 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
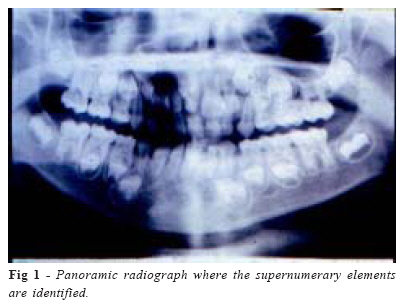
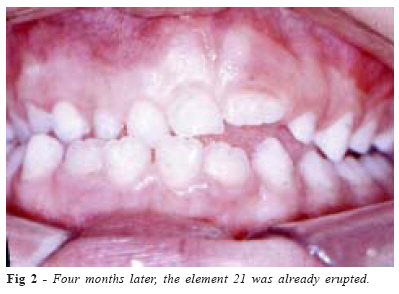
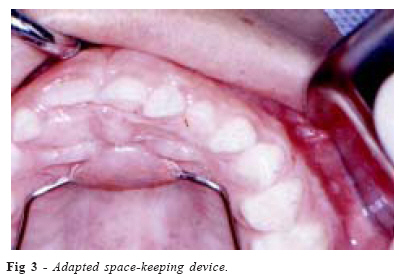
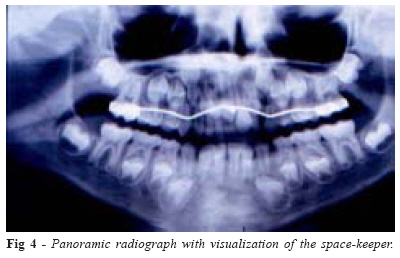
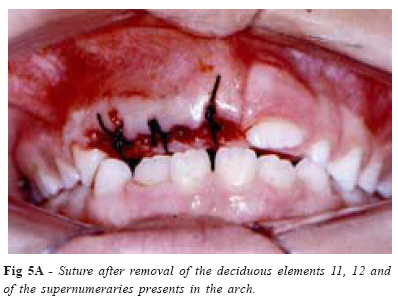
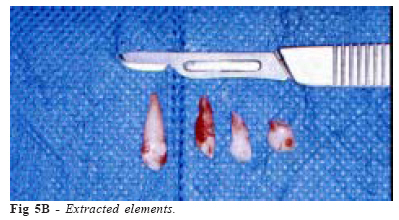
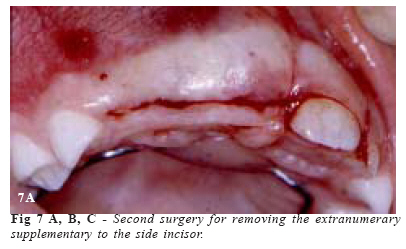
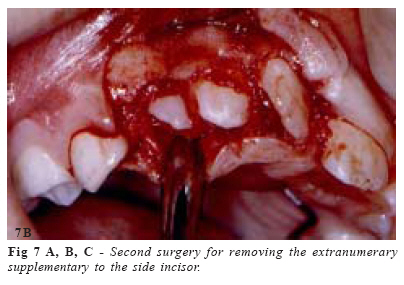
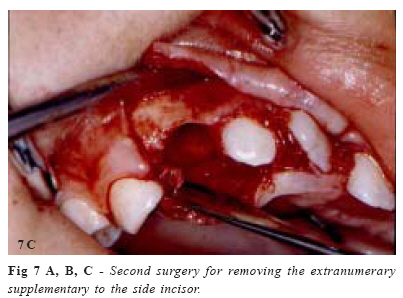
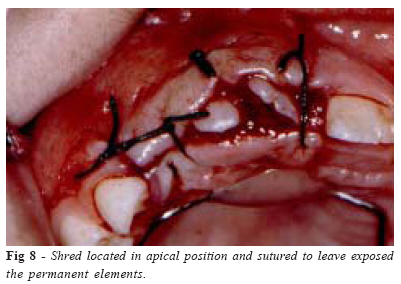
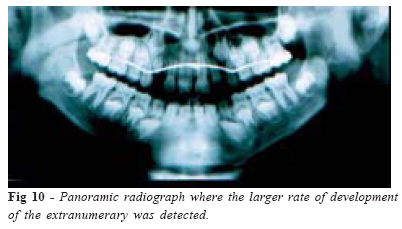
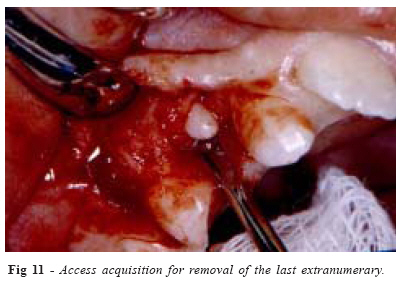
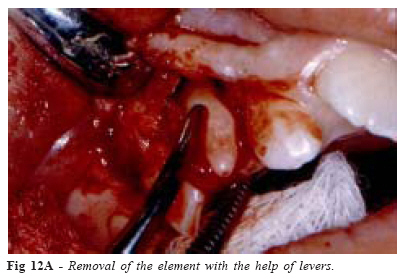
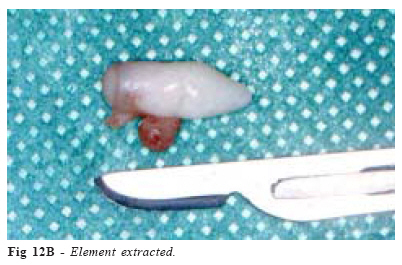
Brazilian Journal of Oral Sciences, Vol. 5, No. 18, July-September 2006, pp. 1112-1118 Supernumerary teeth at primary and permanent dentition Henrique Duque de Miranda Chaves Netto1* Neuza Maria de Souza Picorelli Assis1* Breno Nogueira1* Maria das Graças Afonso Miranda Chaves2* Robert Willer Farinazo Vitral3* 1 Oral and maxillofacial surgery Received for publication: April 03, 2006 Accepted: June 05, 2006 Code Number: os06033 Abstract Development disturbance originate in the odonthogenesis and begin around the 40TH week. It might occur on both dentitions, being scarcer in the primary one. Several hypotheses are mentioned for etiology of the supernumerary teeth and, among them, that one about hyperactivity of the Dental Blade, what would cause increment in the quantity of dental elements. There are correlations among the alteration in the quantity of teeth and systemic diseases, several syndromes as: Cleidocranian Displasia, Gardner Syndrome and Labial and Palatal Fissures. The clinical case of a male patient, 8 years old, leukoderm, which upper deciduous central incisors never exfoliated. The clinical examination demonstrated the presence of two erupted deciduous supernumerary elements between the elements 52 and 53. The radiographic tests (orthopantomography and per apical R-X of the incisors region) indicated the presence of further two impacted permanent supernumerary elements in the pre-maxilla region. The treatment plan selected was therapy for space maintenance in the arch with surgical removal of the supernumerary elements and orthodontic motion. Multidisciplinary approach provided adequate diagnosis and treatment to the patient. Key Words: odonthogenesis, radiography, primary dentition, permanent dentition, supernumerary Introduction Development disturbance originate in the Odonthogenesis and begin around the 40th week1. Supernumerary teeth are those found beyond the normal quantity for human dentitions2. Its etiology is controversial, thence several hypotheses are considered, like the Theory of Atavism, that suggests that the supernumerary would be an attempt for involution to ancestors3 and the Theory of Dichotomy, in which a dental germ suffers mitosis, generating similar teeth4. Authors like Borsato et al.5, associated excess of teeth to genetic factors, besides traumas occurred mainly in the period of development of the dental follicle, leading it to division and favoring the development. Almeida et al.6 stated that the most accepted hypothesis is that one about hyperactivity of the dental blade, what would provoke the appearance of supernumerary teeth. Likewise, there are correlations among supernumerary elements, systemic diseases and development disturbance as: cleidocranian displasia, Gardner syndrome and labial and palatal fissures. There are several ways to classify this anomaly, like: a) by location: classified as mesiodens when situated between the upper central incisors, distal molars (distally to third molars) and paramolars (located in the molars region); b) by shape: they might appear conic (small, cuneiforms and normally developed root), tubercular (multicuspidal, small with rudimentary root), supplementary (identical to the serial teeth) and odontomas (without regular shape); c) by position: being erupted or not in the dental arch)7-9. The supernumeraries might assault both dentitions, though they are scarcer in the primary dentition, with no distinction between sexes, whereas in the permanent dentition a greater incidence occurs in the masculine sex. Male patients are about two times more affected relatively to female patients2,7,10 and the relation jaw-maxilla is about 1 to 8, according to Stafne and Gibilisco, 1982 apud Torriani et al.2 2002. Their location varies, but it shows a predisposition for the upper fore region or pre-maxilla (approximately 90% of cases) and it does not present different incidences between left and right sides2. They might be impacted or erupted in the dental arch or in ectopic regions as the nasal sinus or the maxillary, the mesiodens being the most frequent, followed by the upper paramolars, lower premolars and side incisors with lesser frequency6. Their incidence is about 3% in permanent dentition11, increasing in individuals with embryologic disturbance as Gardner syndrom (approximately 21,2%) and labial palatal fissure (approximately 28%), according to Rajab and Hamdam12. In the primary dentition, the prevalence of supernumeraries is lesser than in the permanent one, with a percentage about 0,3 to 0,8%12-13. Torrioni et al.2 affirmed that the existence of a supernumerary element in the primary dentition increases significantly the probability of developing a supernumerary that will succeed it. The supernumeraries appear isolated (greater occurrence), in pairs or multiples, these being rare and usually associated to embryologic disturbance12. A study upon characteristics of the supernumerary teeth made by Borsatto et al.5 demonstrated a 62% incidence for a single supernumerary, 36% for two and only 2% for three. The diagnosis is made by clinical examination, observing the asynchronism in eruption regarding to right and left sides or to preëstablished chronology2, but mainly by radiographic examination, since the supernumerary eruptive potential is about 20%14. Though it might remain in its position for years, without pathologic manifestation, the supernumeraries might bring on several problems as retardation or impediment of succeeding teeth eruption, rotation or displacement of teeth in the dental arch, appearance of lesions like cyst, bone destruction, adjacent teeth rhizolysis, development of diastemes and occlusive disturbance, disruption and disturbance in the development of the permanent dental element and periodontal disorders12-13. The treatment of this kind of anomaly is related to removal or not of the element, being controversial as for epoch and necessity, forasmuch there are cases in which the supernumerary erupt and exfoliate naturally, mainly those related to the deciduous dentition2. The choice of therapeutics varies according to the position of the element and the presence or not of pathologic processes10. When a supernumerary is impeding the eruption of a permanent tooth and supernumerary element; removing the deciduous tooth and the supernumerary element; removing the deciduous, supernumerary, leaving the permanent exposed or removing both and using orthodontic apparatus for traction15. In about 75% of the cases, impacted teeth make eruption spontaneously after a period of 16-36 months post-extraction of the supernumeraries16. Patchett et al.17 states that the time enough for this eruption depends on two factors: rate of impaction and available space for spontaneous motion. Moraes et al.18 correlated the late removal to the impaction and necessity of pulling the permanent elements. One must also observe the apices of the neighboring dental elements in order to avoid the vessel-nervous sheaf to be disrupted. Some authors correlated the supernumerary extraction with lesions in the permanent teeth germs and the dental papillae of the neighboring teeth2. Clinical Case Male patient, 8 years old, leukoderm, headed towards the College of Dentistry from Juiz de Fora Federal University (UFJF) accompanied by a responsible person, advised by his odontopediatrist. His complaint was that his deciduous teeth had not yet exfoliated (upper central incisors). The clinical examination displayed the presence of two supplementary deciduous supernumerary elements erupted in the arch, between the elements 52 and 53. The radiographic examination (orthopantomography and per apical X-R from the incisors region) detected the presence of further two impacted permanent supernumerary elements in the premaxilla region. The right upper permanent central incisor was turnover (Fig 1). The patient was guided to the Clinic of Orthodontics for appraisal. The decision was to accompany in order to permit a possible exfoliation of the deciduous elements, expecting for a better moment for operation. The patient returned six months later and the presence of the element 21 in eruption was detected (Fig. 2). The other deciduous elements did not present mobility. The selected treatment plan was therapy for space maintenance in the arch with surgical removal of supernumerary elements for posterior orthodontic motion. As an initial orthodontic therapy, orthodontic bands were adapted to the first permanent molars and a space-keeping device type lingual bar with Nance’s button was prepared (Fig. 3 and 4). The first surgery was achieved to remove the deciduous elements 51 and 52, besides the supernumeraries present in the arch. With a bistoury blade number 15, an intra-groove incision was made from the distal of element 21 until the medial of element 53. The elements were extracted with the help of a forceps. After inspection and irrigation of the area with 0,9% physiologic serum, a suture with 3-0 silk thread was made (Fig. 5A and 5B). The patient returned for post-operative appraisal and suture removal. After four months, the patient returned for evaluation. The permanent teeth had not yet erupted (Fig. 6A). Then, a second surgery was achieved in order to remove the supernumerary supplementary to the side incisor. Concerning to the supernumerary in the region of the element 13, the option was to maintain it, since it was located close to the radicular apex of the element 53 and to the premolar teeth in development (Fig. 6B). With a bistoury blade number 15, an incision was made on the alveolar crest of the element 21 medial to the element 53 medial, with relaxing incision in the medial of the latter. The shred was doubled over to give access to the region. After the access, the element was removed with the help of levers (Fig. 7 A, B, C). The shred was replaced and sutured in a more apical position, with 3-0 silk thread, leaving the permanent elements exposed to facilitate their eruption (Fig. 8). There were no relevant alterations in the post-operative period. The patient was kept in periodic observation to appraise the eruption of the permanent elements that were exposed. Eight months after the second intervention, the patient presented the element 22 erupted and the elements 11 and 12 in the arch. The element presented spontaneous improvement in its position in the arch (Fig. 9). The radiographic examination (orthopantomography) showed the supernumerary element was in a more advanced stage of formation and in a more coronal position; therefore, its removal would not jeopardize the integrity of the other elements. Spontaneous improvement in the turnover of the element 11 was detected (Fig.10). The patient underwent a third surgery in order to remove the last present supernumerary element. As a more accurate method of radiographic detection, the Clark’s technique was used to determine position in the vestibularpalatine direction. The element under discussion was located vestibularly in relation to the teeth in the arch. With a bistoury blade number 15, an intra-groove incision was made from the element 21 medial to the element 53 distal, with relaxing incision in the distal of the latter. The mucus periosteum shred was severed for visualization and access to the operative field (Fig. 11). The element was removed with the help of levers (Fig. 12A and B). The irrigation was made with physiological solution at 0,9%. The sutured shred was set with 3-0 silk thread. The patient returned for suture removal and post-operative appraisal. The patient returned for suture removal and post-operative appraisal. The patient is still under attendance from the discipline of Orthodontics for future orthodontic motion and dental alignment, if necessary. Discussion Among the several ways to classify the supernumerary elements, we have the classification according to the shape. They might appear conic, tubercular, supplementary and odontomas. In the present case, supernumeraries supplementary to elements of primary dentition (52 and 53) and permanent (12) were under observation. Arcuri et al.10 stated that this anomaly might assault both dentitions, with preference for the fore region in the maxilla. The prevalence of supernumeraries in the primary dentition is around 0,3 to 0,8%, and 3% in the permanent dentition11-13. In this case, the presence of supernumeraries in the primary dentition was observed, what consists in a scarcer occurrence, and in the fore region of the maxilla, what is a more frequent find. The presence of supernumeraries supplementary to the side incisor and to the canine in both the dentitions, being according to Torrioni et al.2, who stated that the existence of a supernumerary element in the primary dentition increases significantly the probability of developing a succeeding supernumerary. Diagnosis is accomplished by means of clinical and radiographic examination and the eruptive asynchronism of the elements is one of the most frequent signals14. The initial diagnosis was eminently clinical, so the patient was guided to this institution with complaint of late eruption and the radiographic tests were achieved. The epoch and the need of teeth removal are controversial, as long as there are some cases in which the supernumeraries erupt and exfoliate naturally, mainly those related to the primary dentition. The loss of space in the arch after extraction must be considered, evaluating the need of therapy for its maintenance2. In the present report, the deciduous and supernumerary elements present in the arch were preserved during six months. At the end of this period, they had not yet exfoliated. So, the elements 51, 52 and the supernumeraries in the arch were removed. Orthodontic therapy was applied (space-keeper type lingual bar with Nance’s button), prevent in this way the medialization of the first upper permanent molars. In 75% of the cases, impacted teeth erupt spontaneously after a period of 16-36 months after extraction of the supernumeraries16 and this eruption depends on the rate of impaction and available space for spontaneous motion17. Since there was no detection of eruption of permanent elements, the choice was making the second surgery. The element position and the presence of pathologic processes influence the choice of therapeutics10. In addition, it must be observed the apices of the neighboring dental elements in order to avoid disruption of the vessel-nervous sheaf. Some authors correlate the extraction of a supernumerary with lesions in the permanent teeth germs and the dental papillae of the neighboring teeth2. In the second operation, only the element supplementary to the side incisor was removed, since the other impacted element was close to the tooth 53 apex and to the germ of the elements 13 and 14, without apparent lesion. In the appraisal made eight months the second operation, the remaining supernumerary element was still impacted. Its position did not jeopardize the adjacent elements, so its removal was achieved. The treatment applied in this anomaly is due to change from one case to another. It is important to evaluate the position of the element, the possibility of eruption and the risk to the adjacent structures, taking in consideration the risks and benefits of the surgery. The approach to patients with supernumerary teeth must be multidisciplinary. It is important the appraisal of the risks and benefits that the institution of a certain treatment must bring on. A more conservative therapy might bring many risks to the adjacent permanent teeth. It is possible to choose the serial removal of the supernumeraries, but it must be emphasized the constant accompaniment of the patient, as well as the space maintenance, so that the permanent teeth will be able to erupt. References
© Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06033f12b.jpg] [os06033f2.jpg] [os06033f6a.jpg] [os06033f7a.jpg] [os06033f7b.jpg] [os06033f11.jpg] [os06033f12a.jpg] [os06033f3.jpg] [os06033f5b.jpg] [os06033f4.jpg] [os06033f1.jpg] [os06033f6b.jpg] [os06033f9.jpg] [os06033f5a.jpg] [os06033f10.jpg] [os06033f7c.jpg] [os06033f8.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}