 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 5, No. 19, October-December 2006, pp. 1203-1208 Electromyographic analysis of the upper lip in nose and mouth breathers Michelle Santos Vianna-Lara* , Paulo Henrique Ferreira Caria** * Dental Branch Pontifical Catholic
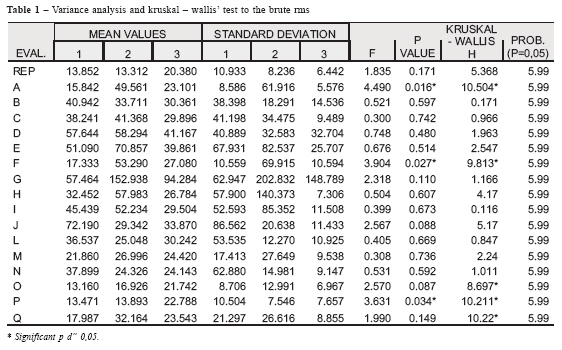
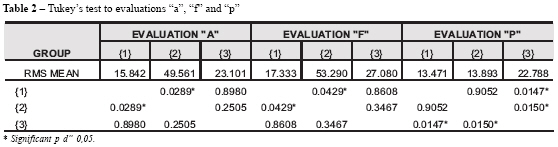
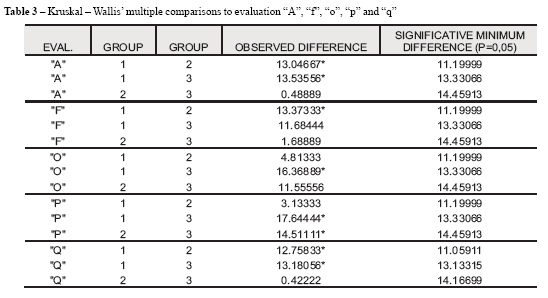
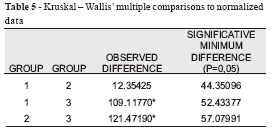
University of Paraná, Brazil Received for publication: June 06, 2006 Code Number: os06036 Abstract The purpose of this research was to compare the electromyographic (EMG) activity of the superior belly of orbicularis oris muscle between individuals with Class II Division 1 malocclusion, nose breathers (Group 1) and mouth breathers (Group 2), having as a comparative parameter a control group of individuals with clinically normal occlusion (Group 3). The EMG recordings were obtained in resting position and in 16 movements. A statistically significant difference between Groups 1 and 2 was observed during puffing out with flaccid cheeks, dispelling of the lips' angle and saliva deglutition; between Groups 1 and 3 during puffing out with flaccid cheeks, posterior right and left clenching and saliva deglutition; between 2 and 3 during posterior right and left clenching. According to the normalized data the malocclusion groups (Groups 1 and 2) have a similar muscle behavior but when they are compared with the normal occlusion group there was a statistically significant difference between them. It can be concluded that, for this sample, the breathing mode did not influence the muscular behavior of the subjects with Class II division 1 malocclusion and that subjects with normal occlusion have more competent lips than the ones with Class II division 1 malocclusion. Key Words: electromyography, facial muscles, mouth breathing, malocclusion Introduction Nasorespiratory function and its relation with craniofacial growth and orofacial muscle activity has been a topic of great interested for at least a hundred years. The modification of this function by a nasal airway obstruction or simply by mouth breathing habit has been associated with morphologic variations of the craniofacial complex, abnormal muscle function and malocclusions1-3. The open mouth posture with or without documented airway patency may be a potentially undesirable factor in dentofacial development4 and its association with mouth breathing can lead to various muscle alterations5-7 resulting in malocclusions and in facial growth alterations1,5-6. In 1899, Angle8 associated the Class II malocclusion with the mouth breathing. Although Ung et al.3 observed a tendency for the development of Class II malocclusion in mouth breathers; other authors reported that patients with mouth breathing are not limited to one specific malocclusion. Schlossberg9 considered that muscle physiology was the main etiologic factor of the Class II malocclusion. Concerning to the etiology of malocclusions, the effect of surrounding soft tissues is a controversial subject. Thereby, assuming that mouth breathing disturbs the balance of the facial muscles and that this imbalance can influence the occlusion, it becames necessary to use a tool, such as electromyography, to diagnose such muscles alterations. By this way, this study aimed to compare the electromyographic (EMG) activity of the upper lip, between individuals with Angle Class II Division 1 malocclusion, nose and mouth breathers, having as a comparative parameter a control group of individuals with clinically normal occlusion. Material and Methods The conduction of this study followed the requirements of the Ethical Committee in Research of the Pontifical Catholic University of Parana. The volunteer participation was possible after explanations regarding the research and of the express agreement of the responsible ones, which was given by the signature of a written consent form. A total of forty-eight general population volunteers, aged between 11 and 14 years old, were enrolled in this study. They were separated into two groups with Angle Class II Division 1 malocclusion and one with clinically normal occlusion: Group 1: composed of 25 subjects with Class II Division 1 malocclusion and predominantly nose breathing (NB). Group 2: composed of 14 subjects with Class II Division 1 malocclusion and predominantly mouth breathing (MB). Group 3: composed of nine subjects with clinically normal occlusion (NO). All individuals had bilateral angle class II (Groups 1 and 2) or class I (Group 3) first permanent molar relationship, absence of anterior or lateral crossbite, no cast restorations and cuspal coverage and no previous orthodontic treatment. The breathing mode evaluation was performed in four steps: (1) a questionnaire answered by the parents with questions related to the mode of breathing, (2) mouth posture observation performed by a dentist, (3) an ear, nose and throat exam and (4) a speech and language evaluation. Electromyographic activity was recorded using one of eight channels of an instrument (EMG System do Brasil, São Paulo SP, Brasil). The analogic electromyographic signal was amplified, digitized and digitally filtered. The instrument was directly interfaced with a computer that presented the data graphically and recorded them on magnetic media for further quantitative and qualitative analyses. To reduce the impedance, the subjects' skin was carefully cleaned prior to the electrodes placement, and recordings were performed 5-6 min later, allowing the conductive paste to adequately moisten the skin surface. During test, disposable silver monopolar electrodes of 10 mm diameter and an inter-electrode distance of 15 mm were used, on each side of the medium line of the upper lip, while a reference electrode was applied to the individual' wrist. The volunteers were examined sitting with their head oriented according to Frankfurt's plane, parallel to the ground. The EMG recordings of the orbicularis oris (superior belly) muscle were obtained in rest position (REP) and in 16 movements, such as: puffing out with flaccid cheeks (A), puffing out with stretched cheeks (B), sucking (C), reciprocal compression of the lips (D), compression of the lips against the teeth (E), dispelling of the lips' angle (F), pursing the lips (G), maximal opening of the mouth (H), pronouncing "ême" (I), "pê" (J), "bê" (L), right (M) and left (N) chewing, posterior right (O) and left (P) clenching and saliva deglutition (Q). Orthodontic elastics (1/2" x 1,5 mm) were used to the chewing and clenching evaluations. All the movements were previously practiced by copying the observer and during the emg exam, the examiners were blinded to the volunteers' mode of breathing. The EMG data was submitted to statistical analysis twice: first the EMG signal was simply processed as RMS (mV) and each evaluation was analyzed separately; second, the EMG signal was processed and normalized by the peak EMG value to evaluate the muscle activity as a whole. Variance Analysis and Kruskal-Wallis tests with a 95% confidence level were used to verify the existence of differences between the values of EMG activity for each evaluation. When differences were observed, Tukey's test and Kruskal-Wallis multiple comparisons, respectively, with the same level were applied. Differences among the groups were considered when these differences were higher than 5%. Results Tables 1 and 4 show the variance analysis and Kruskal-Wallis' test to the brute RMS and normalized data, respectively. Differences among the groups were considered when these differences were higher than 5%. Data analyzed by Tukey's test showed differences between nose and mouth breathers to the following evaluations: puffing out with flaccid cheeks (A) and dispelling of the lips' angle (F). When posterior left clenching (P) was analyzed, the differences observed were between the Class II malocclusion individuals (Groups 1 and 2) and the normal occlusion ones (Group 3) (Table 2). Data analyzed by Kruskal-Wallis confirmed Tukey's test when considering "A" (puffing out with flaccid cheeks), "F" (dispelling of the lips' angle) and "P" (posterior left clenching) evaluations. Besides that, the analyzed data showed difference between Groups 1 and 3 to the "A" (puffing out with flaccid cheeks) and "O" (posterior right clenching) evaluations. When saliva deglutition (Q) movement was analyzed, it was observed difference between Groups 1 and 2; and between 1 and 3 (Table 3). According to Kruskal-Wallis Multiple Comparisons (Table 5) there is a statistically significant difference between the groups with malocclusion (Groups 1 and 2) and the group with clinically normal occlusion (Group 3). Discussion Patients with Class II malocclusion seem to demand greater muscular effort than patients with normal occlusion, in order to perform the movements required10-11. Probably it is related to the malocclusion characteristics such as proclination of the upper incisors associated with a disharmony in the antero-posterior relation between the jaws. These characteristics could hamper the performance of the peribuccal muscles basic functions. In this study, it could not be observed significant statistical differences between the malocclusion groups (Groups 1 and 2) and the clinically normal occlusion group (Group 3) for the majority of the evaluated situations, when the brute RMS was analyzed. Otherwise, analyzing the normalized data, it could be noticed difference between these groups. The higher muscle activity observed in normal occlusion can be explained by the large size of the tooth contact area - more pairs of teeth in contact12. The reduced activity of the upper lip observed in individuals with Class II malocclusion can be related to the unstable intercuspidation observed in this malocclusion, characteristic that can cause the hipotonicity of the upper lip12. If the groups with malocclusion (NB versus MB) are analyzed separately, it can be observed that the mouth breathing group presents higher brute RMS mean values only in three evaluated situations: "A" (puffing out with flaccid cheeks), "F" (dispelling of the lips' angle) and "Q" (saliva deglutition). The muscle imbalance supposedly caused by mouth breathing hampers only some basic functions, which are performed with greater muscular effort. According to normalized data, there is no significant difference between the groups with malocclusion (NB versus MB). It can be suggest that the EMG activity of this muscle is more related to the characteristics of malocclusion than to the breath mode. Subjects with nose (Group 1) and mouth (Group 2) breathing had similar brute RMS mean values at rest position. Silva et al.13 did not observe this similarity and related a great activity of the orbicularis oris for mouth breathers. This greater activity could be related with dental, skeletal and muscular alterations caused by mouth breathing, limiting the ability of these individuals to keep the lips sealed. Schievano et al.14 observed that mouth breathers recruit a greater number of motor units to close the lips, because of a possible muscular hypofunction. In all probability, if we had evaluated the rest position in two situations, with relaxed musculature and requested joint lip, some difference would be expected between nose and mouth breathers during the rest with sealed lips. Besides the possible alterations caused by the open mouth posture, the characteristics of this malocclusion and the breath mode would hamper the maintenance of the closed lips. In the movements of sucking (C), reciprocal compression of the lips (D), compression of the lips against the teeth (E) and pursing the lips (G), the three groups presented the highest RMS mean values of all evaluated movements (Table 1). This was expected since in these situations the muscle is more required. There was no difference between NB and MB for these movements as well as between the malocclusion groups and normal occlusion group agreeing with recordings of previous investigators11 that evaluated the following movements: reciprocal compression of the lips and pursing the lips. The similarity of the statistical values between the three groups suggests that independent of malocclusion or alteration in the breath mode, there is no musculature compromised to produce these movements. However, Tosello et al.11 have observed differences between individuals with Class II division 1 malocclusion and with normal occlusion during compression of the lips against the teeth. The difference observed by these investigators may be attributed mainly to biologic intra-individual variation to perform the task. When posterior right (O) and left (Pa) clenching movements were evaluated, besides the difference observed between the malocclusion groups and normal occlusion group, it was noted a tendency to perform clenching with lower activity of the upper lip by individuals with Class II division 1 malocclusion. Although the peribuccal and masticatory muscles present distinct nerve terminations, the individual reflex in the clenching movement can lead to a contraction of the peribuccal musculature. On this way, the lowest mean values observed in the groups with malocclusion may be related to the hipofunction of this musculature in these individuals. The contraction of the peribuccal muscles, during deglutition, has been considered a typical sign of atypical deglutition. However, Graber15 could not establish a cause and effect relationship between the muscular and bone structures involved in deglutition. Although it was believed that the muscular behavior of Groups 1 (CLII,1 RN) and 2 (CLII, 1RB), in this condition, would be similar because of the intrinsic characteristics of the malocclusion, the results of this study showed that the individuals that breath predominantly through the mouth need a stronger muscular effort to perform this task. However, when comparing the behavior of group 2 (CLII,RB) with group 3 (ON), no statistically significant difference was noticed between them. The proximity of the values between these groups indicate that patients with class II division I malocclusion and mouth breather do not necessarily present atypical deglutition (characterized by the contraction of peribuccal muscles).Theses result are in accordance with the ones observed by Ahlgren et al.12 when compared individuals with Class II division I malocclusion and with normal occlusion. Jacobs16, in 1969, related his anxiety in being able to classify the muscular pattern as it is done following the skeletal and dental patterns. He believed that it was possible to find out that, individuals with Class II division I malocclusion, associated or not to a Class II skeletal pattern, could present a Class II muscular pattern. In light of the results discovered in this study it is believed that such a relationship cannot be established because it is very difficult to determine a pattern of muscular behavior in function of the type of occlusion and any type of alteration of the breath mode, especially because of the great variety of inherent characteristics of each individual in isolated evaluations. The normalization of the signals aims to decrease the influence of the countless variables. The information resulting from this process produces more faithful information of the muscular behavior pattern of the individuals in reference to a higher or lower usage of the muscular fibers in relation to a reference value of the individual himself. On this way, it is believed that the muscular evaluation should be performed in an individualized manner, respecting the idiosyncrasies of each individual, in a way that the goals of the treatment are adjusted to the muscular behavior, just as the positioning of the lower incisors are adapted to the skeletal pattern. It can be concluded, to this sample, that the breath mode has none influence on muscular behavior of the subjects with Class II division 1 malocclusion according to the brute RMS and normalized data. Beside, subjects with clinically normal occlusion have more competent lips than the ones with Class II division 1 malocclusion according to the normalized data. Acknowledgements Supported by "Coordenação de Aperfeiçoamento de Pessoal de Nível Superior" CAPES, Brazil. References
© Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06036t1.jpg] [os06036t2.jpg] [os06036t4.jpg] [os06036t3.jpg] [os06036t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}