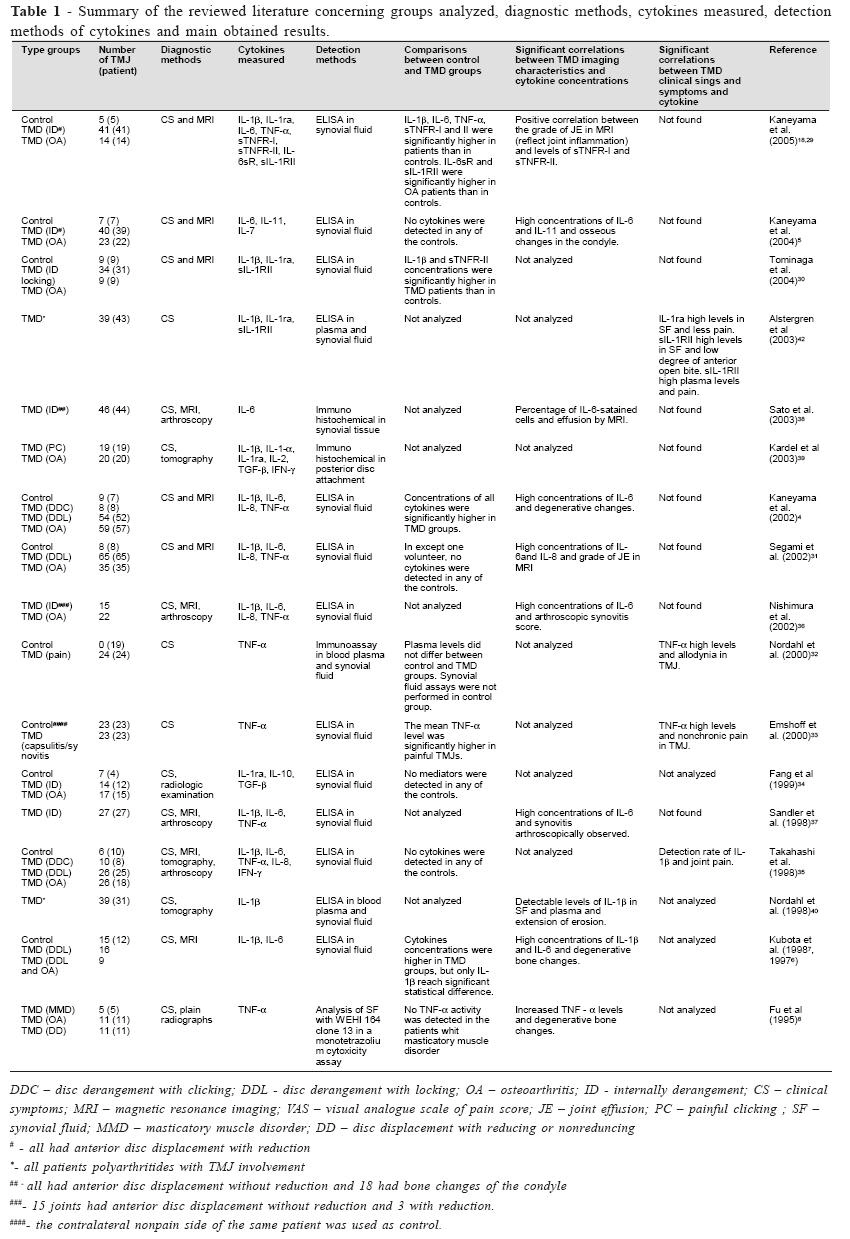
Brazilian Journal of Oral Sciences, Vol. 5, No. 18, July-September 2006, pp. 1054-1062 Inflammatory cytokines activity in temporomandibular joint disorders: a review of literature Maria Isabela Guimarães Campos 1 Paulo Sérgio Flores Campos2 Sergio Roberto Peres Line3 1DDS, Department of Morphology, Dental School of Piracicaba, State University of Campinas, Piracicaba, SP, Brazil. Assistant Professor, Department of Biomorphology, Institute of Health Sciences, Federal University of Bahia, BA, Brazil Received for publication: April 03, 2006 Code Number: os06023 Abstract Cytokines are important polypeptides mediators of acute and chronic inflammation. These molecules act as a complex immunological network, in which there are pro-inflammatory cytokines, such as interleukin-1 (IL-1), IL-6 and tumor necrosis factor-a (TNF-a), and anti-inflammatory mediators like IL-10 and transforming growth factor-b. In spite of some controversial findings, in general high levels of pro-inflammatory cytokines have been correlated with signs and symptoms of temporomandibular disorders (TMD) such as internal derangement and osteoarthritis. These mediators promote degradation of cartilage and bone joint by inducing release of proteinases and other inflammatory molecules. Indeed, pro-inflammatory cytokines have been associated with temporomandibular joint (TMJ) tissue destruction. However, its mechanisms and pathophysiology have not been clearly delineated. In attempt to summarize the role of cytokines in TMD pathophysiology and its potential for medical intervention, the purpose of the current study was to review the literature concerning the analysis of these inflammatory mediators in TMJ fluid and tissues. Key Words: TMJ, temporomandibular joint disorders, osteoarthritis, cytokines, interleukins Introduction The temporomandibular joint disorders (TMD) are a common source of chronic orofacial pain. However, there is not sufficient knowledge about the pathopysiologic mechanisms that underlie the development of local joint destruction and clinical symptoms. Pro-inflammatory cytokines are important mediators of acute and chronic inflammation, being associated with joint destruction in osteoarthritis (OA) and rheumatoid arthritis (RA)1-3. Among several pro-inflammatory cytokines, interleukin-1b (IL-1b), IL-6, and tumor necrosis factor-a (TNF-a) are present at elevated concentrations in the synovial fluid of temporomandibular joints (TMJs) with internal derangement and/or bone changes, reflecting a TMJ behavior similar of other synovial joints4-8. These cytokines promote degradation of cartilage and bone joint by inducing release of proteinases and inflammatory mediators, suggesting its important role in the pathogenesis of TMD6-7,9-11 . L-6 is a multifunctional cytokine with a central role in host defense12 and can be produced by many cell types, such as monocytes/macrophages, T cells, fibroblasts and endothelial cells13-15. IL-6 plays an important role in the enhancement of T-lymphocyte proliferation, B-lymphocyte differentiation and complement cascade activation16. In addition, this cytokine also acts synergistically with IL-1b, inducing bone resorption17. The biological activities of IL-6 occur after binding of the cytokine to its receptor complex consisting of two molecules, IL-6 receptor (IL-6R) and gp 130 (signal transducing protein). Proteolytic cleavage of IL6R originates a soluble receptor (sIL-6R) that acts as an IL6 agonists, binding IL-6 and potentiating its affinity to IL-6 receptor complex18. IL-11 is a novel cytokine that belongs to the IL-6 family and exerts similar functions of IL-6, like acting on osteoclastogenesis5. Tumor necrosis factor-a is a potent mediator of immuneinflammatory response, mainly produced by macrophages19. This factor seems to have similar biological effects as IL-1. It has been shown to induce the secretion of collagenase20, prostaglandin E221 and interleukins, such as IL-6 and IL-822. TNF-a has also been reported to induce bone resorption in vitro and in vivo23-24. In addition, elevated levels of this cytokine have been associated with several diseases25-26. TNF-a binding to its specific cell surface receptors also is required to initiate its biological actions. These receptors, tumor necrosis factor receptor I (TNFR-I) and tumor necrosis factor receptor II (TNFR-II), present soluble forms, sTNFR-I and sTNFR-II, identified in human serum and in synovial fluid. In contrast to sIL-6R, sTNFR-I and sTNFR-II act as cytokine antagonists, neutralizing biological activities of TNF-a by competing with the membrane receptor for cytokine binding18. The interleukin-1 family of cytokines consists of three polypeptides: IL-1a, IL-1b and IL-1 receptor antagonist (IL1ra). IL-1a and IL-1b are pleiotropic cytokines that posses a wide spectrum of inflammatory and immunological activities27. These pro-inflammatory cytokines can cause strong stimulatory effects on bone resorption and inhibitory effects on bone formation and its elevated levels have been correlated with diseases that reflect inflammatory states27-28. IL-1ra is a natural antagonist of both IL-1a and IL-1b by competing for binding to IL-1 receptors without induction of signal transduction. The three polypeptides of IL-1 family bind to two distinct high-affinity receptors, IL-1 receptors type I and type II (IL-1RI and IL-1RII)27. In addition, soluble forms of IL1RII (sIL-1RII) identified in sera and synovial fluid can bind to the precursor form of IL-1b and inhibit its processing to the active form18. Several studies (table 1) have been conducted to prove if cytokines analysis of synovial fluid can reflect the clinical status and imaging characteristics of TMD. The aim of this review is compare the findings of multiple investigations to understand the role of these cytokines in TMD pathophysiology and its potential for medical intervention. Results In all studies that compared control and TMD groups, the synovial fluid of healthy control subjects presented undetectable or significantly low levels of pro-inflammatory cytokines when compared to TMD patients4-7,18,29-35. In general, elevated IL-6 concentrations or expression were correlated with TMD imaging characteristics that reflect inflammation and bone changes. This cytokine had a significant relation with arthroscopic synovitis score36-37 and degree of joint effusion shown by MRI31,38. Concentrations of IL-6 were significantly higher in joints with bone changes in condyle, like flattening, osteophyte formation or erosion45,7. Additionally, IL-6 and IL-11 when detected together were significantly correlated with osseous changes in the condyle5. Kaneyama et al.18 observed significantly higher concentration of IL-6 soluble receptor (sIL-6R) in osteoarthritis group than in control group. TNF-a elevated levels in the synovial fluid of TMJs were significantly correlated with allodynia32 and nonchronic pain33. In addition, increased TNF-a levels were associated with degenerative bone changes8. Besides the evidence that TNFa and its receptors were significantly higher in he synovial fluid of patients than controls, Kaneyama et al.18 found that TNF-a level was positively correlated with those of IL-6, sTNFR-I and TNFR-II. In addition, concentrations of TNF-a and IL-6 correlated with the detection of IL-8 in synovial fluid of patients with DTM4. Comparing cytokine staining in the posterior disk attachment area between patients with painful clicking and OA of the TMJ, IL-1a and b predominated in both groups, with OA group showing the higher scores39. IL-1b significant high concentrations were observed in synovial fluid of TMJs presenting radiographic images of degenerative bone changes6-7 and detectable levels of IL-1b were associated with extension of radiographic erosion in TMJ40. Expression of this cytokine was significantly correlated with arthralgia and TMJ sound41. IL-1ra was found with higher detection rate and concentration in controls than in TMD patients, but without significant difference18,30. In addition, a high concentration of IL-1ra was detected in synovial fluid of TMJs with less pain42. Interestingly, a higher ratio IL-1b/IL-1ra was observed in the TMD group than in control group30. Controversially, Fang et al.34 detected high levels of IL-1ra and TGF-b in synovial fluid of ID and OA TMJs, while it were undetectable in normal controls. In addition, IL-10 was undetectable in both normal and diseased joints. Regarding the IL-1 soluble receptors, significant increased level of sIL-1RII was observed in TMD group (including patients with OA or ID)30, while Kaneyama et al.18 observed significant higher concentrations of sIL-1RII in only osteoarthritis group than in control group. Additionally, in TMD group sIL-1RII was positively correlated with IL-1b in synovial fluid30. Analysis of plasma and synovial fluid from polyarthritides patients with TMJ involvement revealed higher concentrations of IL-1ra in synovial fluid than in plasma, whereas the opposite condition was found for sIL1RII. In addition, high levels of IL-1ra in synovial fluid were correlated with less pain, sIL-1RII high levels in synovial fluid were associated with low degree of anterior open bite and its high plasma levels were correlated with more pain42. Table 1 presents a resume of the reviewed literature concerning analyzed groups, diagnostic methods, cytokines measured, detection methods of cytokines and main obtained results. Discussion Despite the differences in methodology, in all articles that presented control groups the levels of pro-inflammatory cytokines were significantly increased in synovial fluid of TMD patients than in healthy control subjects4-7,18,29-35. This finding reflects an effective role of these cytokines in the pathogenesis of TMD and a TMJ behavior similar to other synovial joints that are affected by OA or rheumatoid arthritis43. The literature showed that elevated IL-6 concentration or expression were more correlated with TMD imaging characteristics that reflect bone changes than with clinical sings and symptoms of TMD4-5,7. Controversially, Sato et al.38 found no significant relation between IL-6 expression in synovial tissue and degenerative bone changes. It could be explained by a few numbers of joints (18) with bone changes analyzed by Sato et al.38 compared to 59 joints with OA evaluated by Kaneyama et al.4. Additionally, IL-6 concentration in synovial fluid cannot be always correlated with its expression in synovial tissues. Immunohistochemical analysis in synovial tissue of TMJs showed IL-6 expression in the cells lining the synovium and the mononuclear cells infiltrating the periphery of the blood vessels, clarifying the origin of this cytokine in TMJ38. sIL-6R concentration was found significantly higher in osteoarthritis group than in control group, since sIL-6R acts as IL-6 agonist, this result reinforces the role of IL-6 in TMD18. Elevated concentrations of IL-6 and its soluble receptors in synovial fluid of patients with bone changes suggests an effective role of this cytokine in the development of osteoarthritis in TMJ, even without significant correlation between this cytokine and clinical symptoms4-5,18. In addition, several authors reported high prevalence, ranging from 50% to 90%, of osteoarthrotic radiographic signs in asymptomatic TMJs33,44. Only Fu et al.8 found a correlation between TNF- a high levels and imaging of degenerative bone change. This cytokine seems to be more correlated with sings and symptoms of inflammation in TMD. Elevated levels of TNFa in synovial fluid were correlated with arthralgia of the TMJ32,33 and histological grading of synovitis was significantly correlated with the intensity of TNF-a expression in synovial tissues45. TNF-a seem to play a significant role in the onset of TMJ inflammation, since TNF-a and its two receptors levels were increased in TMJ tissues after two days of arthritis inducement with complete Freund’s adjuvant. Interestingly, in this same study46 gene microarray and RT-PCR analysis demonstrated elevation in gene and mRNA expression for only TNF-a and TNFR-I. It was found that TNF-a concentrations in synovial fluid of TMD patients could be correlated with the concentrations of sTNFR-I and sTNFR-II which were upregulated and correlated with each other. Since TNF- is an important inducer of the sTNFRs, increased concentrations of TNF-a and its soluble receptors may also reflect pathogenesis of the TMD18. In patients with chronic connective tissue disease presenting TMJ involvement TNF-a levels in TMJ synovial fluid were significantly higher than its plasma levels, reflecting the important role of local cytokine production 32. Although IL-1b and are produced in inflammation by stimulated monocytes and macrophages, most of IL-1a remains intracellular or on the surface of the cell membrane, while most of IL-1b is transported out of the cell27. Elevated levels of IL-1b in synovial fluid of TMD patients might have synovial and endothelial cells as its main cellular source41. IL-1b significant high concentrations were observed in synovial fluid of TMJs presenting radiographic images of degenerative bone changes6-7 and detectable levels of IL-1b were associated with extension of radiographic erosion in TMJ40. In addition, expression of this cytokine was significantly correlated with arthralgia and TMJ sound41. IL-1b and a were the main cytokines expressed in TMJ tissue of patients with OA or painful clicking, however the OA group expressed a more complex cytokine pattern, involving not only pro-inflammatory cytokines, such IL-1, TNF-a and interferon-g (INF-g), but also IL-1ra and TGF-b, which are anti-inflammatory mediators acting in repair mechanisms39. Fang et al.34 also found significant high concentrations of TGF-b in OA joints compared to ID joints. These findings were confirmed with observations during TMJ surgery, where in OA patients were observed signs of both tissue destruction and repair39. IL-1ra was found with higher detection rate and concentration in controls than in TMD patients, but without significant difference18,30. In addition, a higher ratio IL-1b/ IL-1ra was observed in the TMD group than in control group30. These results suggest that the local balance between IL-1b and IL-1ra is important in TMJ inflammation. Other interesting finding is that in both studies18,30 there were substantial amounts of IL-1ra in synovial fluid of either controls and patients, confirming that it is required 5 to 100fold excess amounts of IL-1ra over IL-1b for inhibition of IL1 activity47. Controversial results were obtained by Fang et al.34 that found a high concentration of IL-1ra in 94% of the TMD patients, while the mediator was not detected in controls. These different results could not be explained, since the same assay methods and immunoassay kits were used. IL-1ra is a natural antagonist of IL-1, its detection in patients could be justified as TMD progresses, since IL-1ra should be increased to protect the host against IL-1b activity in excess18. In an animal TMJ arthritis model, Habu et al.48 showed that IL-1ra is produced by the same cell sources of IL-1b, such as macrophages, synovial cells and chondrocytes. Alstergren et al.42 found a three-fold higher IL-1ra level in TMJ synovial fluid than in plasma in polyarthritides patients with TMJ involvement. In addition, a high concentration of IL-1ra was detected in synovial fluid of TMJs with low intensity of pain. These findings suggest that IL-1ra may be mainly produced locally and may control TMJ local symptoms. Regarding the IL-1 soluble receptors, that are considered IL1 antagonists, significant higher concentrations of sIL-1RII were found in synovial fluid of TMD patients than in controls18,30 and it were correlated with low degree of anterior open bite42. Additionally, in TMD group sIL-1RII was positively correlated with IL-1b in synovial fluid30. In the same way of TNF soluble receptors, sIL-1RII may increase in an autocrine or paracrine manner in response to increasing levels of IL-1b in TMD. Interestingly, there were substantial levels of sIL-1RII in synovial fluid of both controls and patients in comparison with IL-1 or IL-1ra levels18,30, probably excess amounts of this soluble receptor is required to its appropriate activity. Therefore, measurement of cytokines soluble receptors or antagonist receptors in synovial fluid could be more accurate to assess disease activity. The interrelation of cytokines activities suggests they act as complex immunological network, in which cytokines can be regulated by others cytokines. Kaneyama et al.18 found that TNF-a concentration in synovial fluid were correlated with the concentrations of IL-6. These authors suggested that TNF-a is in the apex of cytokine network involved in pathogenesis of the TMD, since inhibition of this cytokine reduced the actions of other pro-inflammatory cytokines, such as IL-6, IL-1 and IL-8. IL-8 is also a pro-inflammatory cytokine with multifunctional actions in acute and chronic inflammation, mainly presenting chemotactic activity49. Segami et al.31 also found a close relationship between the concentrations of IL-6 and IL-8 in the synovial fluid of the same patients, suggesting that these cytokines might be activated in cooperation with each other in TMJ disorders. Concentrations of IL-6 and TNF-a were higher in the detected IL-8 joints than in ones that it was not detected. It was speculated that IL-8, produced by stimulation of TNF-a, activates the release of IL-6 by T lymphocytes into the TMJ4. Additionally, it was found that IL-1b could stimulate IL-8 and IL-6 production, through an increase in IL-8 and IL-6 gene expression in synovial cells from human TMJ49-50 . Analysis of TNFa and IL-b in 33 biopsies of synovial tissues from patients with symptoms of anterior displaced and nonreducing discs demonstrated a similar location for both cytokines, in the synovial lining cell layer and the blood vessels. In addition, a statistically significant correlation between the intensity of cytokines expression was also observed45. This finding supported that the same cells may produce TNF-a and IL-b in response to the same stimulus. The TMJ of a transgenic mouse that over expressed the human form of TNF-a showed an early occurrence of inflamed synovium and subsequent structural changes reflecting a degenerative joint. Furthermore, the disc and articular cells expressed IL-1b and MMP-911. Antigen-induced arthritis in a rabbit TMJ model showed an acute stage with one week of duration after induction. In early phase of acute stage, infiltrating inflammatory (polymorphonuclear leukocytes and few macrophages) and superficial synovial cells were the main source of IL-1b and IL-1ra, while in late phase the cytokines were mainly expressed by subsynovial fibroblasts with no involvement of chondrocytes. However, in the chronic stage chondrocytes and hyperplasic synovial cells were the main source of IL-1b and IL-1ra, suggesting that the cellular sources of cytokines change according to the stage of inflammation48. Another investigation51 using an adjuvant model of TMJ inflammation demonstrated that the IL-b and TNF-a peak concentrations were seen at two days, with significant reductions observed at two and four weeks, respectively. Although IL-b and TNF-a early peak, it maintain high levels in TMJ tissues through five weeks, maintaining a persistent inflammation51. Indeed, several inflammatory mediators act during TMD development, however each mediator may play a significant role during different stages in the onset and exacerbation of the inflammatory process. According to the findings of the reviewed literature, it can be postulated that in TMJ arthritis development IL-1b and TNF-a seem to be earlier produced, presenting as important role in the destruction of cartilage by degradation of proteoglycan mediated by matrix metalloproteinases activity. As a result, these cytokines are more correlated with clinical symptoms of inflammation, such as pain (table 1). In other hand, IL-6 production, mainly induced by IL-1b and TNF-a, seems not has important role in inducing matrix metalloproteinases synthesis. Therefore, IL6 may be more relevant inducing bone resorption in later disease stages. The association between IL-6 high levels and radiographic images of degenerative bone changes can confirm this hypothesis (table 1). The results of correlations between pro-inflammatory cytokines and signs and symptoms of TMD differ between several studies analyzed (table 1). These contrasts could occur by differences in the sampling procedures, assay methods, patients and controls. Despite using the same immunoassay kits, some studies showed discrepancies in sensitivity when their results were compared for the same cytokine (table 1). It was suggests that reproducibility of these assays can vary between different laboratories18. Therefore, bioassay may be affected by other factors in the biological specimens18. The lack of correlations between proinflammatory cytokines and signs and symptoms of TMD could be explained by patient’s use of nonsteroidal antiinflammatory drugs or by a rapid turnover of these mediators that promotes varied concentrations in synovial fluid and tissue over the time. In addition, it is thought that cytokine receptor antagonists have a role in the pathogenesis of TMD, the presence of these antagonists could also explains the absence of correlation between proinflammatory cytokine concentrations and TMD clinical variables18,30,39,42. Measurement of inflammatory mediators in synovial fluid seems to be of important value for diagnostic and therapy of temporomandibular disorders. Synovial fluid analysis of 103 joints before undergoing arthrocentesis treatment revealed that unsuccessful joints had high detection ratio of IL-6 and raised concentrations of IL-1b in comparison to successful joints52. It suggests that cytokines monitoring could be useful not only to evaluate the extent of the disease, but also to indicate a possible treatment prognostic. In acute cases, lavage to remove these cytokines could relief the clinical problems of TMD. Additionally, these mediators might be good therapeutic targets for the prevention of bone and cartilage destruction. The pathophysiology behind TMJ pain and dysfunction is not completely understood. Pro-inflammatory cytokines are important immune mediators that confer protective effects to the host, and the production of specific endogenous inhibitors, such as soluble receptors or receptors antagonists, acts as a mechanism to counterbalance the cytokines proinflammatory effects. Indeed, disease is believed to result when a cytokine imbalance occurs, either from persistent local elevation of pro-inflammatory cytokines or from inadequate activity of natural anti-inflammatory mechanisms, leading tissue destruction1,27. Therefore, pro-inflammatory inhibitors such as TNF soluble receptors, receptor antagonists (IL-1ra) and inhibitory cytokines (IL-10) could be used as novel therapy agents to control inflammation, prevent connective tissue destruction and bone loss in synovial joints, like TMJ53. These kind of therapies have been used with success in experimental studies and is already in clinical practice53-54. Nevertheless, it was observed interindividual and intra-articular variation of both quantities and profiles of expressed cytokines in patients with rheumatoid arthritis presenting similar macroscopic and histophatological features of inflammation. This finding could explain the wide variation in responsiveness to different modes of antirheumatic treatment between patients55. Some polymorphisms, which are genetic variations considered biologically normal, can alter gene expression and function, causing an effect on the individual’s phenotype and conferring susceptibility to diseases56. Polymorphisms have been described in genes of cytokines such as IL-1b, IL1ra, IL-6 and TNF-a. These are functional gene polymorphisms, since it can alter the cytokines expression and is related to several diseases, including osteoarthritis and rheumatoid arthritis57-60. Individuals may demonstrate consistent differences in cytokine secretion61, which are probably genetically predetermined62. The process of progression and symptomatic phenomena of TMD may be different in each individual. Indeed, there are people presenting disc displacement or bone degenerative radiographic images without dysfunction or pain and there are also patients with persistent TMD symptoms after conventional or surgical treatments. Could cytokine polymorphisms contribute to these differences? It is of great value study the hypothesis if cytokines polymorphisms could be associated with severity or progression of the TMD. This kind of study, under way by our research group, would lead to a more specific treatment of patients and, in future, individual therapeutics could be developed, improving the treatment options of TMD. References
© Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06023t1.jpg] |
| |||||||||

{kind=link}