 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
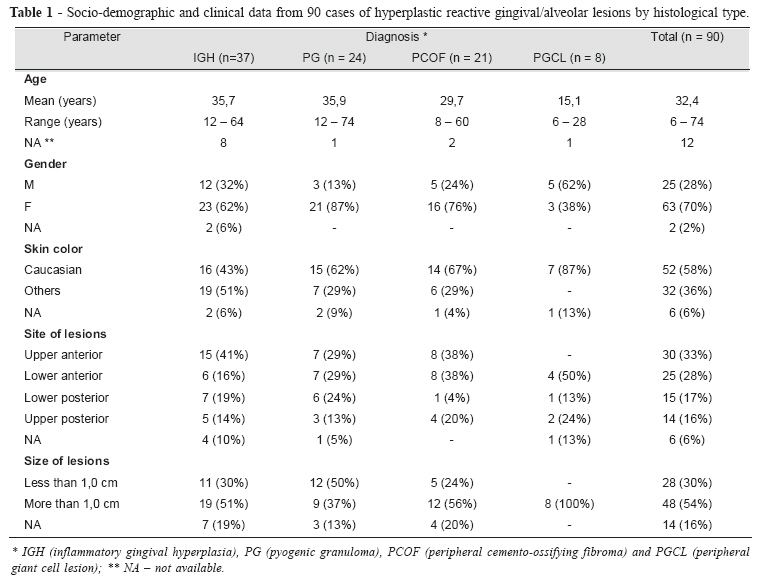
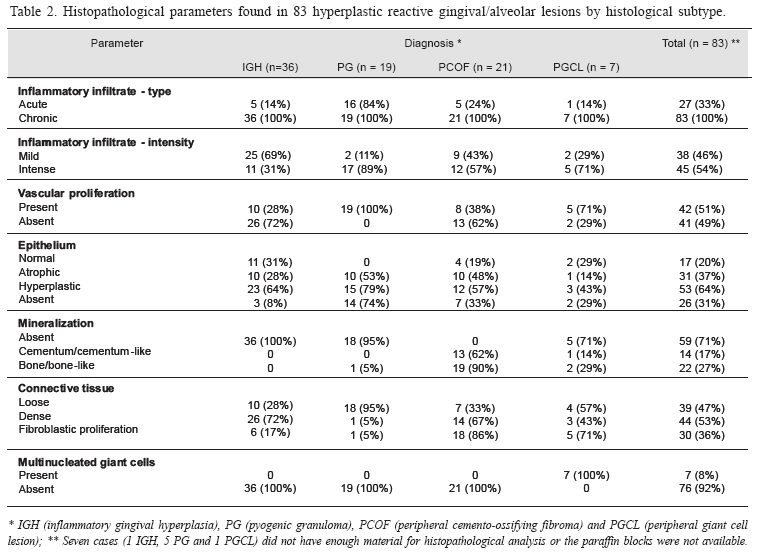
Brazilian Journal of Oral Sciences, Vol. 5, No. 18, July-September 2006, pp. 1085-1089 Gingival and alveolar hyperplasticreactive lesions: clinicopathologicalstudy of 90 cases Pryscilla Giglio Peralles 1 Ana Paula Borges Viana 1 André Luiz da Rocha Azevedo 2 Fábio Ramôa Pires3 1DDS; formerly undergraduating students; School of Dentistry, Estácio de Sá University Received for publication: June 28, 2006 Code Number: os06028 Abstract Hyperplastic reactive gingival/alveolar lesions are one of the most common subgroups of oral lesions, however few studies have focused their clinical and microscopic characteristics on our population. The aim of this study was to analyze the socio-demographic, clinical and microscopical features of 90 hyperplastic reactive gingival/alveolar lesions from an Oral Pathology Laboratory from Rio de Janeiro, Brazil. Inflammatory gingival hyperplasia (IGH) and pyogenic granuloma (PG) were the most common diagnosis in this group. Females on their 3rd to 4th decades of life were the predominant group affected and most cases affected the anterior portion of the oral cavity. Histopathology revealed that all cases were associated to chronic inflammatory infiltrate and vascular proliferation was prominent in PG. Epithelial alterations were also more common in PG, but mineralization showed marked affinity for peripheral cemento-ossifying fibroma (PCOF). Fibroblastic proliferation was more evident on PCOF and peripheral giant cell lesion (PGCL) and multinucleated giant cells were found exclusively on PGCL. Clinical and socio-demographic findings alone were not enough for distinguishing all lesions from this group, and our findings showed that few cases were suggestive of an evolutionary process. Key Words: gingiva, inflammatory gingival hyperplasia, pyogenic granuloma, peripheral cemento-ossifying fibroma, peripheral giant cell lesion Introduction Hyperplastic reactive lesions represent as a group the most common oral lesions, excluding caries, periodontal and periapical inflammatory disease. In this group, fibrous hyperplasia, associated or not to removable prosthetic appliances, represent the great majority of cases, and the second most common subgroup is represented by hyperplastic reactive gingival/alveolar lesions, including inflammatory gingival hyperplasia (IGH), pyogenic granuloma (PG), peripheral giant cell lesion (PGCL) and peripheral cemento-ossifying fibroma (PCOF)1-2. Although there are some clinical differences among the lesions in this subgroup, their etiology is essentially similar, and the presence of variable amounts of inflammatory infiltrate in all of them can determine high clinical and microscopic resemblance2-8. Etiology of these lesions includes local tissue irritation, specially represented by bacterial agents, cellular debris, calculus, foreign bodies, and orthodontic and prosthetic appliances1. Even with common etiologic factors, tissue response follows different courses in each individual lesion, reflected by their microscopical characteristics2-8. Diagnosis of each lesion from this subgroup is aided by their clinical and periapical radiographic features, but histopathology is the key for final diagnosis. Although constituting one of the most common groups of oral lesions, few papers focusing Brazilian patients have been published in the literature, making it difficult to understand their characteristics in our population comparing to others. The aim of this paper was to analyze the clinicopathological features of 90 cases diagnosed as hyperplastic reactive gingival/alveolar lesions from an Oral Pathology Laboratory. Material and Methods Ninety cases diagnosed as IGH, PG, PGCL and PCOF arising from gingival/alveolar oral tissues, selected from the files of the Oral Pathology Laboratory, School of Dentistry, Estácio de Sá University, from 1999 to 2005, were reviewed for the study. Socio-demographic and clinical information such as age, gender, skin color, type of biopsy, and site and size of the lesions, were obtained from the patients records. All cases were histopathologically reviewed on Hematoxilin and Eosin staining, and final diagnosis was grouped in one of the four previously described diagnosis. For final diagnosis, some microscopical parameters were analysed, including: Distribution of inflammatory infiltrate – classified as mild, when there were focal areas, specially on the sub-epithelial area, or intense, when it was disperse and deep on the connective tissue. Type of inflammatory infiltrate - predominantly acute, chronic or both. Presence of vascular proliferation – presence of abundant capillary or cavernous vascular proliferations on the connective tissue (not only focal areas of increased vascularity). Pattern of the oral mucosal lining epithelium – subdivided in normal, atrophic (thin epithelium with less than 5 cell layers), hyperplastic (epithelium with more than 15 to 20 cell layers) or absent (areas of ulceration). Presence of foreign body multinucleated giant cells Presence of mineralized material – microscopically compatible with bone and/or cementum. Type of connective tissue - loose or dense; as well as the presence of fibroblastic proliferation dispersed on the connective tissue. Final diagnosis was correlated to both socio-demographic (age, gender, skin color), clinical (type of biopsy, site and size of the lesions) and microscopical features. This study did not include direct examination of the patients and was based on laboratory registries review. Results From the 90 cases, there were 37 IGH (41%), 24 PG (27%), 21 PCOF (23%) and 8 PGCL (9%). Mean age of the patients was 32,4 years, varying from 6 to 74 years. PGCL (15,1 years) and PCOF (29,7 years) showed inferior mean age than IGH and PG, the latter being close to 36 years. Females represented 70% of the patients, and this predilection was more evident on PG (87%), not being observed in PGCL. Most patients (58%) were Caucasian. Site of the lesions showed that the anterior portion of the gingiva/alveolar mucosa was affected in 61% of the cases, varying from 50% to 66% on the different histological diagnosis, with discrete prevalence for the upper region. Most lesions (54%) were larger than 1,0 cm on diagnosis, except for PG (Table 1). Color, shape and evolution data were available only for 33, 21 and 40 cases, respectively. Almost 75% of the PG were erythematous, in contrast to 58% of the IGH and 36% of the PCOF. The base of the lesion was considered pediculated in all PG, in 70% of the IGH and in 43% of PCOF. Both IGH and PCOF showed 69% of the patients complaining of the presence of the lesions for more than 3 months, while 58% of PG patients reported the presence of the lesion for less than 3 months. We excluded PGCL from this analysis due to the limited number of cases with complete data. Histological parameters evaluated are described on Table 2. Inflammatory infiltrate was considered intense in 54% of the cases, specially on PG (89%) and PGCL (71%). Chronic inflammatory infiltrate was found in all cases and acute infiltrate was particularly common in PG. Vascular proliferation, specially capillary, was commonly present in PG and PGCL. Regarding epithelial morphology, atrophy, ulceration and hyperplasia were found predominantly on PG, although these findings were present in all other histological types. Mineralization showed marked affinity for PCOF, and bone/ bone-like areas were found in about 90% of them. Two cases of PGCL (29%) showed areas of bone formation, as well as one PG (5%). In this case, all other microscopical characteristics together allowed the diagnosis of PG, even with some mineralization foci on the lesion. Connective tissue was considered loose in most PG and, in contrast, was considered dense in most IGH and PCOF. Fibroblastic proliferation was present almost exclusively on PCOF and PGCL and foreign body multinucleated giant cells were found exclusively on PGCL. Hemossiderin was found in 6 cases, 4 PGCL (57%) and 2 PG (8%) (Table 2). Discussion Our results showed that IGH is the most common lesion from this group, followed by PG, in accordance with the literature1,46. Adults on their 3rd to 4th decades are the most affected patients, specially females, also in accordance with previous reports4-9. Most reports also show that the anterior regions of the oral cavity are affected more frequently, varying from 57% to 71% of the cases, and this can be explained by the fact that these regions are drier than the posterior regions, are prone to be affected by calculus deposition on the inferior region, and the frequent teeth malposition also in this area, difficulting hygiene and, consequently, plaque control4,5,7-9. Most PGs were smaller than other lesions, probably by the fact that they showed faster evolution and, as demonstrated by our results, commonly erythematous clinical appearance, reflecting the usual presence of bleeding, bringing local complaints and stimulating prompt evaluation by the patients6. Curiously, in contrast to our findings, Al-Khateeb and Ababneh8 reported that only 9.2% of their 108 PG showed superficial erosion or ulceration and Cuisia and Branon7 reported that more than half of their PCOF showed ulceration, clinically simulating PG. PG shows predilection for females, at least in part due to the fact that estrogen and progesterone levels influence vascular permeability, explaining the greater frequency of PG during pregnancy1,6,8-11. Our results reinforce this concept, as 87% of our PG was found in females and 2 cases (8%) affected pregnant females, however the literature has shown less prominent predilection for females, varying from 55% to 63%8,9. One PG showed small foci of mineralization, apart from the usual microscopic findings of PG. Some reports in the literature suggest a possible evolution and maturation of PG towards PCOF, with decreasing of the inflammatory component, increasing of the fibrous component, and development of some foci of calcification1. In this case in particular, the presence of small foci of calcification, can suggest this transition and, in addition to this possibility, we could identify the presence of vascular proliferation in 38% of our PCOF. In contrast to this possibility, we found that the mean age of the PCOF patients was lower than of PG patients, a finding previously reported in the literature7. Lawovin et al.9 and Al-Khateeb and Ababneh8 reported that about 33% and 25% of their PG, respectively, presented areas of fibrous scar, associated to discrete chronic inflammatory infiltrate. Other 3 cases from our study revealed microscopic findings intermediate from more than one diagnosis: one case presented findings from PCOF and PGCL; one case of PCOF showed areas of PG; and a case that microscopically resembled IGH showed areas of calcification, compatible with PCOF. Cuisia and Brannon7 reported that to their 127 PCOF, PG was considered the clinical diagnosis in 46% of the cases, in contrast to PCOF (9%). These findings reinforce the idea that some clinical and microscopical features can be shared by different diagnosis from this group, and that this supposed maturation process can eventually occur in some cases, but is not the rule in all PG. PCOF affects exclusively the gingival/alveolar tissues, with predilection for young adults, and its histopathology includes the presence of a fibrous colagenized connective tissue and variable amounts of fibroblastic proliferation, both permeated by an usually chronic inflammatory infiltrate1,4-5,7. Ulcerated lesions can represent up to 40% of the PCOF cases, being usually associated to proliferative connective tissue, and this variety of microscopic aspects inside the same entity can in fact also reflect the possibility of a spectrum of evolution also on PCOF4-5. The PGCL, also known as peripheral giant cel granuloma or reparative giant cell granuloma, similarly to PCOF, affects exclusively the gingival/alveolar mucosa, mainly from adult females, and seems to be influenced by hormonal stimulus, specially estrogen3,12-13. Microscopically it is characterized by extensive hemorrhagic areas and hemossiderin deposition, what gives to PGCL usually a somewhat blue-purplish color1-3. Mean age reported in the literature ranges from 40 to 60 years3, in contrast to our findings, but the small number of cases reported in our study difficults a direct comparison. The multinucleated giant cells on PGCL seem to originate their histogenesis from mononuclear phagocytic cells14, and were found exclusively on this lesion. Our findings showed that, in accordance with the literature, calcification foci can be found in PGCL, although they are much more frequent in PCOF2-5,15. Retrospective studies can pose limitations on getting clinical information, as they are based on available information on Laboratory records. In this group of lesions, data from the consistency and mobility of the lesions, presence of bleeding, teeth dislocation, and radiographic findings, are not always included on the laboratory charts, and for this reason were not included in our study. Treatment of all lesions from this group includes conservative surgical removal, associated to removal and control of causative factors. Clinical and socio-demographic findings alone are not enough for distinguishing all lesions from this group, and some authors have suggested that they can be an evolutive spectrum. Our findings sustained that they are probably different reactions to similar causative factors, and few cases are suggestive of an evolutionary process. Acknowledgements We thank the Department of Cientific Research and the School of Dentistry, Estácio de Sá University, for the support to this project. References
© Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06028t1.jpg] [os06028t2.jpg] |
| |||||||||

{kind=link}
{kind=link}