 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 5, No. 18, July-September 2006, pp. 1101-1108 Chewing performance and bite force in children Alexandre Durval Lemos1 Flávia Riqueto Gambareli2 Marcia Diaz Serra2 Rafael de Liz Pocztaruk3 Maria Beatriz Duarte Gavião2 1Department of Pediatric Dentistry, State University of Paraíba, João Pessoa, PB, BR Received for publication: June 23, 2006 Code Number: os06031 Abstract The aim was to correlate the chewing performance and maximum bite force in children, considering the morphologic characteristics of occlusion and body mass index (BMI). Thirty-six children participated (19 girls and 17 boys, mean age 9.06 years). The occlusal characteristics were evaluated by intra-oral examination. Body weight (kg) and height (m) were assessed using a balance with anthropometrical scale, and BMI determined (kg/m2). For chewing performance the children chewed a round silicone tablet (5 mm thick and 15 mm in diameter, 1.2 g ±0.005 g) with 20 strokes. The particle sizes were analyzed by a software. The bite force was determined with a pressurized rubber tube connected to a sensor element. There was no difference between genders in all variables. Bite force correlated negatively with particles sizes (p<0.001), meaning that high bite forces implicated in better chewing performance, and was weakly correlated with BMI (r=0.410, p<0.05). Children with different molar and canine relationship did not show differences among the variables. It was concluded that chewing performance depended on the maximum bite force, but other factors like the number and area of occlusal contacts, the amount of lateral excursion during mastication and dentition phase also may play a role. The occlusal characteristics did not influence the chewing measurements, whereas body size had a relationship with bite force. Key Words: mastication, muscle strength, mixed dentition, dental arch, children Introduction Several factors influence the chewing function. The breakdown path during mastication may be determined by the mechanical actions employed, for example muscle strength and dentition, as well physiological responses, for example, salivation1. The teeth are important in the masticatory system, as they form the occlusal area where the food particles are fragmented, depending on the total occlusal area and thus on the number of teeth2-3. Another important factor in chewing is the bite force, which depends on muscle volume, jaw muscle activity, and the coordination between the various chewing muscles3. Bite force increases with the need for chewing, but decreases with deteriorated dentition4-7. The strength of the jaw muscles determines the amount of available force to cut or crush the food8 and various methods have been used to evaluate clinically the physiologic characteristics of these muscles. One of them is the measurement of the voluntary maximum bite force9-13. As mastication results in reducing the size of food particles in preparation for swallowing and digestion, its performance can be measured by determining the individual capacity to comminute a test food, i.e., asking the subject to chew the food for a given number of chews and spit them out14-15. Some studies have been using chewable test materials other than natural foods for measuring objectively chewing performance, because the physical properties, shape and size of the particles are more reproducible4,8,16. Following the demonstration of its suitability17 the silicone impression material has become the material test choice to measure objectively the chewing performance7,18-20. The silicone samples fulfill all the criteria of a test material. Namely, this material is stable, accurate, reproducible, and has mechanical properties that are comparable to those of natural food substances17, despite it has not showed the same rheologic properties as the natural food substances, but its characteristics were sufficiently similar, suggesting this synthetic material as a reproducible alternative for the testing of masticatory efficiency21. The synthetic materials do not dissolve in water or saliva and are able to be broken down during mastication. They do not break along predetermined fault lines and have no taste. They are standardized and can be stored without loss of their properties. Therefore, they could not be used in studies of the entire process of mastication from incising to swallowing. Otherwise, the silicone samples may be masticated in exactly the same way as a natural food. Fractional sieving has been widely used to determine the degree of breakdown of the chewed particles4,7-8,15,18 as well as an optical system in which the projected dimensions of the comminuted particles were measured22-23. The accuracy and specificity of the optical system is accompanied by an increase in speed over the conventional method and it has value when interest is restricted to relatively large particles, like the first few strokes on hard foods23. Chewing performance and bite force can influence the development of masticatory function. Chewing is a developmental function and its maturation occurs from learning experiences. If mastication is adequate, it gives stimulus and proper function to normal development of maxilla and mandible18,22. Thus, it is important to determine these parameters during the periods of growth and development, as well as their relationship with morphologic characteristics of the dental arches, by getting comparative data in order to verify if the masticatory system is progressing properly. Thus, the aim of this study was to correlate chewing performance and maximum bite force in children, as well as to consider the characteristics of morphologic dental occlusion and body variables. The hypothesis tested was that the chewing performance and bite force would be correlated and depended on the morphological occlusion. Material and Methods Sample About one hundred children, aged 7-12 years, were randomly chosen from the files of our Pediatric Dentistry Clinic and thirty-six children, who agreed and were cooperate, were selected for the study. Those suffering from systemic health diseases, or who showed uncooperative behavior were excluded from the study, as well as those who had previously had any kind of orthodontic treatment. Written and verbal consent was obtained from each child’s parents/guardians prior to the investigation, after having been informed about the procedures, possible discomforts or risks. The Ethics Committee of our Dental School approved the research. The selected children were composed by 19 girls and 17 boys, mean age 9.06 years. The inclusion criteria were as follows: the children should be in mixed dentition, with the presence of first permanent molars and upper and lower central incisors in occlusion or in the initial phase of permanent dentition, i.e., the upper canines should just have erupted. All present teeth should have no anomalies of form, structure or number, or alterations that could compromise their dimensions and the normality of the oral tissues. Postcanine teeth should be present and in occlusion, irrespective of whether they were primary molars or pre-molars. Dental arch characteristics The intra-oral examination comprised the evaluation of the following occlusal characteristics in the clenching position: -first permanent molars relationship: in accordance with Angle’s classification that refers to the position of these teeth and how they bite together
-Upper and lower canines relationship:
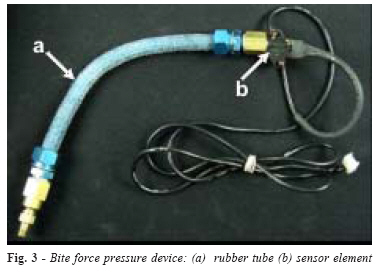
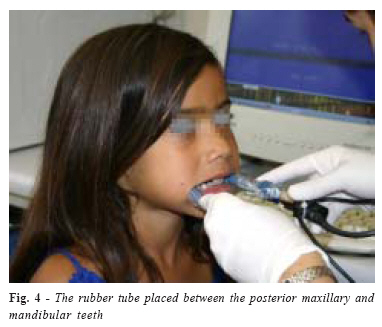
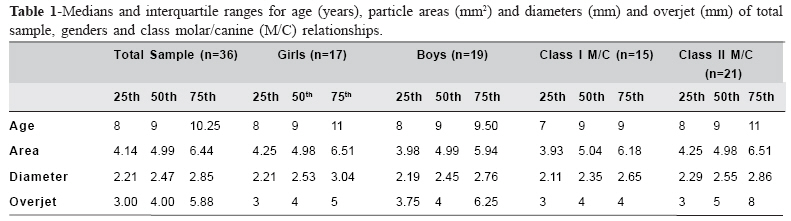
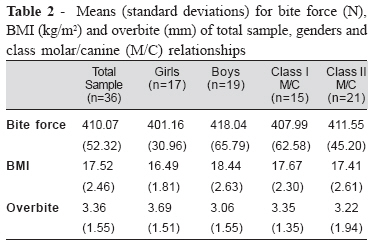
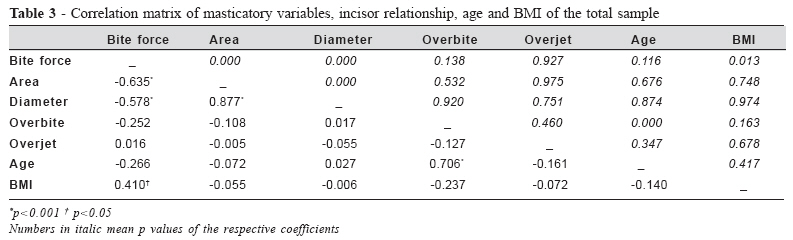
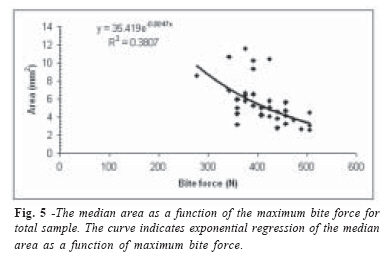
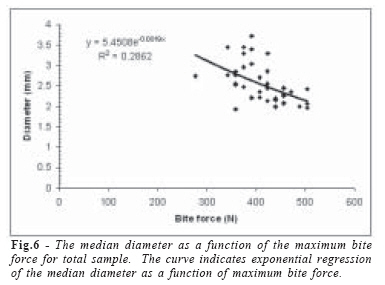
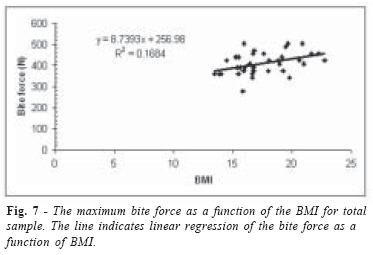
- Overbite: vertical overlap of upper over lower central incisor teeth (mm) -Overjet: horizontal projection of upper central incisor tooth beyond the lower central incisor tooth (mm) - Posterior crossbite: one or more teeth in the maxillary buccal segment is lingual to one or more of the opposing teeth in the mandibular buccal segment in maximum intercuspation The body weight (kg) and height (m) were measured, using a balance with an anthropometrical scale (Welmi, Santa Bárbara D’Oeste, São Paulao, BR), and the body mass index was determined, defined as weight in kilograms divided by height in squared meters. All exams were performed by a trained examiner (ADL). Chewing performance and bite force evaluation The chewing test material was a tablet (Fig. 1), 5 mm thick and 15 mm in diameter, of condensed silicone (Optosil®, Bayer, Leverkusen, Germany), which size and shape allowed comfortable conditions for performance of the test, considering the children’s age. The Optosil® material was manipulated in accordance to fabricant instructions, placed in a split mould (Fig. 2) and pressurized into the perforations between two thin glass plates protected with teflon foil, by hydraulic pressure using a press set at 50 kP/cm2. Each portion was weighed and if weight variation was observed the tablet was cut down by hand to a weight of 1.2g±0.005 g. The completed test portion then was rounded to a tablet formation. This meant that from the beginning of mastication the test portion would be broken in a uniform way. Children were trained before the experiment in relation to masticatory movements and mouth rinsing so that they would chew correctly, not swallow and be familiarized with the test material. All cooperated with the methods. They were instructed to chew one tablet for a total of 20 bilateral strokes, controlled by the examiner. The chewing was unrestricted and allowed to be performed uni – or bilaterally. Following, they spat the particles into a plastic recipient, covered with a filter paper. Next, the children rinsed their mouth with water and spat out the particles that remained in the mouth, repeating it until it was ascertained that there were no particles left behind. After that, the mouth was verified to check that no test material Particles remained. If any particle remained it was removed with a dental nipper. The chewed particles were washed with water, dried and then weighed in order to check the material loss. The test was repeated when there was any loss of material greater than 6%20. After dried, the particles in each filter were transferred onto a tray with a dark background and were spread out unconnectedly, to allow correct digital analysis of all the pieces. Each tray, with each child’s particles, was photographed using a 105 mm standardized-distance particle camera (Mavica® Digital camera, Sony Style, USA) sustained by a support. Flexible optical filament fountains provided the proper incident light. Images were analyzed by Image Lab software (Softium Informatica Ltda-ME, Fortaleza, Brazil). The mean particle sizes, area (mm2) and diameter (mm), of the chewed particles were used as values representative of chewing performance. A decrease in the measurements was considered to be enhanced performance. The bite force was determined with a pressurized rubber tube connected to a sensor element (MPX 5700 Motorola SPS, Austin, Texas, USA), both connected to a converse analog/ digital electronic circuit, fed by an analog sign coming from the pressure sensitive element (Fig. 3). The system was connected to the computer and a software for reading the pressure was developed. The tube was placed between the posterior maxillary and mandibular teeth (Fig. 4). The subject bit the tube with maximum force 3 times successively for 5 seconds, with a 10-second interval between each bite. The highest value was considered. The values from the pressurized tube were obtained in PSi and converted into Newtons taking in account the area of the tube, since force is equal pressure times area. The reliability of the bite force measurements was determined on 10 randomly selected children using the Dahlberg’s formula: EM= √ (x1- x2)2/2n on two repeated measurements (x1, x2) of 10 subjects’ data. The method error was 6.55% (16.28 N). Statistical Analysis The normality of the distributions was assessed by the parameters of skewness and kurtosis and by the Shapiro-Wilks W-test. Student’s t and the Mann-Whitney tests were used to compare values between genders and between different molar and canine relationships, when indicated. Associations between variables were assessed by the Spearman or Pearson rank order correlation. Adjusted different regression models to the data were applied to each correlation significant at the p < 0.05 level, in order to test which parameters were most important for the magnitude of bite force and chewing performance. To determine proportions among morphological characteristics of dental arches in the entire group the Chi-squared test was used. The test results were considered to be significant at p-values below 0.05, The SPSS 13.0 for Windows (Evaluation version, SPSS Inc, Chicago, IL, 2004) was used. Results The particle sizes, age and overjet measurements were not normally distributed. Thus, their central tendencies and dispersions were described with medians and interquartile ranges as shown in Table 1. Means and standard deviations of the bite force, BMI and overbite are shown in Table 2. There was significant negative correlation between bite force and particle sizes (Table 3). The regression analysis showed that the equations explain 29% to 38% of the variation in the particles due to the bite force (Figures 5 and 6). Bite force was also correlated with BMI. Nevertheless the determination coefficient was low, as approximately 17% of variability in bite force could be explained by the body variables. There was no difference between genders in all variables. Children with Class II molar and canine relationship presented significantly higher mean values for overjet compared with children with corresponding Class I, and they showed no differences in relation to other variables. Discussion As chewing performance is one measure of function14,24 and so a material with uniform properties that can be reliably reproduced would provide an ideal test bolus for the scientific study of masticatory effectiveness21. The silicone has been chosen as a test material predominantly in dentate subjects, taking into account the advantages, from a physical point of view, offered by a synthetic material17,21, providing constant physical characteristics, yet their non-edible nature unavoidably affects the natural pattern of jaw movement25. Furthermore, it is readily available and identical test portions can be produced under identical conditions all over the world17. Thus, in this study the Optosil® was chosen as the chewable test material in view of the above-mentioned considerations and because it had been a suitable material for the studied children, well accepted during the training before the actual test. The number of 20 cycles was standardized since it was an adequate number, as perceived during the trials, and did not lead to chewing fatigue. There were no significant differences between genders, thus the results were pooled. The difference in muscle strength observed between boys and girls during puberty6,26 may explain the similar results between boys and girls at earlier ages. The results demonstrated that bite force and particle sizes were negatively correlated (pd”0.0002) (Table 3). As enhanced chewing performance was considered to be dependent on the particle sizes, that is, smaller particles mean better performance, higher bite force determined better chewing performance, agreeing with Fontijn-Tekamp et al.4 and Okiyama et al.12. The regression analysis showed that 29% to 38% of the variability in chewing performance could be explained by the effects of bite force, as found by Fontijn-Tekamp et al.4, suggesting that other factors besides muscle efficiency and force generated during mastication are determinants of chewing performance12,16, for example, the number and area of occlusal contacts and the amount of lateral excursion during mastication27-29. The children of the current study had all their posterior teeth, irrespective of being deciduous molars or pre-molars. The number of post canine functional tooth units and the number of occluding pairs of teeth have been considered the best predictors of chewing performance2,5,7,29. On the other hand, Julien et al.8 and Shiere and Manly30 considered that during the time that the deciduous molars are shed and when their second molars reach the occlusal plane the children’s performance can be reduced. Therefore, masticatory performance should not be expected to improve at a constant rate in growing children, particularly during the change from the primary to the permanent dentition30. In addition, under a more normal condition, when the maximum bite force exceeded a certain value, it made no further contribution to a decrease in particle size, as reported previously4,19. It must also be considered that the jaw stretch reflex is maturing as the child continues to acquire new oral motor skills, as feeding31. The results showed that children with Class I molar/canine relationships did not have different particle size values in comparison with Class II relationships, agreeing with Toro et al.32. Contact areas determine the area available for comminuting the foods during masticatory movements, whereas wide chewing cycles with predominately lateral paths of closure are closely related to improve chewing performance8,29. Although it is believed that some malocclusions may limit the amount of lateral excursion, there are no studies documenting a consistent relationship between malocclusion and reduced lateral excursions during chewing18. On the other hand, individuals who had the largest wear facets on the occlusal surface also had the highest amount of occlusal contact8, the wear being a physiological occlusal condition in deciduous dentition. Although the contact areas were not quantified in this study, it is possible that the children’s deciduous teeth may have had greater contact areas due to the physiological wear, as most of them were in the mixed dentition. Since occlusal wear may eliminate interferences, a greater range of lateral excursion was allowed33-35 thus improving the chewing performance33. These considerations could be supported by the lack of correlations between particle sizes, overbite and overjet (Table 3). Therefore, the chewing performance could be more related to the contact areas than the bite force itself28. Conversely, the findings of English et al.18 showed relationships between objective and subjective measures of masticatory performance with malocclusion, but malocclusion has no effect on the number of chews required to swallow jerky and almonds, affecting an individual’s perception of how well they can chew. Our results are distinct from these authors in relation to capacity of our children with different types of malocclusions break the chewable test material, but their age sample ranged form 7 to 37 years. As considered by them, comparisons of median particle size among studies are confounded by the use different methodologies18. Maximum bite force was also not statistically different between the two types of molar/canine relationships, agreeing with Sonnesen and Bakke36, who found that the number of teeth present was the most significant factor for the magnitude of bite force in children aged 7-13-years. On the other hand, maximum bite force was weakly correlated with normal occlusion in accordance with Kamegai et al.10 in a very wide age range (3 to 17 years). In spite of the differences in sample characteristics, the variations in the maximal bite forces among studies have been shown to be associated with instrumentation design and transducer position related to dental arch36-37. Moreover, many physiological factors, like size, composition and mechanical advantage of jawclosing muscles, sensitivity of the teeth, muscle and temporomandibular joints can influence maximum bite force generation36,38-39. Thus, the subjects’ sensory feedback may limit willingness to exert the maximum effort6. BMI presented positive weak correlation with bite force, as demonstrated in Table 3. Taking in account the determination coefficient (Figure 7), BMI explained only 17% of variability in maximum bite force. Thus, it is believed that in the age group of the present study, bite force evidently depends on more complex factors than body size11,38-39 such as the crosssectional area of masticatory muscles and jaw biomechanics40. No correlation between particle sizes and BMI was observed. Nevertheless, several authors have found positive correlations between bite force, chewing performance and body height and weight8,41. Julien et al.8 found that heavier individuals broke down the particles into smaller sizes, and concluded that body weight and the contact areas of the teeth were significantly correlated with median particle size. On the other hand, despite the age range of the selected sample, all children had their upper and lower permanent first molar occluding, as considered in the inclusion criteria, showing that age changes in chewing performance are related to dental maturation, as considered by Toro et al.32, who verified an improvement in performance after the eruption of the first permanent molars, but a smaller difference between 9- and 12-year-old children, that may be related to the transitional nature of the mixed dentition. Considering the small influence of BMI on bite force found in this study, it could be inferred that the correlations between chewing functions and body variables could be stronger later on, when children are older, with increasing muscle mass during growth, influenced by androgenic steroids6,11,26. From the results, it was observed that the chewing performance may be dependent on the maximum bite force, but other factors besides muscle efficiency and force generated during mastication must be related. For Hiiemae et al.42 and Okyama et al.12 these two functions can influence dietary selection, which is closely related to quality of life43. The progressive dentition deterioration in adults was related to decreasing intake of calories, protein, carbohydrates, fiber, and numerous vitamins and minerals44-45 inferring that lower chewing performance might also be related to decreasing intake of nutrients18. In view of that, it might well be a more significant problem in young and growing children than it is in aging adults. Thus, the properly preventive and restorative dental measures, when indicated, might benefit the children’s general and oral health, as considered on the correction of malocclusion by Owens et al.28. Thus, as stated by Lucas et al.14, the state of the mouth might affect mastication and swallowing. Although malocclusion did not influence the chewing performance and bite force in the studied sample, it is important to diagnose it carefully and to decide when and how to treat the condition, in order to assure the proper development. Moreover, further studies should be undertaken, relating other influencing factors, such as craniofacial morphology, signs and symptoms of temporomandibular dysfunction and mandibular movements. In addition, the known fluctuation of functional variables in growing individuals in a time dependent context must be addressed by carrying out repeated measurements in order to verify the respective influences on masticatory system development. Acknowledgements We are grateful to CAPES and FAEP/UNICAMP that supported this research. References
© Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06031f2.jpg] [os06031t2.jpg] [os06031f3.jpg] [os06031f6.jpg] [os06031t1.jpg] [os06031f1.jpg] [os06031t3.jpg] [os06031f4.jpg] [os06031f7.jpg] [os06031f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}