 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 5, No. 19, October-December 2006, pp. 1198-1202 Forensic tanatology: biological and legal aspects Arsenio Sales-Peres¹* , Ricardo Henrique Alves da Silva²** , César Lopes-Júnior³* ,Suzana Papile Maciel Carvalho4* ¹DDS, MSc, PhD Received for publication: February 10, 2006 Code Number: os06035 Abstract The forensic tanatology is a term which remits to a Greek origin: thanatos meaning death and logy meaning study. This way the discussed subject is wide however it refers only to human death. The purpose of this work is through a literature review give an actualization dates to law professionals, as well as to those who work in peritial activity in Medicine and Dentistry, searching to approach questions referred to death diagnostic and its certification, its law aspects and details referred to peritial tests in Tanatology. Key Words: forensic dentistry, tanatology, peritial, law science Introduction Tanatology (from Greek thanatos, death and logy, science) is the part of Legal Medicine that deals with death, phenomenon, and laws related to it. However, the concept of death seems difficult to be defined over the time and is always associated to the exclusion of some vital phenomenon1. According to the Committee for Definition of Death, of Christian inspiration (Work Group of the Pontific Academy of Science, reunited in the Vatican in 1989), a person is dead when she/he has been through a terrible and total loss of the capacity of integrating and coordinating all the functions - physical and mental - of the body in a functional unity2. The great difficulty is to define the exact moment the death occurred, which is extremely important for the family, experts in transplants, society and to the state. The idea that the body can only be in two states; life and death is wrong, since death is a slow and increasing process, with successive stages in a certain space of time and not only a moment. The death of the whole does not follow the death of the parts. Therefore, they necrose in increasing order of time: the nervous cells, epitheliums glandular, endothelium, myocardium, skeletal muscles, skin, spermatozoids, and epitheliums ciliates e leucocytes. This is what allows the use of these organs in transplants³. Thus, the death's definition accepted by the law is total and irreversible cease of vital functions, which do not disappear at once. Moreover, the study and acknowledgement of Forensic Tanatology are extremely important in Dentistry, since it is one of competences of the specialist in Legal Dentistry3, as well as to Medicine and Law, closely related to the theme of this study. The purpose of this work is, by a literature review, to provide an actualization to law professionals, as well as to those who work in peritial activity in Medicine and Dentistry, searching to approach questions referred to death diagnostic and its certification, law aspects and details referred to peritial tests in Forensic Tanatology. Death Diagnoses It is up to the doctor to certify the irreversible cease of the encephalic activity. As requested by the Commission for Organs Transplant, the subject of Neurology of the Medical School of University of São Paulo established official criteria for encephalic death according to the Legal Prosecution and the Commission for Regulamentation and Ethic Rules4. This criteria was approved by the Deliberative Council of University of Sâo Paulo Clinical Hospital, in a meeting in July 12 of 1983 when the following requirements to the diagnosis of encephalic death were established: subject under artificial breather and in deep coma, absence of primary hypothermia, of actual effects of paralyzing drugs, anesthetics, central nervous system depressors, hydroelectrolytical disturbances (hypo and hypernatremia), metabolic disorders, hemodynamic alterations (hypovolemia or shock), hypoxia and, cause of coma known and demonstrated4. Several actions can be done to prove this diagnosis, such as: electroencephalogram, brain arteriography or blood flow measures with the use of radioisotopes³. Resolution CFM n°1480/97 states rules to diagnosis of encephalic death to determine the moment of death and provide some aid to take organs, tissues and parts out of the body for transplants. The 2nd article requires a Declaration Term of Encephalic Death5. CFM n°27/90 states that when a patient suffers encephalic death, therefore considered dead, the doctor responsible for the patient must inform the family before the interruption of the artificial ways of maintaining vegetative functions, so that they have time to contest diagnosis. This practice has not yet become part of the people's culture, so the family may request another professional to provide diagnosis. This would be the moment to discuss the possibility of organs donation to transplant6. Medical Death Certification There are two kinds of coma resulting in death: structural and non-structural coma. In structural coma, diagnosis is relatively easy and reliable for it presents macroscopic alterations of the encephalon, such as: post-traumatic, vascular, or post-neurosurgical injury. Two clinical exams with a 12 hour-break must be performed³. In non-structural coma, unbalance and intoxication must be waited to disappear. Two clinical examinations with a 24-hour difference followed by um electroencephalogram isoelectric and eventually, other sophisticated exams such as angiographies can be used³. Encephalic or neurological death is characterized by the total and definitive abolition of the encephalon activity. The death of the cells of the central nervous system allows only one vital function to last, which is the heart, once the heart has an independent control system7. Classification of the kinds of death 1. The cause The most frequent cause of death is the natural, from morbid phenomenon, consequence of diseases evolution. On the other hand, the least frequent are violent deaths, resulting from the action of a hurting instrument of traumatic nature¹. Legally this kind of death can be classified as resulting from a homicide, accident, or suicide. Suspicious death does not show any evidence of violence; however it does not seem to be natural, including sudden or unpredictable death of an apparently healthy individual. Terminology may be used in two different ways: pathologic death, which the body belongs to the family, and legal death, which the body belongs to the State. A summary police investigation with necropsy proceeded of information collection, familiar anamneses, clothing and document examination is required. At the necroscopic examination the state of the clothes as well as hair traces, spots from liquids and human secretions (blood, saliva, sperm), minimum bodily injuries, (bruises on the neck, nose and mouth, petequial eyelid or subconjunctival, lesions on genitals), toxicological exams, microscopic evaluations, research on vital reactions and so on¹. 2. About reality Not so long ago one of the questions was to determine if the person was really dead or in an apparently death state, because despite the great number of signs which allow us that a person is dead, there are cases of return to life when it seemed impossible². Aiming to avoid precipitate burial which would be fatal in case of apparent death, the law establishes from at lest 24 to 36 hours, unless it ids for special reasons, burial8. In case of apparent death the vital functions are supposedly out due to depressors diseases of the central nervous system, body temperature may slightly fall and cardio-respiratory functions are lowered ending up in Thoinot's Triad, that is, immobility, absence of blood circulation, absence of apparent breath, which can last from some minutes until days9. Tanatologic examination It consists of the examination of the corpse and verification of the circumstances involving death. To find the cause of death the medical and legal aspects are considered. The tanatologic examinations that can be performed are:
According to Diniz7 (2001), it is sensible to accept the Theory of total encephalic death, that is, death only occurs with the death of the encephalic trunk, where the superior nervous centers that support respiratory and blood circulation. It is characterized by the absence of encephalic activity proved through laboratory exams, such as: encephalogram, carotid-angiography echo doppler or brain mapping, and all the present clinical and complementary criteria required by the Resolution nº 1.480/975. The Resolution n°1.480/975 of the Federal Council of Medicine states that the total and irreversible cease of the encephalic functions corresponds to death. The following criterions were observed:
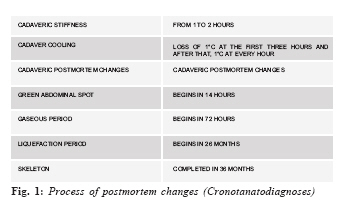
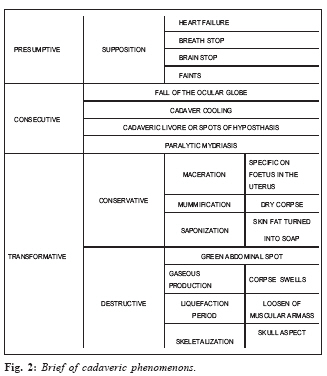
Cadaveric phenomenons Abiotic Phenomenon Immediate abiotic phenomenons happen after apparent death, that is, loss of consciousness, insensitivity, and immobility, abolition of muscular tonus, breathe and blood circulation suppression. Immediate abiotic phenomenon consists of: weight loss, skin parchment, mucous dissection, ocular globe flattening, body cooling, hypostasis and cadaveric stiffness. It begins with dehydration and reaches the maximum of 5 to 8 hours, remaining for 2 to 3 days, as consequence of the decrease in pH4. Hypostasis occurs due to blood circulation cease and blood suffers the action of gravity, staying internally in the viscera with much blood turning the skin pale. The destructive phenomenons occur simultaneously, autolysis, that is, cellular self-destruction due to the acidification of the middle and decomposing, which the first evidence is the green abdominal spot resulting from the reaction of hydrogen and hemoglobin. This reaction forms the sulfmethemoglobin that appears 16 to 20 hours after death and remains for about 7 days, followed by the gas period, with intense and unbearable smell, swelling of the cavities, lasting from 1 to 3 weeks4,7. The larva and insects participate in the process of the corpse disintegration, in the period of the liquefaction of tissues and skeleton at the end, which can take months or years4,7. Contrarily to destructive processes, there are the ones that maintain the corpse such as mummification, provoked (embalm) or spontaneous when the conditions of the environment collaborate to it. The skin of the corpse is stiff, with the appearance of dry leather, dark gray, more common in arid regions. Saponization occurs in locations with water and mud. The tissues are turned into adipocerous (dark yellow substance), with the smell of rancid cheese. Men chronotanatognosis studies can determine the time between death and necropsy. The modifications and phenomenons that are installed in the corpse are observed by chronotanatognotic techniques. Complementary exams are performed in the corpse in order to date with relative precision in a time range, the time of death (Figure 2). Requirements on the Tanatologic Exams According to Silva4 (1997), the requirements to be observed in the tanatologic exams are:
According to França9 (2004) legal medical necropsy determines violent death or suspicious death and provides through description, discussion and conclusion aids for certain facts to be taken into consideration, such as: legal cause of death, estimated time of death, identification of the dead subject and so on. Legal aspects of death The change from cardio-respiratory criterion to encephalic provided a great advance in transplantations since it allowed organs capitation. Article 6 of the Brazilian Civil Code states that the existence of the physical person ends with death. Rodrigues-Filho13 (2001) affirms that the Federal Council of Medicine does not have the power to rule death through simple resolution. For the legal concept, a person who has her/his respiratory and circulatory functions working, even if forced, is not dead, despite the failure of the brain activity. Legally, the failure of the brain activity leads to incapacity not death. Thus, a great legal discussion is begun; shocking Medicine, especially transplant groups and, Law. According to Venosa14 (2003), death is proved by the certificate extracted at the assent of death and the moment it happens is extremely importance. Nowadays death is diagnosed by the cease of brain, circulatory and respiratory activity. Rizzardo15 (2005) quotes Rita Maria Paulina dos Santos, who states that death phenomenon can be explained as: "Firstly the cell dies, after the tissue and following, the organs; it is a cascade phenomenon. Once this process is established, it can reach the organs on which life depends, called vital organs. Thus, breathe, circulation and brain cease their activity"15. Concerning the Obit Declaration by the doctor, there are circumstances leading her/him to decide to take the corpse to the Legal-medical Institute, as in violent deaths or in cases with violence suspect³. The Brazilian Penal Process11 (1941) on the article 158 states that when the infraction leaves traces, direct or indirect crime examination is essential, not being able to make up for the defendant confession. The article 162 affirms that legal necropsy must be performed at lest 6 hours after death, except when the examiner do not consider this time11. The Medical Ethical Code16 (1996) in articles 114 and 115 forbids the doctor to claim death without her/his personal confirmation. The personal information even of great competence is not enough. It cannot be done in case of violent death or suspect of violence. Final considerations Pereira17 (2005) inquires about what is death consisted of. He states that the moment of death was the total cease of the great functions of the body: absence of heart beat, end of respiratory movements, and pupil contraction. Nevertheless, if we observe the scientific evolution we can conclude that life is subordinated to brain activity, therefore it has its end encephalic death. The same author asks: if there is encephalic death, can the integrity of the individual be considered finished and the body unit broken so that its parts can be extracted under scientific, curative and savior? If we consider that science is correct to claim that life ends with encephalic death and if the jurist claims the personality ceases with death (both propositions are totally right), we can say that the answer to first question is yes. Therefore, the range of Forensic Tanatology and its relation to two fundamental health areas, Medicine and Dentistry, especially to those professionals working at the expert area can be observed. References
© Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil
The following images related to this document are available:Photo images[os06035f1.jpg] [os06035f2.jpg] |
| |||||||||

{kind=link}
{kind=link}