 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
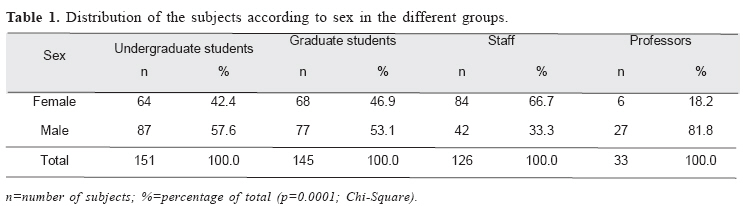
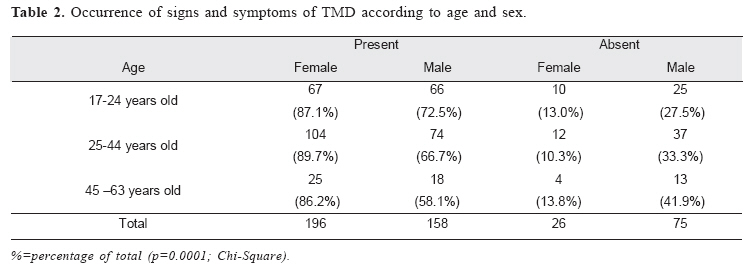
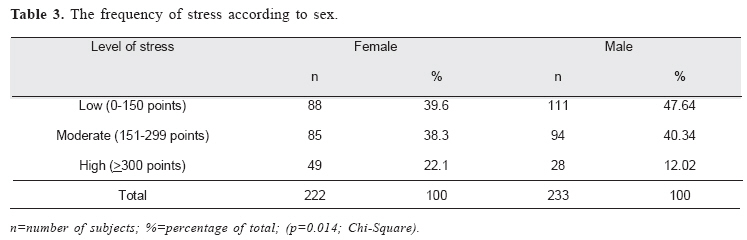
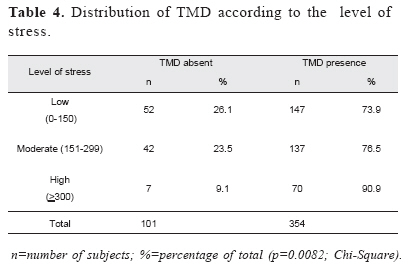
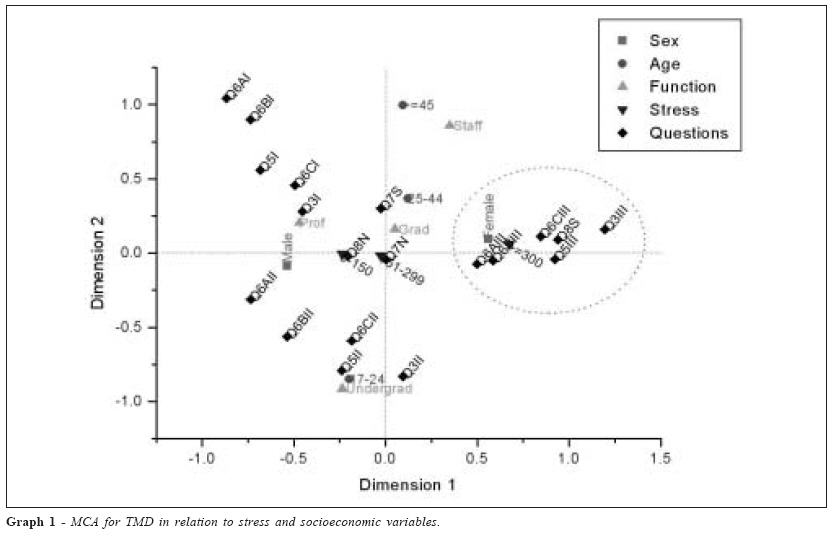
Brazilian Journal of Oral Sciences, Vol. 5, No. 18, July-September 2006, pp. 1074-1078 Environmental stress and temporomandibular disorder (TMD) among members of a public university in Brazil Ana Paula Sereni Manfredi1 *, Paula Próspero Borelli Bortolleto2 *, Ariovaldo Armando Da Silva3*, Izilda Esmênia Muglia Araújo4 *, Sebastião Araújo5 *, Laércio Luis Vendite6* 1MD,Dental surgeon, CSS/CECOM, Specialist in Orofacial Pain and Temporomandibular Disorders, Master of Ciências Biomédicas by Faculdade de Ciências Médicas, Universidade Estadual de Campinas (UNICAMP), Campinas, SP, Brazil. Received for publication: May 29, 2006 Code Number: os06026 Abstract Temporomandibular disorder (TMD) is one of several somatic manifestations of stress. Several studies have shown that some patients with TMD suffer more anxiety than individuals without this condition. The aim of this study was to identify individuals with TMD and correlate with environmental stress among members of a public university. A proportional stratified probabilistic procedure was used to select 455 subject’s age 17-63 yrs consisted of students, staff and professors. The subjects were enlisted after lunch. TMD were diagnosed using a screening questionnaire based on the American Academy of Orofacial Pain (AAOP). Presence of TMD was defined based on pain in chewing or speaking, tired maxillae and pain in the head, neck and/or teeth. Environmental stress was diagnosed by using the Social Readjustment Rating Scale (SRRS).Gender distribution was similar among undergraduate and graduate students, but there were significant differences in the sex ratio of university staff (66.7% were females) and professors (81.8% were males). Prevalence of TMD influenced by stress among women was significantly greater than in men of the same age group (p=0.0001), and almost all individuals (90.9%) with TMD had a high level of stress (p=0.0082). These findings suggest that there is positive association between TMD and environmental stress. Key Words: orofacial pain, questionnaire, stress, temporomandibular joint Introduction Temporomandibular disorders (TMD) have been extensively investigated in the last ten years, and several hypotheses have attempted to integrate studies on the etiology, diagnosis and prognosis of these craniofacial pains1. TMD can be classified according to the signs and symptoms of the affected region, and the patients may present pain in the musculature of the stomatognathic system, mainly in masseter, temporal, medial and lateral pterygoids muscles. These pains, which may be present during masticatory functions, speaking or opening and closing of the mouth, are referred to as myalgia disorders. Noises within the temporomandibular junction (TMJ) and mouth opening limitation and deviation on maximum opening are manifestations of internal disorders2-3. The etiology of TMD has been attributed to muscular inflammatory processes, alterations in the positioning or in the number of teeth and their occlusion, local facial and cranial trauma, and whiplash. However, none of these factors acts alone, and it is always necessary to investigate the patient’s adaptive capacity, particularly since the occurrence of TMD is closely related to the individual’s emotional wellbeing4. TMD is one of several somatic manifestations of stress5, and some patients with TMD suffer more anxiety than individuals without this condition6. In the former group, stress-related emotional factors acting on specific anatomical structures can function as coadjutants in TMD patients. Most patients generally have a large number of symptomatic manifestations7 that can confound and complicate the diagnosis. Hence, TMD must be considered as having multiple rather than simply dental causes8. The aims of this study were to: a) identify individuals with extracapsular TMD in a population of students, staff and professors at a public university in the state of São Paulo, Brazil, b) assess the level of environmentally-induced stress in these individuals, c) evaluate the extent to which stress initiated or modified TMD of muscular origin, and d) compare the results obtained among the subjects in this study. Material and Methods This study was done at the State University of Campinas (UNICAMP), in Campinas, in the State of São Paulo, Brazil, and was approved by the institutional Ethics Review Board (protocol number 168/2000). Informed consent was obtained from all subjects prior to participation in the study. Subject selection According to the university’s General Department of Human Resources, the university population includes four groups, namely, 10,328 undergraduate students, 10,467 graduate students, 7,631 staff and 2,012 professors. The number of students is updated annually with new enrollments. The study method and design were selected by one of the authors (L.V.V.) using a proportional stratified, probabilistic procedure applied to the four groups of university subjects. Using this approach, a representative ratio was calculated for each professional category for a sample of 455 subjects, of whom 151 (33.2%) were undergraduate students, 145 (31.9%) were graduate students, 126 (27.7%) were staff and 33 (7.3%) were professors. These professional categories will be referred to hereafter as functions. Measuring instrument TMD were diagnosed using an already tested and standardized screening questionnaire based on the one recommended by the American Academy of Orofacial Pain (AAOP)4. The questionnaire consisted of eight questions related to jaw pain, including the location of pain, precipitating factors, and temporal pattern of pain, and five questions related to jaw function, including TMJ noises, locking, and difficulty in opening. A validation of this questionnaire done in a university population prior to this study showed a sensitivity of 85.4% and a specificity of 80% for extracapsular disorders9. Environmental stress was diagnosed by using the Social Readjustment Rating Scale (SRRS) described by Holmes and Rahe10. Application of the TMD screening questionnaire and SRRS Since most of the university population spends the entire day on the campus, the subjects were recruited upon exiting the institutional cafeterias after lunch, between noon and 2 p.m. This recruiting point was chosen because the individuals had just used their masticatory apparatus, which made identification and confirmation of the symptoms easier. Two dentists specialized in TMD and orofacial pain questioned the potential subjects. Criteria for inclusion The subjects were initially approached and received an explanation of the purpose of the study, and then decided whether they wished to participate in the investigation. No verbal explanations were provided to subjects when answering the questions since the questionnaires was selfexplanatory. Individuals who were undergoing any type of orthopedic or orthodontic treatment were excluded from the sample. All of the data were tabulated using the program Excel (Microsoft®). The Kruskal-Wallis test was used for numerical variables and the chi-square test for categorical variables. Multiple Correspondence Analysis (MCA) was used to analyze the conjoint relationship among the variables. The level of significance used was 5%. Results Based on literature reports of the age group in which the highest frequency of TMD has been observed, the subjects were divided into three categories: 17-24 years old (n=168, 36.9%), 25-44 years old (n=227, 49.9%), and >45 years old (n=60, 13.2%). There was an equal distribution of the sexes among undergraduate and graduate students, whereas women were significantly (p<0.0001) more common among staff (66.7%) and men were more common among professors (81.8%) (table 1). The presence of TMD was determined by classifying the pain associated with difficulty in chewing or speaking or with tired maxillae as moderate or strong; pain in the head, neck and/or teeth was scored in a similar manner (table 2). The prevalence of TMD among women in the three age groups was significantly higher than in men of the same age group. Among men, there was a higher prevalence in younger subjects compared to older ones. Analysis of the SRRS showed that 22.1% of the women had a high level of stress compared with 12.0% of the men (table 3). The SRRS also showed that 90.9% of the individuals with TMD had a high level of stress (table 2), i.e. >300 points (table 4). Multiple correspondence analysis (MCA) revealed the following relationships: a) The highest level of stress (>300) was associated with the highest scores (III) in questions 3 (greater difficulty/maxillary pain), 5 (greater maxillary rigidity), 6 (a,b,c) (more pains in the head, neck and teeth), and 8 (alteration in the bite), and was more common in women (right quadrant of the graph, showing the staff and graduate students); Discussion The main finding of this study was an association between stress and the symptoms of TMD. The strong association seen between stress and pain-related symptoms compared to other symptoms may reflect the greater effect of stress, especially in myalgia11. These results agreed with clinical findings that associated facial pain and headache with stress. A living organism maintains a complex dynamic equilibrium or homeostasis that is constantly challenges by intrinsic or extrinsic factors. These stressors, psychological or physiologic, set into motion central and peripheral responses designed to preserve homeostasis12. The hypothalamicpituitary-adrenal (hpa) axis and the autonomic nervous system are the principal effectors of the generalized stress response and are crucial for maintaining basal and stressrelated homeostasis13. Deregulation of the HPA axis has been demonstrated in several psychiatric stress-related disorders, such as depression and post-traumatic stress disorder, which have a significant higher prevalence among patients with TMD14. Reviewed the studies of patients with TMD15 concluded that despite many contradictions, there were no significant differences between the sexes when changes and alterations in the morphology of the TMJ are considered. On the other hand, when the signs and symptoms of TMD are considered, and an incidence of 1.5-2 women for every man, and about 80% of the patients treated with complaints of TMD are women16. The severity of the symptoms was correlated with age, with a greater prevalence among 20-40-year-old women17. The results of this study show that the prevalence of extracapsular TMD among 25-44-year-old women is significantly higher than in men of the same age group. This age-dependent distribution of the pathology and the greater number of female subjects suggested a possible link between TMD and female hormones16. Bush, Harkins and Harrington18 attributed the larger prevalence of TMD in females the fact that women seek treatment or generally care better care of their health than men. Gender differences in HPA axis function have been demonstrated in animals and humans, and interactions are known to occur between the HPA axis and the hypothalamicpituitary-gonadal axis at multiple levels. The gender differences in HPA axis function make women more vulnerable to the pathologic sequelae of stress and may account for the female predominance in stress-related disorders19. Headaches are a common complaint among adults, but are subjective and are generally not life-threatening. Headaches associated with TMD result from pain originating from the masticatory muscles, TMJ, teeth or cervical areas18. In a study of the incidence of headache in TMD and non-TMD groups, Pettengill20 found that the TMD group had a greater severity of headaches than the non-TMD group, and that females in the TMD group had the highest values. Approximately 40% of chronic pain syndromes occur in the craniofacial region21, with the most prominent being craniomandibular dysfunctions and cephalalgias caused by muscular contraction. The latter observation suggests that head and neck muscles are particularly sensitive to psychological stress. Most (90.9%) of our patients with a high level of stress had moderate/strong symptoms of TMD. Anxiety and depression22 may be part of this phenomenon by acting as a predisposition and aggravant in cases of TMD. The association between neck pain and TMJ symptoms was shown by multivariate analysis, when higher levels of stress (³300) were associated with higher scores in the questions that quantified maxillary difficulty/pains, maxillary rigidity, pains in the head, neck and teeth, and alterations in the bite, and associated these effects with women. Among the subjects studied here, the subgroup with the strongest relationship between TMD and stress consisted of women 25-44 years old. This age interval included the majority of staff and graduate students. Gender, age and socioeconomic differences have provided insights into the risk factors for TMD, and have led to broader biopsychosocial investigations of the causes of this pathology. References
© Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06026t2.jpg] [os06026t1.jpg] [os06026t3.jpg] [os06026t4.jpg] [os06026g1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}