 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
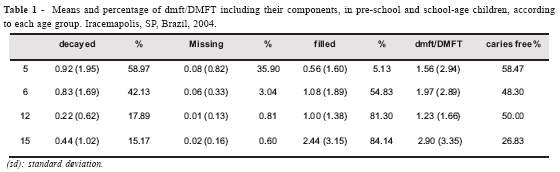
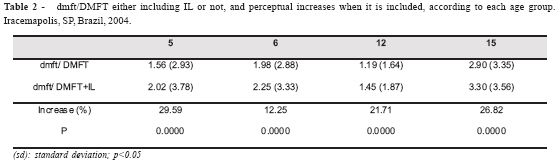
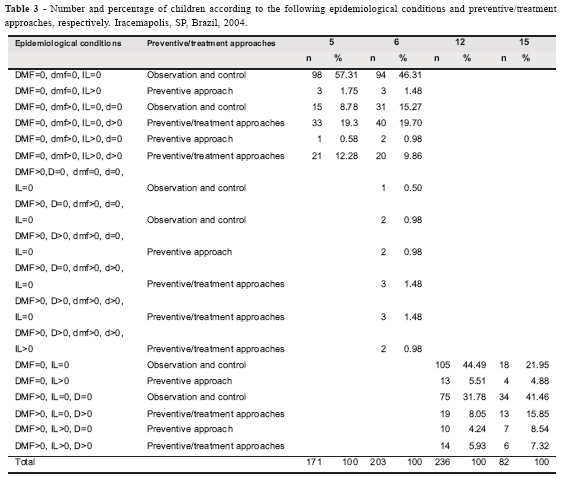
Brazilian Journal of Oral Sciences, Vol. 5, No. 19, October-December 2006, pp. 1217 - 1222 Influence of initial carious lesions on oral health planning Andrea Videira Assaf* , Cristiana Tengan** , Elaine Pereira da Silva Tagliaferro** , Zuleica Pedroso Meneghim*** , Marcelo de Castro Meneghim** , Antonio Carlos Pereira** , Gláucia Maria Bovi Ambrosano** *Department of Community Services Fluminense Federal University, Niterói, RJ, Brazil Received for publication: April 18, 2006 Code Number: os06039 Abstract The aim of this cross-sectional study was to verify the importance of including initial carious lesions (IL) in the oral health planning of a public health service. The sample comprised 692 schoolchildren at the ages of 5 (n=171), 6 (n=203), 12 (n=236) and 15 (n=82), enrolled in state schools in Iracemapolis, SP, Brazil. Clinical examination was performed, using dental mirror and CPI (Community Periodontal Index) probe, after tooth brushing and drying. Two diagnostic thresholds were used for measuring the outcome: diagnostic threshold based on cavitated lesions and diagnostic threshold based on the inclusion of IL. The mean value for dmft was 1.56 for 5-year-olds and 1.98 for 6-year-olds. The mean value for DMFT was 1.19 for the age of 12 and 2.90 for the age of 15. The dmft and DMFT indexes increased significantly for all ages (paired t test, p<0.05) when IL was included in the examinations (29.59%, 12.25%, 21.71%, 26.82% for the ages of 5, 6, 12 and 15, respectively). The inclusion of IL in surveys generated a statistically significant percent increase in caries indexes for all age groups, contributing to obtain additional information for oral health planning in public services. Key Words: epidemiology, dental caries, diagnosis Introduction The pattern of dental caries has undergone profound changes in high-income countries over the last few decades, having shown drastic decrease in prevalence and incidence of the disease and consequently, increasing numbers of caries-free children1-2. Several factors have been pointed out, which could have contributed to this change. Although factors like fluoridated water, preventive programs, oral hygiene, reduction in sugar consumption and others have been indicated as possibilities, most of the studies have considered the dissemination of fluoridated dentifrices as being the most important one1-2. Consequently, there has been a larger number of initial lesions (IL), a reduction in cavitated carious lesions and predominance of activity on the occlusal surfaces3-7. These modifications in the pattern of dental caries are very relevant, not only for clinicians, but also for epidemiologists and oral health service planners. The scientific literature has discussed the methodologies of epidemiological studies, which use diagnostic criteria/thresholds that consider caries as a cavitated lesion, e.g., the WHO diagnostic criteria8. The argument is that these studies have underestimated dental caries in populations/groups, since initial lesions have been more prevalent than cavitated lesions, particularly in low prevalence groups3,5,9-10. The aim of this cross-sectional study was to verify the importance of including IL in the oral health planning of a public health service, which is focused on groups with low and moderate caries prevalence. Material and Methods Approval was obtained from the Ethical Committee in Research at the Piracicaba Dental School/UNICAMP (State University of Campinas), Protocol No. 209/2004, in agreement with Resolution 196/96 of the National Committee of Health/Health Department (BZ). The schools granted permission for the study and informed consent was obtained from the parents. General Aspects of the Town Iracemapolis is situated in São Paulo state and has a total of 17,506 inhabitants11. The city has had fluoridated water since 1997 (0.7 ppmF) and presented a DMFT of 2.1 for the 12-year-old group12. Sample Six hundred, ninety-two schoolchildren, of whom 171 were 5-year-olds, 203 were 6, 236 were 12 and 82 were 15-year-olds, participated in the study. This sample represented all pre-school and school-age children in state schools of Iracemapolis, except those children who study at night. Children with local or general problems, such as the use of a fixed orthodontic device, severe fluorosis and hypoplasia, or a serious systemic disease were excluded from the sample. Diagnostic codes and criteria and diagnostic thresholds used for assessment The criteria and codes were those based on the WHO8 recommendations. For the IL, active caries with intact surfaces were recorded - an adaptation of the criteria according to Nyvad et al.13 and Fyffe et al.14. Thus, an IL (initial lesion) was defined as active caries which, through visual assessment by a calibrated examiner, indicated an intact surface, no clinically detectable loss of dental tissue, with a whitish/yellowish colored area of increased opacity, rough, with loss of luster and presumed to be carious (when the CPI probe is used, its tip should be moved gently across the surface). Smooth surface: caries lesion typically located close to gingival margin. Fissure/pit: intact fissure morphology: lesion extending along the walls of the fissure. In this study, localized surface defects (active microcavities) restricted to enamel only were included in the IL group. Active white spot lesions and microcavities contiguous to sealants, restorations and cavitations were also recorded. Two diagnostic thresholds were used: WHO8 diagnostic threshold, in which caries is considered a cavitated lesion, and WHO+IL diagnostic threshold, including active ILs. Examiner Training and calibration Four examiners with previous experience in epidemiological surveys participated in the study. The calibration process began with a theoretical phase in order to verify examiners' knowledge about epidemiological diagnosis, according to WHO8 and for the purpose of initial standardization, to measure the examiner's ability of diagnosing IL, mainly focused on the clinical characteristics, according to the location. After that, clinical training sessions were held with discussions among the examiners and the benchmark examiner, with regard to clinical diagnosis, codes and criteria used, recording and other errors. Following the clinical training exercises, the examiners undertook two calibration exercises, which generated mean inter-examiner Kappa values of 0.88 for the WHO+IL diagnostic threshold and 0.95 for the WHO diagnostic threshold. The total time for the entire calibration process was 28 hours. During the examinations, the 4 examiners re-examined 10% of the sample for each age group in order to verify the intra-examiner error8. Mean Kappa values of 0.96 for the WHO diagnostic threshold and 0.89, for the WHO+IL threshold were obtained during this phase. Epidemiological examinations Supervised tooth brushing was done with fluoridated dentifrice for a standardized time of 2 minutes, according to the modified Bass technique, before the individuals were examined. After that, children were taken for examination, performed in outdoor setting. All examinations were carried out by the 4 examiners, helped by dental nurses, under the following conditions: natural light, use of dental mirror and ball-ended CPITN probes with a diameter of 0.5mm (for removing debris, assessing presence of fissure sealants and, in case of doubt, to check the surface texture of IL) and dental drying. During the examinations, prior dental drying was carried out for about 5 seconds per tooth with the use of compressed air through a dental compressor (Proquest Delivery System, model 4010, Compressor Technologies LTD, Englewood, USA). Statistical analysis For the analysis of the results dmft and DMFT were employed for primary and permanent teeth, respectively. The Bioestat 3.0 statistical program and paired t-test were used to verify the statistical significance of the percent increases when including IL (p<0.05). Results Table 1 shows that dmft for 5 and 6-year-olds was 1.56 and 1.97 respectively, representing a low caries prevalence. DMFT for the 12-year-old children was 1.23 and 2.90 for the 15-year-olds, showing a percent increase of 135.77. Except for the 15-year-old group, a high percentage of "caries free" children, with percent ranges between 48.30 and 58.47%, was observed. The distribution of each component of the caries indexes showed that the filled component was the most relevant for the ages of 6, 12 and 15 years, while for the 5-year-old children, it was the decayed component. When including IL in caries indexes, percent increases from 12.25 to 29.90%, which were all statistically significant, were verified for all age groups (p<0.05) (Table 2). Table 3, which aimed to show the importance of IL inclusion in oral health planning surveys, showed a few examples of possible epidemiological conditions found among the age groups, associated with their respective indications for preventive/treatment approaches. Except for the 15-year-old group, around 50% of the children were "caries free", with only periodic observation and control being recommended. In general, a small increase between 1.48 and 4.51% of children presenting only initial carious lesions was found, and preventive strategies were indicated. On the other hand, there was a larger group of children (between 5.93 and 12.28%) found to have cavitated lesions (decayed component>0) and IL in both dentitions, and restorative associated with preventive approaches were recommended. Discussion Epidemiology, together with biological sciences, has been important for analyzing and understanding different diseases, in order to generate knowledge to control or eradicate them by means of therapeutic approaches. Epidemiological surveys are relevant strategies that generate future information about health-disease processes in a population. Dental caries has been analyzed through surveys performed around the world for decades2. Up to the present time, epidemiological data have been poorly used for planning dental health services and when they are used, most of them generate information according to the diagnostic threshold with cavitation being considered as caries lesions. The literature has shown that by considering the diagnostic threshold on the basis of cavitated lesions does not inform epidemiologists and health planners about which lesions/individuals need preventive and non-invasive treatment. Thus, health services are still treating dental caries as a cavity and not as a multifactorial disease, which clinically presents evident initial signs of enamel demineralization15-16. Nowadays, a large number of researchers, like Pitts and Fyfee3, Sköld et al.9, Amarante et al.10 and Assaf et al.17 have shown some need and justification for including IL in epidemiological surveys3,9-10,17. One of the reasons is that there has been an even higher prevalence of IL than of cavitated lesions, particularly in low caries prevalence areas. Therefore, its inclusion would contribute to a decrease in the level of underestimating the disease, and would provide a better classification of dental caries levels in the population 6. On the other hand, it has been alleged that IL is difficult to be diagnosed correctly, mainly in surveys and the benefits derived from the extra information may be outweighed by increased examiner and method error6,15-16,18. Moreover, the use of less sensitive criteria is also justified by the fact that restorative intervention is usually carried out at the dentin cavitation stage8. However, the scientific literature has shown the real possibility of using more sensitive dental caries criteria. Clinical trials19-21, cross sectional surveys and studies of dental caries calibration13-14,17-18,22 have demonstrated substantial to high levels of inter- and intra-examiner reliability at more sensitive diagnostic thresholds. In agreement with previous studies3,9-10,17, the present study showed evidence, for all age groups, that percent increases in caries indexes, which were 29.59% for the 5-year-old children, 12.25% for the 6-year-olds, 21.71% for the 12-year-olds and 26.82% for the 15-year-olds, were verified when IL was included in the examinations. Dental health programs that focus only on the treatment of cavitated lesions are not enough to reestablish health in an individual/population because they do not consider the different stages of carious lesion progression. Surveys that include IL could be very relevant to show distinct preventive and operative needs. Table 3 intends to exemplify the importance of surveys in health planning by demonstrating the percentage of children in specific clinical dental health situations, and associating each respective preventive/operative approach with these situations. When observing each age group, it could be noted that 76.27% of the 12-year-old children did not need an individual approach, for this group only periodic educational reinforcement being indicated; preventive strategies associated with educational reinforcement were indicated for the 9.75% who presented only IL; and for the 13.98% of 12-year-olds, operative/preventive approaches were needed, with periodic educational reinforcement. Therefore, this selection and classification according to different procedures, educational-preventive-invasive treatment, could not only help dentists but also generate a better quality of public services, because these dental approaches would be linked to the individual's priorities and risk of caries. On the other hand, the additional costs incurred by implementing these measures would be offset by the better performance of the service; more detailed health planning would lead to optimization of time spent on individual attendance and consequently increase the productivity of the service. Therefore, at the present time, it is necessary to make epidemiological changes, in the light of the development of epidemiological surveys to evaluate the prevalence of IL in different groups, and studies capable of analyzing the costs for adopting this new measure, which uses additional diagnostic adjuncts, like brushing and drying during examinations. Furthermore, there is need for a new consensus among the scientific community, about the epidemiological diagnosis of dental caries. Epidemiological criteria, with the inclusion of IL, diagnostic examination adjuncts, and the calibration process for examiners need to be standardized, and would be important aspects for conducting future epidemiological and clinical studies that could be properly compared6,15-16. Acknowledgements The authors wish to thank the teachers, students, and directors of João Hometo and Cesarino Borba state schools and all the state preschools in Iracemapolis for their valuable participation in this study. References
© Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06039t2.jpg] [os06039t3.jpg] [os06039t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}